
Abstract
Abstract
Background:
Numerous studies have reported the associations between the type of feeding during infancy and subsequent chronic diseases.
Objective:
The objective of this systematic review is to synthesize the available literature concerning the effect of breastfeeding in infancy on physical and cardiorespiratory fitness in children and adolescents.
Materials and Methods:
We performed a comprehensive search of medical bibliographic databases to identify observational studies reporting the association between breastfeeding and cardiorespiratory or physical fitness. Random effects model was used for calculating the pooled estimates.
Results:
Three studies with 2,792 children were included in the meta-analysis. The mean value of VO2max was similar between formula-fed and 1–3 months breastfed participants (standardized mean difference [SMD]: 0.1, 95% confidence intervals [CI]: −0.09 to 0.29, p = 0.31). There was no difference between 3 and 6 months breastfed (SMD: 0.17, 95% CI: −0.01 to 0.35, p = 0.06), >6 months breastfed (SMD: 0.37, 95% CI: −0.03 to 0.78, p = 0.07), and formula-fed children. The pooled SMD in handgrip strength was 0.09 (95% CI: −0.04 to 0.23; p = 0.17) between 1 and 3 months breastfed and formula-fed children .Nevertheless, 3–6 months (SMD: 0.13; 95% CI: 0.03–0.24) and >6 months (SMD: 0.19; 95% CI: 0.01–0.37) breastfeeding was associated with higher handgrip strength compared with formula-fed children. Breastfeeding for 1–3 (SMD: 0.20; 95% CI: 0.12–0.28), 3–6 (SMD: 0.27; 95% CI: 0.18–0.37), and >6 months (SMD: 0.34; 95% CI: 0.11–0.58) led to a significantly higher standing long-jump performance compared with formula feeding.
Conclusions:
Breastfeeding shows beneficial effects on physical fitness, but further well-designed studies need to clarify effects of breastfeeding on cardiorespiratory fitness.
Introduction
C
The role of nutrition in the prevention of chronic diseases, including CVD, has been shown since the early stages of life. 4 One of the key factors in early life nutrition is breastfeeding. It has been shown that breastfeeding plays an important role in adulthood health by preventing noncommunicable diseases. As mentioned previously, breastfeeding has been shown to be effective in the prevention of CVD in adulthood. 5 Moreover, various studies have been accomplished about the effect of breastfeeding on cardiorespiratory fitness in children and adolescents. Although some of these studies have not detected any traces of benefit in this regard, others have shown that breastfeeding improves cardiorespiratory fitness.6–8 Since cardiorespiratory fitness is affected by many factors throughout life, it is best to look at this relationship early in life. Therefore, according to the results of studies conducted in this field, this systematic review and meta-analysis has sought to review and summarize the effect of breastfeeding on physical and cardiorespiratory fitness in children and adolescents.
Materials and Methods
Literature search strategy
The present study followed the guidelines recommended by the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols. 9 We systematically searched all published original articles, letters, abstracts, and review articles about infant feeding and cardiorespiratory and physical fitness by using the EMBASE (1980 onward), PubMed (1966 onward), Scopus (1995 onward), and Web of Science (1980 onward) bibliographic databases. Relevant references were identified using a combined text word and MeSH heading search strategy. We reviewed the reference lists of identified articles and hand-searched reviews, bibliographies of books, and abstracts. Also, we checked the citation lists of relevant publications. We also contacted experts and specialists in the field for possible unpublished research on the topic and additional relevant citations. No further limitations were made to be as sensitive as possible. The search was modified for Web of Science, EMBASE, and Scopus using their subject headings instead of the MeSH subject headings. Our review was restricted to human subjects. Search details are available in Appendix 1.
Study selection criteria
The review included English-written epidemiologic (case–control, cohort, and cross-sectional) studies of the association between breastfeeding and cardiorespiratory fitness. Articles would be included if they fulfilled the following criteria: (1) breastfed infants compared to infants fed with formula (2) cardiorespiratory and physical fitness parameters compared between breastfed infants and formula-fed infants as outcome measurements, and (3) articles which categorized breastfeeding as a category variable.
Data extraction
Each of the relevant articles identified through the search strategies was reviewed by at least two of the authors by using a standardized report form based on (1) study design, (2) target population, (3) sample size/power, (4) specific definition of breastfeeding, (5) clear definition of diabetes, and (6) control for confounding variables.
Outcome measures
The primary outcomes; VO2max, handgrip strength, standing long jump, 20 and 40 minutes sprint, sit-and-reach flexibility test, and Flamingo balance were defined as pooled estimates of the mean difference in changes between the means of the breastfed and formula-fed children. The effect was measured as standardized mean difference (SMD) and 95% confidence intervals (CI) between breastfed and formula-fed infants by using the DerSimonian and Laird method, which is based on the random effects model. The results of the included studies were tested for statistical heterogeneity by visual inspection of forest plots, by performing the Q test (assessing the p-value) and by calculating the I 2 statistic. Statistical heterogeneity was considered substantial if the p-value was less than 0.10 or I 2 value exceeded 50%. The statistical analyses were performed using RevMan5 (2008).
Assessment of bias risks and methodologic quality of included trials
Included studies were critically appraised by two independent review authors using a priori criteria based on the Newcastle–Ottawa Scaling for nonrandomized studies. The Newcastle–Ottawa Scale is an ongoing collaboration between the universities of Newcastle, Australia and Ottawa, Canada. It was developed to assess the quality of nonrandomized studies with their design, content, and ease of use directed to the task of incorporating the quality assessments in the interpretation of meta-analytic results. A “star system” has been developed, in which a study is judged on three broad perspectives: the selection of the study groups; the comparability of the groups; and the ascertainment of outcome.
Results
Literature search
The initial literature search identified 1,173 potentially relevant articles: 469 from PubMed, 598 from EMBASE, 52 from Scopus, 45 from Web of Science, and 9 from Cochrane Library. No unpublished studies were found. By reviewing the title and abstracts of the included articles, duplicate studies and nonrelevant studies were removed. Out of the remaining eight articles, three articles were discarded as they did not have a proper control group. Full-text review of the articles revealed that five were potentially relevant to the analysis relating breastfeeding and cardiorespiratory and physical fitness (Fig. 1).
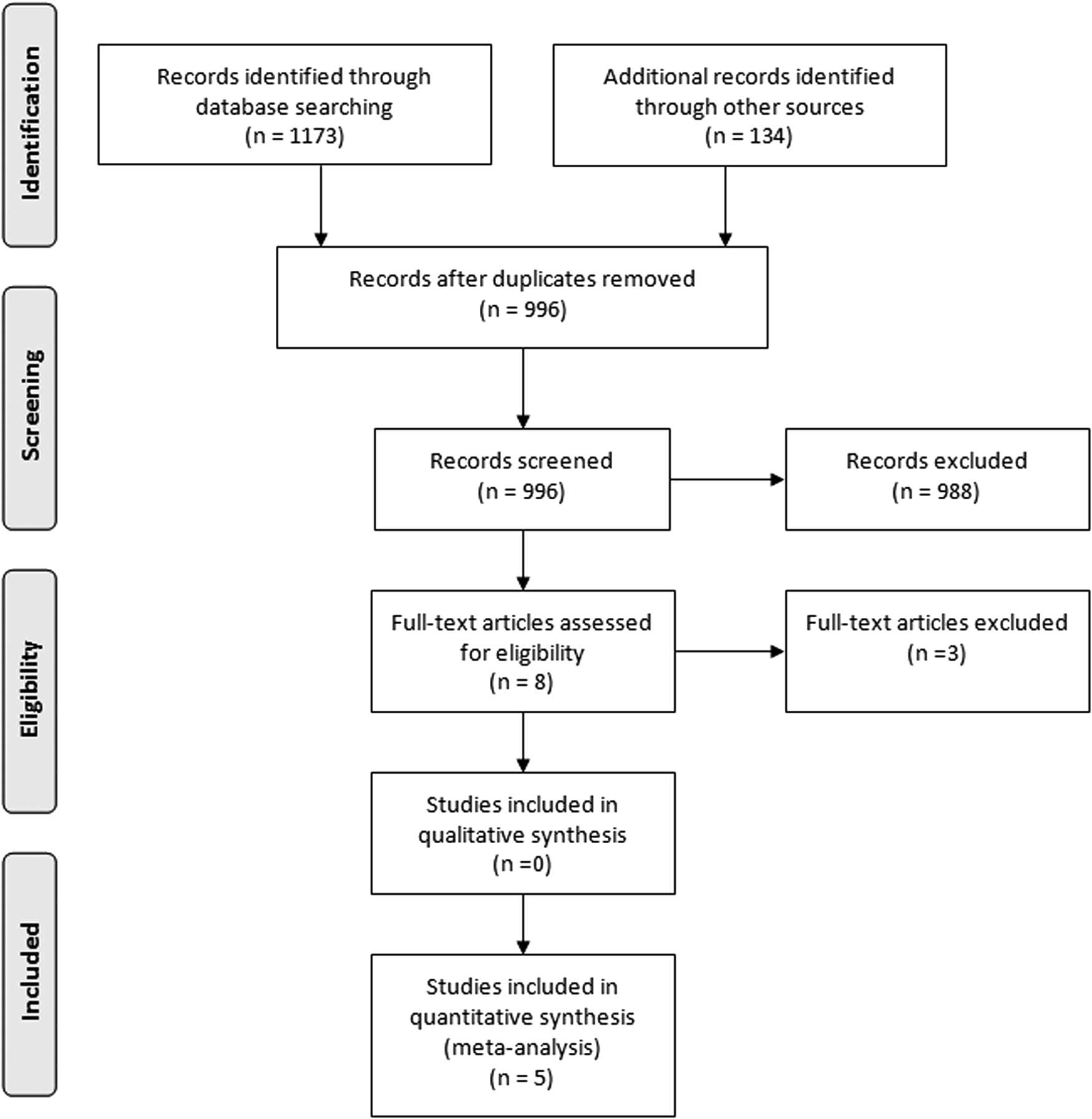
Flowchart of the study selection process.
Summary of study characteristics
Three studies were eligible for the meta-analysis comprising more than 2,792 children included in the final analysis. Two studies reported different outcomes and entered into the qualitative analysis. Characteristics of included studies are presented in Table 1. The publication dates ranged from 2008 up to 2016. Among the 5 studies, 3 were on children aged between 6 and 11, and 2 on children and adolescents (aged between 9 and 17.5). Three studies were based on Europe (including Belgium, Cyprus, Estonia, Germany, Hungary, Italy, Spain, and Sweden), and one study was conducted in England and one study in Iran. Three of the studies had a cross-sectional design; the remaining studies were retrospective cohort studies. The sample sizes varied between 246 and 3,612 participants. Three studies used an ergometer test for assessing cardiorespiratory fitness among children. Two studies used various indices (Handgrip strength, standing long jump, 40-m sprint, sit-and-reach flexibility test, and 20-m shuttle run).In all studies, the breastfeeding variable was categorized into four categories according to the presence and the duration of exclusive breastfeeding: Exclusive breastfeeding (1–3, 3–6, and >6 months) and exclusive formula-fed.
FFM, fat free mass; FM, fat mass; VO2max, maximal oxygen consumption, M, male; F, female.
There were four studies classified as good and one as fair quality. Only one of the five included studies was found to have a moderate risk of selection bias. All studies provided adequate criteria for diagnosis of the outcomes of interest and provided a proper description of how the outcomes were measured. All studies reported that cases and controls were selected from the same community sample. Comparability of participants on the basis of potential confounders was addressed in all studies (Appendix Table AT1).
Summary of study results
Cardiorespiratory outcomes
VO2max
We found three studies in which VO2max was compared between exclusive breastfed and formula-fed children.10–12 In a random effects model, including three studies, the mean value of VO2max was similar between formula-fed and 1–3 months exclusive breastfed participants (SMD: 0.1, 95% CI: −0.09 to 0.29, p = 0.31; I2 = 76%). Also, there was no difference between 3 and 6 months exclusive breastfed (SMD: 0.17, 95% CI: −0.01 to 0.35, p = 0.06; I2 = 73%), >6 months exclusive breastfed (SMD: 0.37, 95% CI: −0.03 to 0.78, p = 0.07; I2 = 90%), and exclusive formula-fed children (Fig. 2).
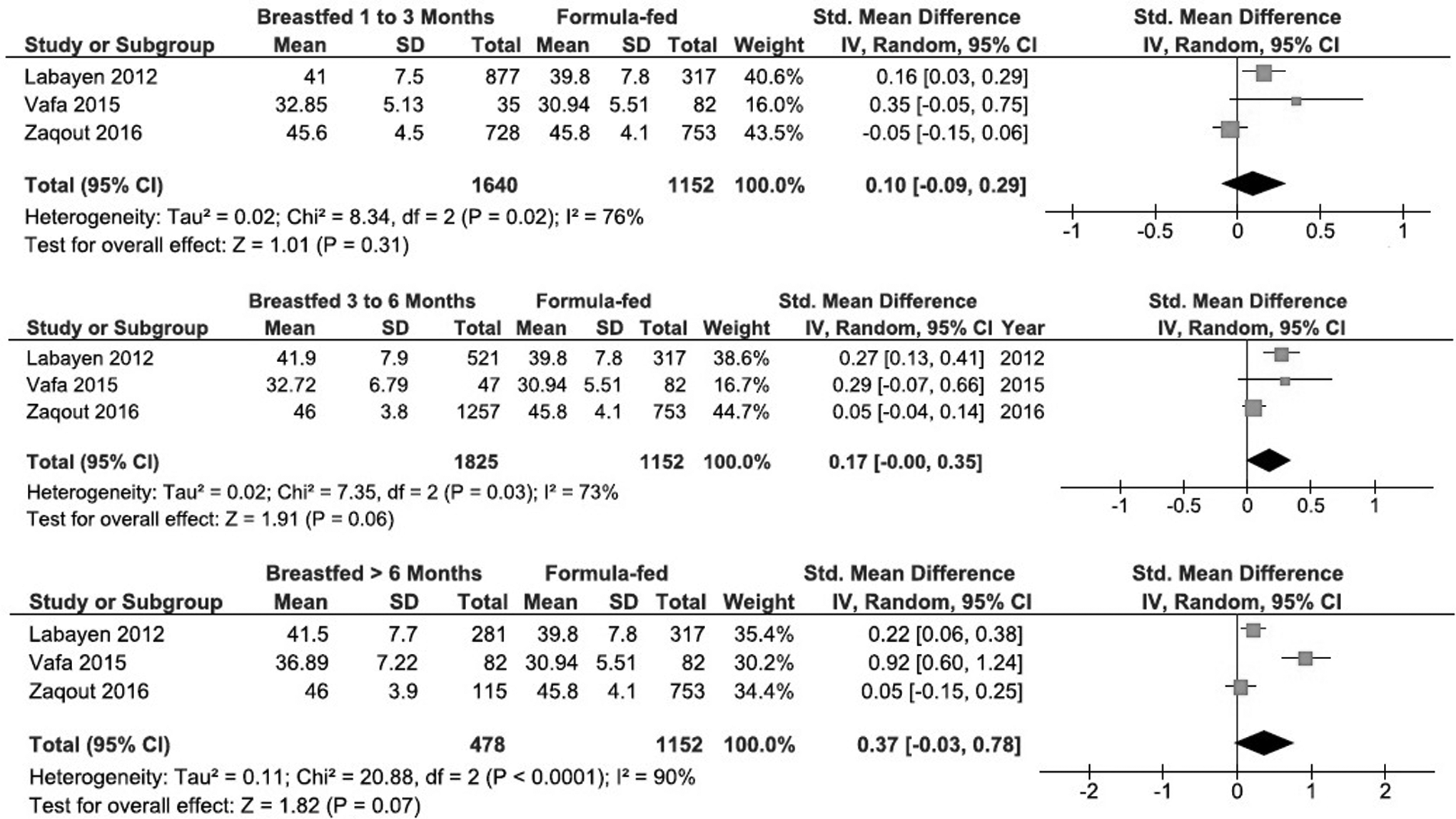
Forest plots of meta-analysis results presented, as pooled standard mean differences with 95% CIs for changes in Vo2max, between formula-fed and 1–3 months exclusively breastfed, between formula-fed and 3–6 months exclusively breastfed, between formula-fed and >6 months exclusively breastfed. CI, confidence intervals.
Handgrip strength
Two studies used the handgrip strength to compare children's physical fitness; both studies did not show a significant association. In a study by Artero et al., in 2010, a total of 2,567 adolescents (1,426 girls), who were recruited from the Healthy Lifestyle in Europe by Nutrition in Adolescence (HELENA) cross-sectional study, aged 12.5–17.5 years were included. 13 In the crude analyses, as well as in the adjusted models, the duration of any breastfeeding was not associated with the handgrip strength in both boys and girls. In boys, the mean of handgrip strength was similar between formula-fed (mean: 36.0 95% CI: 35.1–36.9), 1–3 months breastfed (mean: 35.8 95% CI: 35.2–36.5), 3–6 months breastfed (mean: 35.8 95% CI: 35.1–36.5), and >6 months breastfed children (mean: 36.6 95% CI: 36.0–37.3) (p = 0.238). Also in girls, the mean of handgrip strength was similar between formula-fed (mean: 26.0 95% CI: 25.5–26.5), 1–3 months breastfed (mean: 25.7 95% CI: 25.3–26.2), 3–6 months breastfed (mean: 26.3 95% CI: 25.8–26.8), and >6 months breastfed children (mean: 26.4 95% CI: 26.0–26.8) (p = 0.138). Similarly, Zaqout et al. demonstrated no differences between the mean of handgrip strength in formula-fed, 1–3 months breastfed, 3–6 months breastfed, and >6 months breastfed children; the results were adjusted for related confounders in mixed model regressions (p = 0.312). 12 Combining the two studies showed a pooled SMD in handgrip strength of 0.09 (95% CI: −0.04 to 0.23; p = 0.17; I2 = 66%) between 1 and 3 months exclusive breastfed and formula-fed children (Fig. 3). Nevertheless, 3–6 months (SMD: 0.13; 95% CI: 0.03–0.24, I2 = 50%) and >6 months (SMD: 0.19; 95% CI: 0.01–0.37, I2 = 60%) exclusive breastfeeding were associated with higher handgrip strength compared with formula-fed children.

Forest plots of meta-analysis results presented as pooled standard mean differences with 95% CIs for changes in handgrip strength, between formula-fed and 1–3 months exclusively breastfed, between formula-fed and 3–6 months exclusively breastfed, between formula-fed and >6 months exclusively breastfed. CI, confidence intervals.
Standing long jump
There are three studies in which standing long jump were compared between exclusive breastfed and formula-fed children. Artero et al. revealed that those adolescents who were breastfed for 3–5 or >6 months showed a lower risk of having a standing long jump performance below the 5th percentile compared with those who were never breastfed (odds ratio [OR] = 0.54, 95% CI = 0.30–0.96, p < 0.05; and OR = 0.40, 95% CI = 0.22–0.74, p < 0.01, respectively) after adjusting for variables of gender, age, and country. When variables of fat mass, fat-free mass, and height were included in the model, no changes were observed in the results. The percentage of adolescents below the 5th percentile were 6.3%, 6.7%, 3.7%, and 2.4% for those adolescents who were never breastfed or breastfed for 3, 3–5, and >6 months, respectively. 13 In a study by Zaqout et al., it was found that there was a positive effect of breastfeeding on lower-body explosive strength for both boys and girls. This relationship was independent of physical activity and body mass index (BMI) in girls. This association was significant between those who never breastfed and those who breastfed for the first 1–3 or 4–6 months (p = 0.019; p = 0.002), respectively, with a 2 cm further jump distance. They found no significant difference between 1–3 and 4–6 months of breastfeeding. Furthermore, longer breastfeeding durations (7–12 months) did not lead to an extra benefit compared with 4–6 months of breastfeeding. 12
All combined results revealed that breastfeeding for 1–3 months (SMD: 0.20; 95% CI: 0.12–0.28, I2 = 0%), 3–6 months (SMD: 0.27; 95% CI: 0.18–0.37, I2 = 37%), and >6 months (SMD: 0.34; 95% CI: 0.11–0.58, I2 = 76%) resulted in a significantly higher standing long-jump performance compared to exclusive formula feeding (Fig. 4).

Forest plots of meta-analysis results presented as pooled standard mean differences with 95% CIs for changes in standing long jump, between formula-fed and 1–3 months exclusively breastfed, between formula-fed and 3–6 months exclusively breastfed, between formula-fed and >6 months exclusively breastfed. CI, confidence intervals.
Twenty and 40 minutes sprint
Two studies used the sprint run to compare the children's aerobic fitness according to whether they had been breastfed or not. All the studies did not show a significant association between 20 and 40 minutes sprint and breastfeeding status. Zaqout et al. reported no significant difference between formula-fed and breastfed (all categories) children regarding a 40 minutes sprint (p = 0.755). 12 Likewise, Artero et al. reported that in healthy boys, 20-m shuttle run ranged from 6.5 (95% CI: 6.2–6.8) in 1–3 months breastfed to 7.1 (95% CI: 6.7–7.5) in formula-fed boys (p = 0.184).Also in healthy girls, 20-m shuttle run ranged from 3.6 (95% CI: 3.4–3.8) in 1–3 months breastfed to 4.2 (95% CI: 3.9–4.4) in formula-fed (p = 0.003). 13
Sit-and-reach flexibility test and Flamingo balance
We found only one study, which compared flexibility and balance between formula-fed and breastfed children. In a study by Zaqout et al., it was found that there was a positive significant association between exclusive breastfeeding and flexibility. Flexibility was only better (0.3 cm further reach) in those children who had been breastfed 4–6 months, compared with those never breastfed (p = 0.006). However, this association was observed after adjustment for physical activity and BMI.
After splitting for sex, the association was only significant between exclusive breastfeeding and balance. There were positive relationships in girls, but negative associations were found in boys. However, the associations were only significant in 4–6 month breastfed children after further adjustment for physical activity and BMI.
Discussion
In this systematic review and meta-analysis, we investigated the effect of breastfeeding duration on Vo2max as a main factor in physical and cardiorespiratory fitness in young age. No significant effect was detected between both variables. Also, about 20 and 40 minutes sprint, no significant difference was seen between breastfeeding group categories (1–3 month breastfed, 3–6 months breastfed, and over 6 months breastfed) and formula-fed children. However, other physical fitness indices, including standing long jump, sit-and-reach flexibility test, Flamingo balance, and Handgrip strength, were significantly improved in longer periods of breastfed groups. However, the heterogeneity of evidence was high and this relationship had a large number of environmental and genetic confounding factors. Therefore, these results should be declared by caution.
To the best of our knowledge, this is the first systematic review and meta-analysis, which investigated the association between breastfeeding and childhood/adolescent cardiorespiratory fitness. In the context of examining the effects of breastfeeding on cardiorespiratory fitness, other factors affecting cardiorespiratory fitness such as obesity, overweight, blood pressure, and the lipid profile have been systematically reviewed and a meta-analysis has been carried out. 8
The results of this meta-analysis has showed that breastfeeding decreases the possibility of type 2 diabetes and the chance of becoming overweight/obese by 13%. However, no associations were found for blood pressure or total cholesterol. In another systematic review, systolic blood pressure was lower in breastfed children compared with formula-fed subjects. 14 This study, similar to the results of our meta-analysis, also showed that smaller sample sized studies indicated more significant relationships compared to larger studies. 14 However, there was an insufficient consistent evidence that breastfeeding affects all-cause or CVD mortality in earlier systematic reviews and meta-analysis. 5
The heterogeneity of the studies carried out in this meta-analysis can be due to the differences in the study communities along with other confounding factors, such as age and gender. Although age was considered as an inclusion criteria in this systematic review and meta-analysis, there was a large difference between the participants' age of the five studies. Among the five studies which were included in this review, four studies investigated the correlation between breastfeeding and cardiorespiratory fitness,10,11,13,15 whereas two studies investigated physical and muscular fitness.12,13 In the studies which investigated cardiorespiratory fitness, the different results could have been due to different methods used. 16 The gold standard method for evaluating cardiorespiratory fitness is the VO2max assessment, 17 which is used as an assessment tool in a majority of studies.18–20 In this meta-analysis, three studies used VO2max as a predictive factor for cardiorespiratory fitness assessment. Vafa et al. and Labayen et al., used a treadmill and a cycle ergometry, respectively; whereas Zaqout et al. used a progressive 20 m shuttle run test. All the three studies included in this meta-analysis showed that an increase in the breastfeeding duration elevates VO2max; however, this association was not statistically significant. Furthermore, in different breastfed groups a duration-respond effect on VO2max was detected, and in formula-fed groups there was a modest protective effect. The advantages of breastfeeding in this content could be due to special nutrients, such as trophic substances, hormones, and long-chain poly unsaturated fatty acids (LCPUFA), which are not found in formula. Previous studies have shown that LCPUFA has immunomodulatory effects and also improves better growth.21,22 Moreover, the extent of assurance against low cardiorespiratory fitness was bigger when the results were measured in children and adolescents, proposing that the relationship might be weakened after some time. 23 Also, besides VO2max, some other methods were used in literature to assess physical and cardiorespiratory fitness such as handgrip strength, 20 or 40 m run sprint, standing long jump, and sit-and-reach flexibility test. They are usually used as a predictor of physical fitness and muscular strength. In addition, these tests are influenced by other factors such as body weight, so the best way to assess cardiorespiratory fitness seems to be VO2max by means of ergometry. Two studies used physical and muscle strength methods, by Artero et al. and Zaqout et al., a combination of their results in the meta-analysis model showed that handgrip strength as an upper physical fitness increased significantly in children who have been breastfed compared with formula-fed groups. Previous studies also show that breastfeeding improved pincer grip in healthy infants. 24 These two studies12,13 observed that the duration of either exclusive or mixed breastfeeding (breastfeeding and formula-fed in same time) was positively associated with more standing long jump as lower-body explosive strength. Previous studies have also shown that breastfeeding improves motor skills in infants and children who have been breastfed, and they were more likely to be walking by 12 months and crawling sooner. 25 Also another study observed that breastfeeding in early infancy influences walking skills in later infancy and childhood. This could be due to the active ingredients, enzymes, and adipokines in breast milk26,27 compared to formula. 28 One of the main ingredients that may play a fundamental role in muscle and physical strength is insulin-like growth factor 1 (IGF-1). 27 IGF-1 levels are positively associated with energy intake, neonatal protein intake, and muscle and bone growth. 29
It seems that the beneficial effects of breastfeeding on muscle and physical fitness compared to formula, arises from IGF-1.It is notable that Artero et al. and Zaqout et al. also measured sprint run to evaluate physical and muscle fitness, but they used different methods (20 m sprint run and 40 m sprint run, respectively). So we could not include them in meta-analyses. Breastfeeding pattern is different in various countries because of different cultures. 30 Studies in developing countries on the association between breastfeeding and cardiorespiratory fitness shows positive results, and an increase in the duration of breastfeeding has led to a greater increase in cardiorespiratory fitness in childhood. 11 While this association has not been statistically significant in developed countries. However, in a study by Labayen et al., the results were statistically significant, but not clinically significant. 10 This difference seems to be due to the economic conditions governing these countries. In developing countries, due to less economic potentials a breastfed child may profit more health benefits of breastfeeding than a child in developed countries. According to previous studies human milk is less affected by mother's diet. 31 Moreover, in high-income communities in contrast to low- and middle-income communities, breastfeeding is more usual among mothers who have a higher socioeconomic position and are more educated. 32
Other factors such as regular children's exercise programs at schools and child nutrition policy at schools which affect cardiorespiratory fitness also vary between developing and developed countries. 33 The reason for this difference could be due to the different methodological aspects in studies of developed and developing countries. However, the quality assessment of studies also showed a difference between developing and developed studies. In our systematic review, we excluded studies reported as abstracts and conference articles because we intended to summarize as much information as feasible and figured out that studies released as conference articles or abstracts might have not enough information we need. It is possible that the exclusion of abstracts and conference articles lead to publication bias. Data collection of the studies in this systematic review and meta-analysis was based on a retrospective- maternal recall process and may have had recall bias. The better way to control this bias would be to evaluate patterns of breastfeeding on cardiorespiratory fitness prospectively, with longitudinal follow-ups.
Conclusions
Breastfeeding shows beneficial effects on physical fitness, but further well-designed studies are suggested to clarify effects of breastfeeding on cardiorespiratory fitness.
Footnotes
Disclosure Statement
No competing financial interests exist.
Appendix
| Study ID | Study design | Selection (max 4 stars for cohort and 5 for cross sectional studies) | Comparability (max 2 stars) | Exposure (max 3 stars) | Quality |
|---|---|---|---|---|---|
| Lawlor et al. 15 | Cohort | **** | ** | *** | Good quality |
| Artero, et al. 13 | Cross-sectional | **** | ** | *** | Good quality |
| Labayen, et al. 10 | Cross-sectional | **** | ** | *** | Good quality |
| Vafa et al. 11 | Cohort | ** | ** | ** | Fair quality |
| Zaqout et al. 12 | Cross-sectional | **** | ** | *** | Good quality |