
Abstract
Abstract
Introduction:
Serratia marcescens is an opportunistic pathogen and common cause of infectious outbreaks in pediatric units, leading to both significant morbidity and mortality in immunocompromised hosts. Environmental and some clinical strains may produce a characteristic red pigment, prodigiosin. Colonization can hence turn breast milk and fecally-soiled diapers pink, which can lead otherwise unaffected patients to present to their physicians and also interrupt breastfeeding. No clear guidance exists regarding the outpatient management of breastfeeding mothers and infants colonized with S. marcescens.
Methods:
Our aim was to understand the significance of pigment–producing S. marcescens colonization of breast milk and stools in healthy infants in the community setting. We describe the case of a healthy 9-week-old infant presenting with pink soiled diapers secondary to S. marcescens colonization and systematically review previously reported cases of infants diagnosed with pink diapers or milk published in PubMed between 1958 and 2017.
Results:
Six publications describing seven additional mother-infant cases were selected for inclusion. In all, 8 mother-infant groups of colonization were reviewed, involving 10 infants (there were 2 sets of twins). Good clinical outcomes were reported in all cases regardless of whether antibiotic treatment was prescribed.
Conclusion:
Providers evaluating mother-infant dyads with S. marcescens colonization causing pink milk or pink infant soiled diapers should assess for manifestations of systemic infection. In the absence of evidence of clinical infection, expectant management is appropriate and continued breastfeeding can be supported.
Introduction
W
Outpatient cases of S. marcescens infection and colonization have also been reported, but reports of outpatient-acquired infections in immunocompetent pediatric patients are rare.15,16 To our knowledge, the first report of S. marcescens colonization was made by Waisman and Stone in 1958. The remarkable observation regarding this thriving infant who was fed a mixture of evaporated milk, water, and corn syrup was that fecally soiled diapers would turn red after 18–24 hours, which coined the term “red diaper syndrome.” S. marcescens grew from culture of her stool and was found to be identical to a strain aerosolized by a nearby research laboratory. 17 Since then, cases of colonization in healthy infants have been reported with a wide variety of diagnostic and treatment approaches described; some have included antimicrobial therapy and pauses from breastfeeding.11,14,17–20 The significance of isolation of S. marcescens in the community setting in asymptomatic infants and implications for breastfeeding remain unclear, particularly in mothers who express breast milk using a pump. Our aim was to better characterize the clinical outcomes of healthy infants colonized with prodigiosin–producing S. marcescens or who consume breast milk that is colonized with prodigiosin–producing S. marcescens. We present the case of a healthy infant who developed pink diapers secondary to S. marcescens and review previously reported cases of asymptomatic colonization.
Materials and Methods
A review of articles published in PubMed between 1958 and 2017 was conducted to identify previous reports of prodigiosin–producing S. marcescens colonization of breast milk or stool (Appendix Fig. A1). The search was conducted on February 22, 2017 with the following terms: disease (“pink milk”[All Fields] OR “pink diaper”[All Fields] OR “‘red diaper” [All Fields] OR “breastfeeding serratia” [All Fields] OR and “nursing serratia”) AND (“195801/01”[PDAT]: “2017/22/02”[PDAT]). Titles and abstracts were assessed for inclusion in the review. Articles not published in the English language were excluded. Articles without a clinical focus were excluded as were publications reporting patients older than 1 year of age. Finally, publications describing hospital-associated outbreaks or infections were excluded. Our objectives were to describe the clinical presentation of pigment–producing S. marcescens colonization in healthy infants or in the breast milk they were fed and compare clinical approaches of management. Of specific interest were morbidity of S. marcescens colonization and impact on breastfeeding cessation. For the purposes of this review, reports of pink expressed breast milk, pink milk in breast pump parts, equipment, and tubing, bottles or pink milk on nursing pads are referred to as “pink milk,” and cases describing soiled diapers that turned either red or pink with time are referred to as “pink diapers.”
Results
Our case
A healthy, term, breastfed female born through vaginal delivery presented at 11 weeks of age with a 2-week history of clothing that had been regurgitated on and soiled cloth diapers turning pink after being laundered (Fig. 1). Similarly, soiled disposable diapers and discarded nursing pads turned pink the following day. The infant seemed fussier than usual, especially in association with feeding, but was afebrile and otherwise well. Her birth history was uncomplicated other than brief readmission shortly after birth for management of hyperbilirubinemia. Her mother was on maternity leave from work as a surgical nurse and had intermittently used a breast pump to express milk for bottle feeding. The milk was normal in color during pumping. Following an Internet search, her mother presented to the pediatrician with concern for S. marcescens infection. At presentation, the infant was well appearing with normal vital signs, physical examination, and growth. After consulting with the infectious disease specialist, both mother and infant were treated with a 10-day course of trimethoprim–sulfamethoxazole (TMP-SMX) given the infant's fussiness. Cultures of the infant's stool and urine, as well as the mother's expressed breast milk, were sent, with no bacterial growth reported. Temporary discarding of expressed breast milk while completing antibiotic therapy and replacement of pump parts was recommended. During this period the red diapers resolved and infant's fussiness improved.
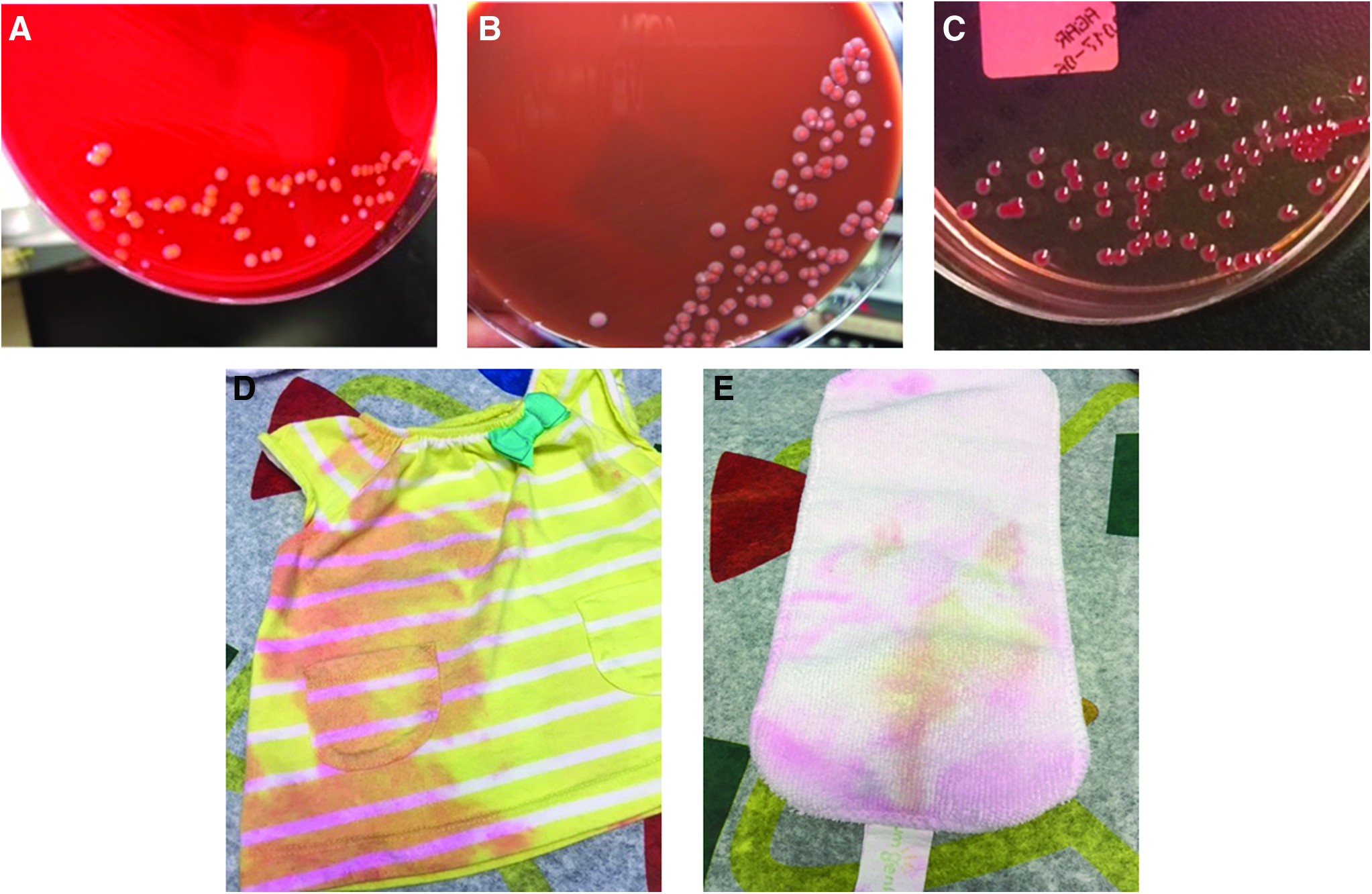
Prodigiosin–producing Serratia marcescens. Colonies on
Within 10 days of reintroduction of breast milk the infant's fussiness returned, seeming to increase as the volume of breast milk increased. The pink milk and stools also returned. In addition, pumping equipment had now turned pink. The infant's stool, urine, and blood were recultured, as were freshly expressed and older breast milk. A repeat 10-day course of TMP-SMX was prescribed for the infant, and a course of ciprofloxacin was recommended for her mother. This time, S. marcescens susceptible to TMP-SMX and ciprofloxacin was isolated in the infant's stool.
Search
One hundred thirty-eight publications were identified in our search. Of these, 105 publications were not clinical reports of Serratia and were excluded. Twenty-five publications focused on hospital-associated outbreaks, and two articles were published in non-English journals so were also excluded. A total of six publications describing seven additional mother-infant groups and nine infants (two sets of twins) were identified and included for review along with our case (Appendix Fig. A1).
Mother-infant group characteristics
There were 10 infants included in this description, including from the United States and Mexico. The baseline characteristics of the reviewed cases were similar (Table 1).11,14,17–20 With the exception of one case describing late preterm twins, all of the reported cases were born at term. 19 All infants were previously healthy and had only been treated for common newborn conditions such as unconjugated hyperbilirubinemia of infancy. The majority of the infants (90%, n = 9) were breastfed before the development of pink milk or diapers. Of the seven breastfeeding mother-infant groups, the majority of mothers (71.4%, n = 5) reported use of a breast pump, with only two mothers (28.5%) reporting never using a breast pump. Two of seven (28.5%) of breastfeeding mothers had recently been treated with antibiotics: one was treated with TMP-SMX and nitrofurantoin during pregnancy for urinary tract infections, and another was treated with dicloxacillin at 4 days postpartum for mastitis. One case reported an established environmental source of S. marcescens exposure in a nearby laboratory that was aerosolizing the organism. Our case was the only report that noted a parent working in healthcare.
Twin gestation.
Treated for mastitis 4 days postpartum.
Treated for urinary tract infection prepartum.
EBM, expressed breast milk; po, oral; TMP-SMX, trimethoprim–sulfamethoxazole.
Clinical presentation
Age at presentation to medical attention varied from 10 days to 3 months, with a median of 5–6 weeks. Signs of colonization included pink diapers, burp pads, breast pads/towels and breast pump supplies, and bottles. The most common presentation was some form of pink milk (87.5%, seven of eight reports). Three (38%) infants presented with pink diapers, including two breastfeeding infants and the one formula fed infant. While in the majority of cases pink milk or diapers were the only presenting signs, the mothers of 2 of the 10 infants (20%) reported additional symptoms such as fussiness or decreased feeding. All cases reported normal infant growth before development of pink milk and/or diapers.
Diagnostic cultures
In all seven cases presenting with pink milk, expressed breast milk was cultured. Breast milk cultures grew S. marcescens in six (86%) of seven cases. Of the three cases presenting with pink diapers, two sent stool cultures, which were both found to be positive either initially or on repeat culture.
Therapy
The approach to management regarding antibiotic use and breastfeeding recommendations was quite variable. All seven breastfeeding mothers were encouraged to continue breastfeeding, but in four cases (57%) they were advised to temporarily discard expressed breast milk until completion of antibiotics given the concern for symptomatology in the infant (Table 1). Choices of maternal antibiotics included ciprofloxacin, cephalosporin, and TMP-SMX. Three (38%) of eight infant groups were treated with antibiotics, choices including TMP-SMX and sulfasuxidine.
Repeat cultures
Repeat cultures were collected in two cases of pink milk after treatment and were found to be negative (Table 1). Evidence of continued colonization was noted in at least half (n = 2) of the treated infants, although repeat cultures were not consistently obtained.
Outcome
None of the infants developed clinical sepsis. Although follow-up time varied from a few weeks to several months, no adverse outcomes were reported. All infants were reported to be growing and developing normally at last follow-up, including those with evidence of continued colonization. While no direct measure of maternal stress was reported, at least one mother discontinued breastfeeding out of worry for the risk of infection (Table 1).
Discussion
Our report shows that good clinical outcomes were reported in all cases of community associated colonization. Human milk is an excellent culture medium for bacteria, and expressed breast milk is a recognized source of sepsis in susceptible infants. S. marcescens isolation from expressed breast milk has been implicated as the source of several healthcare-associated outbreaks in neonatal intensive care units, including fatal descriptions. 14 There is also at least one description of a healthy term infant developing S. marcescens bacteremia on day of life 17 after being fed expressed breast milk with heavy growth of Serratia, occurring shortly after hospitalization for another illness. 21 Of note, this strain was not prodigiosin producing. Considering this, infants presenting with pink milk or diapers should always be evaluated for clinical manifestations of systemic illness. Diagnostic evaluation is indicated if there is any suspicion of infection, and multiple cultures from different sources may be required to establish the diagnosis. Guidelines on the collection of breast milk for culture have been published. 22 As S. marcescens was not grown from breast milk in our case, it is possible that contamination could have occurred from an environmental source. In fact, S. marcescens was later cultured from their kitchen sink in attempt to identify potential sources of contamination, although genotyping was not carried out, so is difficult to interpret the significance of this. Microbiologic sampling of environmental surfaces however is expensive, complicated to conduct properly, and difficult to interpret, so should not be considered a routine part of evaluation.
While the actual number of bacteria excreted in milk is not well described, it seems unlikely that infants feeding directly from the breast would ingest enough bacteria to develop sepsis. Colony counts of bacteria were not quantified in our reported cases. Several other factors may contribute to either higher amounts of bacteria in breast milk and/or the subsequent development of sepsis. Improper handling or storage of expressed breast milk, for example, could facilitate the growth of bacteria within the milk. 23 One outbreak investigation conducted in a special care nursery suggests that contamination with >103 bacteria/mL is associated with feeding intolerance in premature babies and >106/mL can be associated with sepsis.21,24 Guidance exists on the proper handling and storage of breast milk. 25
A variety of management approaches are reported in our review, ranging from reassurance only to temporarily discarding of expressed breast milk and administration of antibiotic therapy to mother, infant, or both. Based on the reviewed cases, there is insufficient evidence to determine whether breast pump sterilization may prevent S. marcescens colonization or recurrence after treatment. S. marcescens has been isolated from breast pumping units 19 and can cause tubing to turn pink. Contamination of expressed breast milk by bacteria has been previously described and is thought to be a common.26–28 While one study demonstrated improvement in the degree of contamination after counseling regarding milk collection technique, the level of contamination considered acceptable and safe remains undefined. 26 Nevertheless recommending handling methods to reduce the level of contamination in breast milk is reasonable in dyads with S. marcescens colonization and could serve to alleviate parental concern and thereby support continued breastfeeding. Guidelines regarding maintaining breast pump cleanliness have been put forth by the U.S. Centers for Disease Control and should be offered as a reference to all mothers using this equipment. 29
While all patients presenting with signs and symptoms of infection should be evaluated appropriately, 21 based on our review, there does not appear to be clear evidence to support treatment of only colonization in otherwise well appearing healthy infants, and the significant risks of adverse reaction to antibiotic therapy and contribution to antimicrobial resistance must be considered. The infant in our case was treated for the symptom of fussiness. While she seemed to show symptomatic improvement with antibiotic therapy, the exact cause of the fussiness was never elucidated. She continued to have intermittent pink diapers, but never developed any further systemic symptoms or signs of infection and fussiness finally resolved after about 9 months of age. Other causes of fussiness, including gastroesophageal reflux and milk protein intolerance, were explored. The infant was also evaluated for Chronic Granulomatous Disease. Breastfeeding was discontinued after 6 months, after which pink diapers also resolved. At 1 year of life she continued to grow and develop normally. In the cardinal case described by Waisman and Stone, repeat stool cultures collected from the infant continued to intermittently grow S. marcescens during the first 2 years of life despite multiple courses of sulfasuxidine and the introduction of a probiotic rich diet.
It is interesting to note that at least three of the breastfeeding mothers (37%) had searched the Internet before seeking care. One mother discontinued breastfeeding after watching a disturbing Internet video despite provider education and encouragement to continue. 19 While we only found seven other cases in the medical literature, “pink milk” is more easily found as a discussion point on Internet forums for parents and social media, suggesting that this may even be a more common occurrence than reported in the medical literature. The AAP, Academy of Breastfeeding Medicine, and the U.S. Surgeon General's Call to Action emphasize the important role clinicians serve in supporting breastfeeding mothers 30 ; so providers who care for infants and breastfeeding mothers should be prepared to discuss the significance of S. marcescens colonization as the pink discoloration may cause parental distress.
There are several limitations to our descriptive report, including our retrospective analysis, lack of a control group, and the variable duration of follow-up reported. However, we were able to show that while prodigiosin–producing S. marcescens colonization causing pink milk or diapers is rarely reported, providers can support continued breastfeeding in the absence of signs of systemic infection as this is unlikely to pose significant risk to mother or infant, and antibiotic treatment does not appear to be indicated as good clinical outcomes were reported in all cases.
Conclusion
Providers evaluating mother-infant groups with S. marcescens colonization causing pink milk or red/pink infant diapers should assess for manifestations of systemic infection. In the absence of systemic illness expectant management is appropriate, breastfeeding can be supported and mothers educated on proper cleaning of breast pump parts.
Footnotes
Acknowledgments
The authors wish to acknowledge both the patient on which this case report is based and her mother. We would also like to acknowledge Dr. Melinda Poulter and Joanne Carroll for providing images of pigment- producing Serratia marcescens. This work was unfunded.
Disclosure Statement
The authors do not have any competing interests to disclose.