
Abstract
Abstract
Background:
Breast milk is considered the normative nutrition for human infants, and exclusive breastfeeding for the first 6 months of life is recommended by several national and global societies. Female physicians are a high-risk group for early unintended weaning. We aimed to assess and compare the most common barriers to successful breastfeeding perceived by female physicians in various stages of training and practice.
Materials and Methods:
Female faculty physicians and trainees (medical students, resident physicians, and fellows) affiliated with a large medical university in 2016 were surveyed via an anonymous web-based survey distributed through institutional e-mail lists. The three-item survey assessed role, breastfeeding experience, and perceived barriers to successful breastfeeding. Comparisons between groups were performed using Wilcoxon rank-sum tests or Fisher's exact tests.
Results:
The survey was distributed to 1,301 women with 223 responses included in analysis. The majority (57%) of respondents had never breastfed; of those, 87% reported plans to breastfeed in the future. Ninety-seven percent of women with breastfeeding experience reported at least one perceived barrier to successful breastfeeding. Trainees identified more barriers compared with faculty physicians (median count 5 versus 3, p = 0.014). No individual barrier reached statistical significance when comparing between faculty and trainees. The most frequently identified barriers to breastfeeding were lack of time and appropriate place to pump breast milk, unpredictable schedule, short maternity leave, and long working hours.
Conclusions:
Physicians and medical students who breastfeed face occupation-related barriers that could lead to early unintended weaning. Trainees and faculty report similar barriers. Institutional support may help improve some barriers to successful breastfeeding in female physicians.
Introduction
B
Physician advice has been shown to increase rates of breastfeeding initiation and continuation, and the strongest predictor of physicians' clinical breastfeeding advocacy is their personal or spousal breastfeeding behavior. 4 While physicians often have positive attitudes toward breastfeeding, their training generally lacks hands-on experience 5 and pediatric residents in the United States average 3 hours of breastfeeding education per year. 6 Infants cared for in institutions with residency curicula breastfeeding are more likely to breastfeed exclusively for 6 months. 7
Despite wide support for breastfeeding, physicians are a high-risk group for early unintended cessation of breastfeeding. 8 While physician mothers as a group have high rates of intention to breastfeed 9 and initiation of breastfeeding at birth,4,9 many do not breastfeed as long as intended or meet the recommendations of the American Academy of Pediatrics and World Health Organization for exclusive breastfeeding.4,9,10 A study of female physicians reported that while 64% intended to breastfeed for at least 12 months, 41% were feeding any breast milk by 6 months postpartum and only 29% were exclusively breastfeeding at 6 months. 9 A recent study of pediatric trainees showed that one-quarter of respondents did not meet their breastfeeding duration goal, and one-third did not meet their goal for exclusive breastfeeding; negative emotions were common among those not meeting their goals. 11
Many barriers to successful breastfeeding that have been described in the literature may affect female physicians. Barriers identified previously include inadequate milk supply, return to work, work schedule, and inability to breastfeed or express breast milk. 12 In a study of obstetrics residents, two-thirds discontinued breastfeeding earlier than planned, for reasons including low milk supply, work demands, and the perception that breastfeeding is too difficult during residency. 10 Trainees may also lack an appropriate room to pump or breastfeed. 11
This study aimed to identify barriers to successful breastfeeding in physicians in various stages of training and practice. We hypothesized that female physicians in all stages of training would report similar occupational-related barriers to breastfeeding.
Materials and Methods
An anonymous, web-based survey was distributed in 2016 via e-mail to female medical students, resident physicians, fellows, and faculty physicians affiliated with our medical university. E-mail addresses were obtained from the College of Medicine, the Graduate Medical Education office, and the Women's Faculty Development Caucus.
Inclusion criteria were female gender and current role as a medical student or physician employed by the medical university. Participants were not required to have children or experience with breastfeeding to respond to the survey. The survey addressed demographics, breastfeeding history, and perceived barriers to successful breastfeeding (Fig. 1). Roles were defined as trainee (medical student, resident physician, fellow) or faculty physician. Respondents who indicated nonphysician roles were excluded from statistical analysis.

Survey questions.
Data were analyzed using statistical software R v3.3.0 (R Foundation for Statistical Computing, Vienna, Austria). Comparisons between groups were performed using Wilcoxon rank-sum tests or Fisher's exact tests. p-Values <0.05 were considered to indicate statistical significance.
This study was approved by the University of Arkansas for Medical Sciences Institutional Review Board.
Results
The survey was widely distributed to a total of 1,301 women. There were 232 respondents to the survey. Nine nonphysician respondents were excluded, and a total of 223 responses were included in the analysis (Table 1). The most common roles represented were medical students (38%) and faculty (30%). The majority (57%) of respondents had never breastfed; 97 (43%) respondents reported personal breastfeeding experience. Of the 126 women who had not breastfed, 110 (87%) reported plans to breastfeed in the future.
Ninety-seven percent of women with breastfeeding experience reported facing at least one barrier to successful breastfeeding. As a group, trainees identified more barriers compared with faculty physicians (median count 5 versus 3, p = 0.014). Although no individual barrier reached statistical significance when comparing between faculty physicians and trainees, there was a trend of a larger proportion of trainees selecting each barrier compared with faculty physicians. Specifically, more trainees (83%) identified “no time” compared with faculty physicians (66%, p = 0.66). Overall, the most frequently identified barriers to breastfeeding were lack of time to breastfeed or pump milk (72%), unpredictable schedule (64%), lack of appropriate place to pump breast milk (50%), short maternity leave (47%), and long working hours (43%) (Fig. 2).
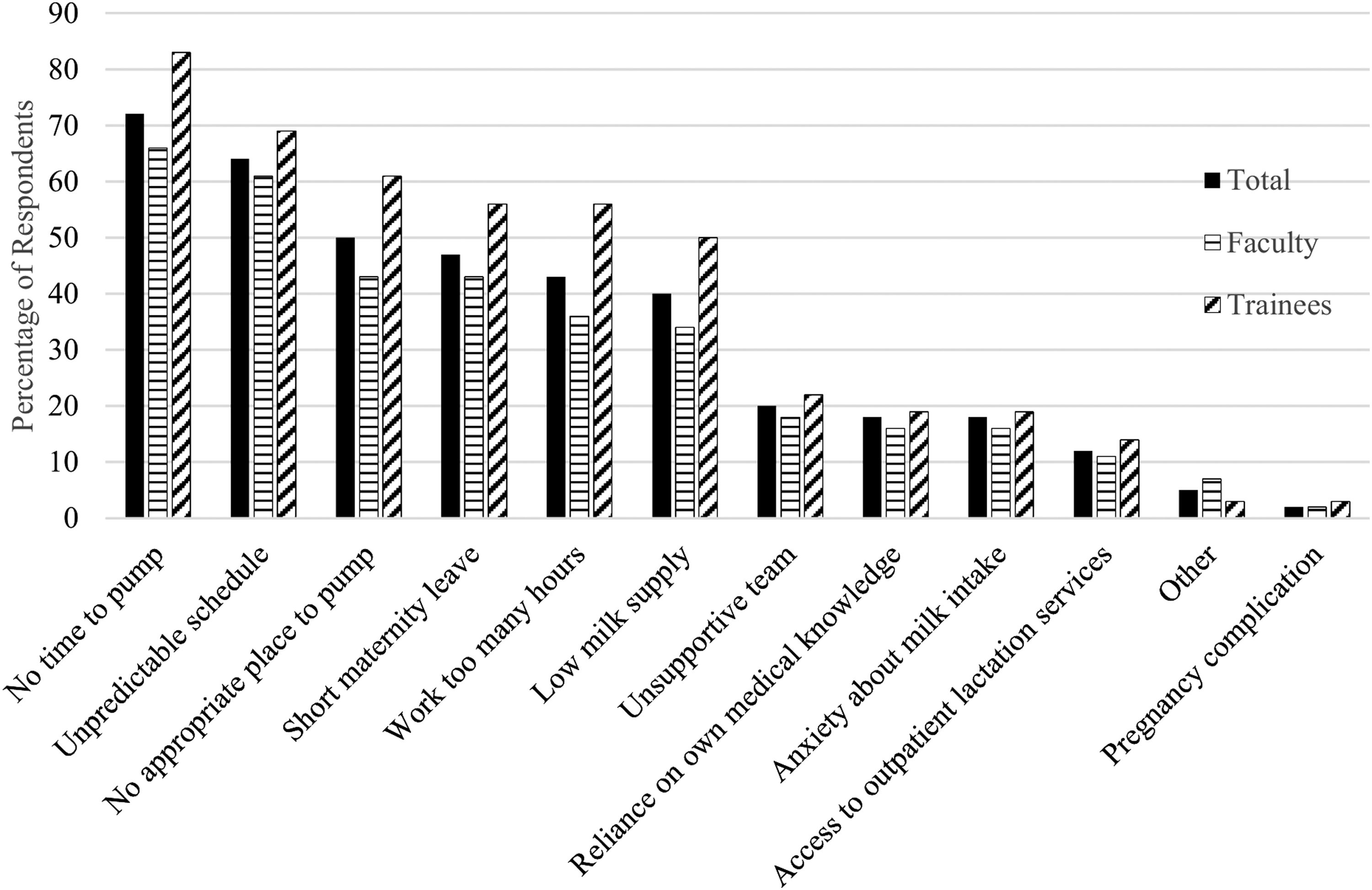
Perceived barriers to breastfeeding in female physicians and trainees currently or previously breastfeeding (N = 97).
Discussion
This survey of female physicians affiliated with a large medical university identified several barriers to successful breastfeeding faced by students and physicians in different stages of training and practice. It also showed a high percentage of female physicians who have never breastfed but plan to in the future.
Many of the barriers reported in our study may be occupation-related for physicians. Physicians may work long and unpredictable hours. In the United States during medical training, the Accreditation Council for Graduate Medical Education limits residents to 80 hours of clinical and educational work per week, averaged over 4 weeks. Shifts may last up to 28 consecutive hours. 13 After completion of training, physicians do not have restrictions on work hours. The mean annual hours worked by attending physicians across all specialties were 2,524, with wide variation among specialties. 14
A frequently cited barrier in our study was insufficient maternity leave. Previous research has demonstrated that shorter maternity leaves are associated with cessation of breastfeeding before 6 months. 15 In a study of a Canadian residency cohort, where the contract provided 17 consecutive weeks of pregnancy leave with the possibility of extending leave to 1 year, the average duration of maternity leave was 6 months. 16 The duration of maternity leave during medical residency in the United States is generally 4–8 weeks, although programs vary in whether this time is allocated as paid vacation or if the residency must be extended to accommodate the leave.17–20 Existence of formal parental leave policies in U.S. residency programs varies widely, with studies reporting ranges of less than one-third to greater than 90% of programs having policies.17,18,20,21
Insufficient maternity leave also affects practicing physicians. Only 29% of female attending physicians in a national survey reported that maternity leave was mentioned in their most recent contract. 22 A study of female urologists included 70% of respondents taking 8 weeks or less of maternity leave; women taking 9 weeks or longer were nearly four times as likely to report satisfaction with the leave. 23 A study in emergency medicine showed a range of no compensated time off to 12 weeks or more of fully paid leave. 24 More than half of female attending physicians reported losing more than $10,000 in income due to maternity leave, with no significant difference between procedural and nonprocedural fields. 22 Parental leave laws vary by state. In Arkansas, where this study was conducted, there are no state laws mandating paid parental leave time. 25
Half of the women with breastfeeding experience in our study reported lack of time and appropriate place to pump breast milk as a barrier to breastfeeding. This finding is reflected in existing literature. One-quarter of respondents in a previous survey of medical students and residents reported no private place to pump or breastfeed. 11 Forty percent of family practice residents in a national survey stopped breastfeeding earlier than planned due to residency demands. 19 A study of female urologists related inadequate breastfeeding duration to inability to break from work or the operating room to pump, long work hours interfering with nursing or pumping, and lack of place to pump breast milk. 23 In another study, physicians in surgical or procedural-based subspecialties universally reported that a significant challenge to successfully breastfeeding was the lack of lactation rooms close to the operating rooms. 9 This problem is not unique to hospitals; only 8% of U.S. airports 26 and 5.5% of U.S. convention centers, where medical conferences may be held, 27 provide appropriate pumping facilities for breastfeeding mothers.
The Affordable Care Act (ACA), passed in 2010, mandates that certain employers must provide reasonable break time and private space for the expression of breast milk. 28 However, this section of the ACA is an amendment of the Fair Labor Standards Act, which only covers employees subject to overtime pay, which are usually hourly employees, not salaried workers. 29 Thus, physicians who are salaried employees may only have legal breastfeeding protection through their state laws, which vary. 30 States are allowed to pass additional laws regarding breastfeeding. In Arkansas, the law states that employers must provide reasonable unpaid break time for the expression of breast milk and provide a private and sanitary room that is not a toilet stall for the expression of breast milk (A.C.A. § 11-5-116).
Our survey did not address intended breastfeeding goals or duration of breastfeeding. These questions were omitted in an effort to minimize the time required to answer the survey and increase response rate. Future research is warranted to correlate the barriers with breastfeeding duration and outcomes in female physicians, and intervention studies are needed to investigate whether initiatives aimed at alleviating or removing barriers are effective in supporting physicians' breastfeeding goals. There is also likely a participation bias, in that women with no interest in breastfeeding may be less likely to respond to a survey about breastfeeding. This is a single-center study, which may limit generalizability of our findings. We did not collect information on specialty among the residents, fellows, and faculty respondents, which also limits generalizability. Differences among specialties such as shifts and hours worked, location (inpatient, outpatient, operating rooms), and amount of procedures done may determine which barriers more heavily affect those physicians; future research could help further direct specific interventions to alleviate barriers to breastfeeding. Because the respondents in our study were affiliated with an academic institution, our results may not be generalizable to other populations of physicians, such as those in private practice. Laws regarding parental leave and breastfeeding protection vary by state.30,31
Our study is unique in that it included women in various stages of medical training and practice. We had a fairly high number of responses, although our sample size may be too small to identify some statistical differences. Our survey also allowed respondents to identify multiple barriers they perceived facing during breastfeeding.
We limited our subjects to female medical students and physicians to maintain a homogenous population; however, many women employed in a variety of fields likely face similar barriers to breastfeeding. For example, a study of female lawyers also showed shorter duration of breastfeeding than intended and recommended, correlating with level of support at work and sufficient time and place to pump breast milk. 32 More research into the needs of all employed breastfeeding women may help bolster support from employers. Increased workplace support for breastfeeding is associated with increased job satisfaction. 33 Evidence shows that successful breastfeeding reaps mental and physical health benefits for mothers and children as well as economic benefits. 2 Our results underscore the need for institutional backing of breastfeeding support, including expanded breastfeeding education in residency, stronger maternity leave policies, and improvement in support for pumping such as blocked time and access to appropriate facilities.
Footnotes
Acknowledgment
The authors report no external funding source for this study.
Disclosure Statement
No competing financial interests exist.