
Abstract
Abstract
Background:
Nonnutritive sucking (NNS) has been identified as having many benefits for preterm infants. NNS may improve the efficacy of oral feeding, reduce the length of time spent in orogastric (OG) tube feeding, and shorten the length of hospital stays for preterm infants.
Aim:
This study aimed to assess the effect of pacifiers on preterm infants in the transition from gavage to oral feeding, their time to discharge, weight gain, and time for transition to full breastfeeding.
Methods:
A prospective, randomized controlled trial was conducted in our center. Ninety infants were randomized into two groups: a pacifier group (PG) (n = 45) and a control group (n = 45). Eligibility criteria included body weight less than or equal to 1,500 g, gestational age (GA) younger than 32 weeks, tolerating at least 100 kcals/kg/day by OG feeding, growth parameters appropriate for GA, and a stable clinical condition.
Results:
Mean GAs were 29.2 ± 1.86 versus 28.4 ± 1.84 weeks (p = 0.46), and birth weights were 1,188.2 ± 272 versus 1,112.8 ± 267 g (p = 0.72) in the PG and CG groups, respectively. The time for transition to full oral feeding (38 ± 19.2 days), time to transition to full breastfeeding (38.1 ± 20 days), and time to discharge (48.4 ± 19.2 days) in the PG were significantly shorter compared with the control group (49.8 ± 23.6, 49.1 ± 22, 65.3 ± 30.6 days, respectively) (p < 0.05). For preterm infants with gastrointestinal motility disturbance, similar symptoms (regurgitation, vomiting, abdominal distension) (n = 6, 22%) in the PG were significantly lower than the control group (n = 21, 77.8%) (p < 0.05).
Conclusion:
In this study, we determined that the method of giving pacifiers to preterm infants during gavage feeding reduced the infants' transition period to oral feeding and the duration of hospital stay. In addition, the pacifiers could be used during gavage feeding and in the transition from gavage to oral/breastfeeding in preterm infants to encourage the development of sucking ability.
Introduction
T
Coordinated feeding in infants requires the sensorial and motor integration of sucking, swallowing and breathing, where several muscle groups participate in an observable rhythmic process. 5 Although sucking movements exist from the 28th gestational week, feeding must be started thorough gavage methods (nasogastric/orogastric) for preterm infants. Improvement of sucking in preterm infants may be achieved gradually and spontaneously at 34 weeks of gestational corrected age.2,5 Some studies showed that by using various external stimuli (pacifier, lullaby, music, breast milk smell, kangaroo care, etc.), preterm infants can proceed to oral feeding earlier than the 34th gestational week. 2 Via sensory-motor stimulation, pacifier use might also help in achieving oral feeding and reducing hospital stay. At the same time, NNS provided by a pacifier might elicit different physiological, pharyngeal, and esophageal motility events, potentially affecting gastroesophageal reflux. 6 In addition, advantages of pacifier use for preterm infants have been defined, which include neurodevelopmental organization, supporting neurobehavioral maturation, and optimizing ventilation in preterm infants who require nasal noninvasive ventilatory support, as well as reducing pain. 7 The World Health Organization (WHO) proscribes the use of a pacifier in the list of 10 steps toward successful breastfeeding. 8 Many studies have shown that pacifier usage during gavage feeding may encourage the development of the sucking behavior of preterm infants. 9 Therefore, the risks and benefits of pacifiers need to be clarified.
The aim of this research was to assess the effect of giving pacifiers to preterm infants on the transition period to oral feeding, time at transition to full breastfeeding, time to discharge, body weight at discharge, weight gain rate, and gastrointestinal intolerance symptoms.
Methods
This prospective, single-center, randomized, controlled study was conducted in the Neonatal Intensive Care Unit (NICU) of the University of Health Sciences Zekai Tahir Burak Maternity Teaching Hospital between July 2016 and November 2017. The trial was approved by the local Ethics Committee. Written informed parental consent was obtained for each patient. Inclusion criteria for enrollment in this study were that the preterm infants had a gestational age (GA) between 26 and 32 weeks, had a stable clinical condition and full enteral feeding with an orogastric (OG) tube, and had a birthweight of 1,500 g or less. A simple randomization method was used to allocate infants to groups. The research was conducted with 90 preterm infants. The infants were divided into two groups as follows: (1) control group, including 45 infants not using pacifiers and (2) pacifier group (PG), including 45 infants using pacifiers. In the present study, the PG and the control group were compared in terms of time to transition to full breastfeeding and full oral feeding, time to discharge, and daily weight gain of the preterm infants. Preterm infants with congenital anomalies, perinatal asphyxia, prolonged respiratory distress, intraventricular hemorrhage of greater than grade 2 according to the Papille classification, 10 hyperbilirubinemia requiring exchange transfusion, or intestinal anomalies or necrotizing enterocolitis with a Bell stage ≥2 11 were excluded. In addition, preterm infants receiving invasive or noninvasive mechanical ventilator support were excluded from the study. For preterm infants, an intravenous dextrose solution was begun after delivery. This was followed, usually within 24–36 hours, with total parenteral nutrition and lipids. Trophic or low-volume gavage feedings were started within the first days of life.
Gavage feeding is a procedure in which a tube passed through the nose or mouth into the stomach is used to feed a newborn with weak sucking, uncoordinated sucking, and swallowing. Infants were gavage fed until they were developmentally and physiologically ready to begin the process of learning to suck, swallow, and breathe in a coordinated manner. Preterm infants who did not need total parenteral nutrition were fed via an OG tube and cared for in the neonatal intensive care. Feeding was carried out every 2 or 3 hours via OG tube according to the weight of the infants. The required amount of breast milk that should be given to the preterm infant for energy need was calculated by a neonatologist. A pacifier was used every day during four feedings and the postprandial period. The attending nurse regularly checked that the pacifier was in place and periodically slightly alerted it to stimulate the sucking reflex.
In the PG, before and after the feeding time for a total of four times a day, preterm infants were allowed to use pacifiers for 15 minutes. The mothers use an electric pump (Ameda, Lincolnshire, IL) to empty her breast just before the infant's gavage feeding time. Preterm infants were fed with a syringe during the transition to the mother's breast. When the oral feeding process was completed, pacifier implementation was also terminated. In the control group, no procedure other than standard nursing care was applied to the preterm infants in the control group. Since our hospital is a Baby-Friendly Hospital, there was no pacifier and no bottle use in routine practice in the NICU. The study flow diagram for the enrollment of the preterm infants is shown in Figure 1.
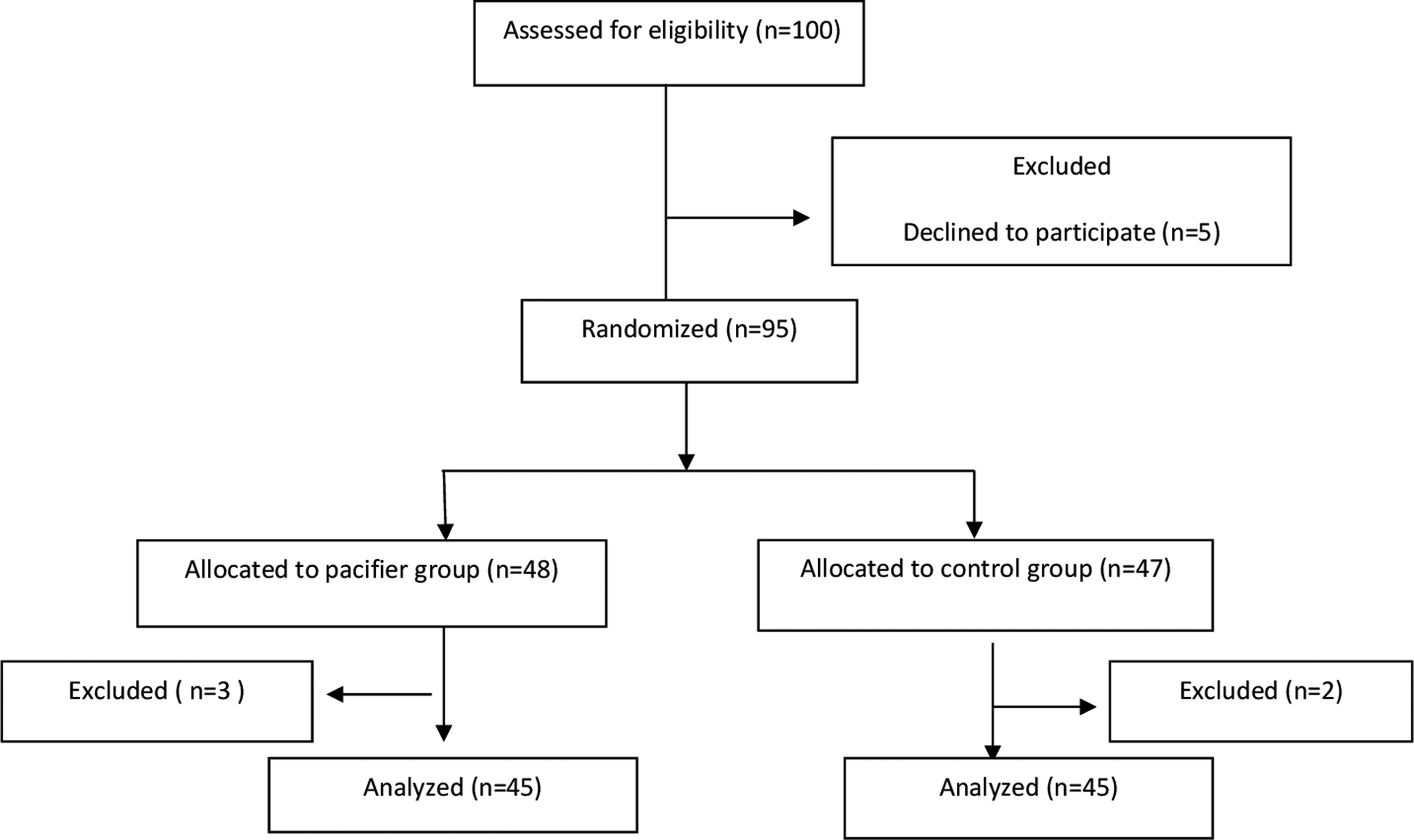
The flowchart of the clinical trial.
The pacifier used in the present study was “From Read McCarty, Inventor of GumDrop®& Soothie®, Hawaii Medical GumDrop Pacifier, USA.” Time to full enteral feeding, OG tube feeding time, time at transition to full breastfeeding, time to discharge, weight at discharge, daily body weight, and gastrointestinal intolerance symptoms of the preterm infants were recorded during the study.
Statistical analysis
Data were analyzed using IBM SPSS Statistics 21.0 (SPSS, Inc., Chicago, IL) statistical package program, and statistical significance was set at p < 0.05. A descriptive analysis of the demographic and clinical characteristics of the patients was conducted. Student's t-test for parametric data or Mann–Whitney U test for nonparametric data was used for comparison of variables between the two groups. Chi-square test was used to compare ratios between the two groups.
Results
Participant flow and follow-up: we invited 100 women to participate, 5 refused (Fig. 1). During the study, three cases were excluded from the PG and two cases were excluded from the control group due to unstable clinical state. Thus, 90 infants were enrolled and available for the primary analyses (PG, n = 45; control group, n = 45). Characteristics of the participants, including both maternal and neonatal characteristics, were balanced between the groups (Table 1). The time to start pacifier use for preterm infants in the PG was a mean of 29.64 days. Mean GAs were 29.2 ± 1.86 versus 28.4 ± 1.84 weeks (p = 0.46), and birth weights were 1,188.2 ± 272 versus 1,112.8 ± 267 g (p = 0.72) in the PG and CG groups, respectively. The comparison of control and PGs is presented in Table 2. There were no significant differences in late neonatal sepsis, time to reach birth weight, body weight at discharge, and body weight gain (g/day). However, there were significant differences between the groups in gavage feeding duration, time for transition to full breastfeeding and time to discharge (p < 0.05). The time for transition to full oral feeding (38 ± 19.2 days), time to transition to full breastfeeding (38.1 ± 20 days), and time to discharge (48.4 ± 19.2 days) in the PG were significantly shorter than the control group (49.8 ± 23.6, 49.1 ± 22, 65.3 ± 30.6 days, respectively) (p < 0.05). In addition, for preterm infants with gastrointestinal motility disturbance, similar symptoms (regurgitation, vomiting, abdominal distension) (n = 6, 22%) in the PG were significantly lower than the control group (n = 21, 77.8%) (p < 0.05).
Mean ± SD.
Mean ± SD.
LNS, late neonatal sepsis.
Discussion
Studies on pacifier use have reported that its use in preterm infants helps make the baby awake and active before feeding. It also helps to increase the secretion of gastrointestinal hormones by accelerating the development of the sucking reflexes of the infant. In this study, pacifier use significantly decreased the time of transition from gavage feeding to oral feeding and duration of hospital stay. A meta-analysis by Pinelli and Symington showed that positive outcomes were demonstrated for NNS with respect to reduced length of hospital stay. 12 Orocutaneous therapy using pacifiers has been associated with nonnutritive suck development and enhanced feeding performance, 12 in addition to decreased length of hospitalization.
Pacifiers are not recommended for term infants because of the relationship between pacifier use and decreased incidence of exclusive breastfeeding (EBF). NNS, however, has been found to strengthen the preterm infant's oral-facial musculature, lead to more effective bottle feeding, and significantly decrease the length of hospitalization. Because of these positive effects, preterm infants are traditionally provided pacifiers to improve their oral motor skills at the earliest possible GA.13,14 Some studies also demonstrated a positive effect of NNS on the exhibited less defensive behaviors during tube feeding.9,14 Some researchers found that pacifier use has been identified as a factor associated with shorter duration of EBF in observational studies. 15 However, preterm infants with immature neurological development and uncoordinated sucking-swallowing-breathing pattern cannot be fed by mouth successfully and safely. 15 Therefore, it is important that improving sucking skills and pacifier use recommendations need to be based on a benefit-risk approach focus for preterm infants. A Cochrane review found that nonnutritive sucking is associated with shorter hospital stays, earlier transition to bottle feeding from enteral feeding, and improved bottle feeding. Although the review did not show that pacifiers have a significant impact on weight gain, behavior, energy intake, heart rate, oxygen saturation, or age at full oral feeding, none of the studies reported harmful effects from pacifier use. 16
Furthermore, oral feeding is a complex multisystem process involving the integration of lips, jaw, cheeks, tongue, palate, pharynx, and larynx. 15 Pacifiers are used as a means for providing sensitivity to mechanical stimuli such as pressure to the orofacial and lingual sucking apparatus for activating the sensory-motor components of cranial nerves V, VII, IX, X, and XII that are involved in safe feeding. 12 The pharyngoesophageal motility of preterm infants does mature with increasing postnatal age. In this study, gastrointestinal motility disturbance with similar symptoms (regurgitation, vomiting, abdominal distension) in the PG was significantly lower than the control group (22%, 77.8%, respectively) (p < 0.05). The Cochrane review by Pinelli and Symington also included studies of the effect of NNS in preterm infants on a number of outcomes related to gastrointestinal function and feeding. The results of that review revealed no significant effect of NNS on weight gain, energy intake, intestinal transit time, postconceptional age at full oral feeding, and energy expenditure. 16 Another systematic review by Premji and Paes using many of the same studies came to similar conclusions, that is, the effects of gastric emptying and weight gain on preterm infants were inconclusive. 17 In our study, we analyzed the effects of pacifier use on the time at transition from gavage feeding to oral feeding, time at transition to full breastfeeding, time to discharge and duration of hospital stay of gavage-fed premature infants. The time for transition to full oral feeding (38 ± 19.2 days), time to transition to full breastfeeding (38.1 ± 20 days), and time to discharge (48.4 ± 19.2 days) in the PG were significantly shorter compared with the control group (49.8 ± 23.6, 49.1 ± 22, 65.3 ± 30.6 days, respectively) (p < 0.05). However, there were no significant differences in body weight at discharge or body weight gain in our study (p > 0.05). One study of 71 infants ranging from 26.7 to 35.9 weeks GA found that extremely preterm infants allowed NNS at the breast were able to latch on and demonstrate nutritive sucking as early as 30 weeks GA. 17
Medical and public health organizations recommend that mothers exclusively breastfeed for at least 6 months. 18 NNS at the breast has been associated with longer breast-feeding duration and allows the critically ill infant to have a smooth transition at breast feeds. 19 Nonnutritive sucking at the breast should be initiated once an infant has been extubated. 20 However, the lack of a mother hotel in our hospital made it difficult for mothers to access it at certain intervals during the day. Because of this reason the mothers are unable to do NNS with the infants at the breast. This is a limitation of the study.
Most of the 18,000 babies born each year or admitted to the Zekai Tahir Burak Maternity Teaching Hospital are premature, as the hospital handles high-risk births. The high rate of hospitalization in our neonatal intensive care units and the low socioeconomic level of the mothers led us researchers to do such studies. Although hospitalization costs of preterm infants are covered by the state in our country, the difficulty of educating a mother, the prolongation of the hospitalization period of preterm infants, and the complications related to it should also be considered. In addition to the WHO recommendation, which is generally accepted around the world, it is necessary for units to act according to their specific problems and the characteristics of their populations. 19
Footnotes
Disclosure Statement
No competing financial interests exist.