
Abstract
Abstract
Background:
Mother-infant skin-to-skin contact (SSC) immediately after birth helps transition infants to the post-uterine environment and increases the likelihood of breastfeeding initiation and duration. This study examines trends in U.S. maternity practices related to SSC, and variations by facility demographics.
Methods:
Data were from the Maternity Practices in Infant Nutrition and Care (mPINC) surveys (2007–2015), a biennial assessment of all U.S. maternity facilities. Facilities reported how often patients were encouraged to practice mother-infant SSC for ≥30 minutes within 1 hour of uncomplicated vaginal birth and 2 hours of uncomplicated cesarean birth, and how often routine infant procedures are performed while in SSC. We calculated the percentage of maternity facilities reporting these indicators for ≥90% of patients across the United States for each survey year. Estimates by facility characteristics (size, type, and state) were calculated for 2015 only.
Results:
The percentage of facilities reporting “Most (≥90%)” women, which were encouraged to practice early SSC, increased from 2007 to 2015 following both vaginal (40.4% to 83.0%) and cesarean (29.3% to 69.9%) births. The percentage of facilities reporting routine infant procedures were performed “Almost always (≥90%),” while mother and infant were SSC increased from 16.6% to 49.5% (2007 to 2015) for vaginal births and from 2.2% to 10.7% (2009 to 2015) for cesarean births. Variations in SSC practice by facility type, size, and state were noted.
Conclusions:
Significant progress has been made in increasing hospital encouragement of early SSC for both vaginal and cesarean births. Continued efforts to support evidence-based maternity practices are needed.
Introduction
B
SSC is the practice of placing the naked infant in direct contact with the mother's bare chest immediately after birth, with a warmed blanket then typically placed on top of the infant's body. A 2016 Cochrane Systematic Review of early SSC for healthy newborn infants, defined as SSC initiated between 10 minutes and 24 hours after birth, found that SSC increases the likelihood of breastfeeding initiation and continuation, when compared to routine care that does not include SSC. 5 Placing a newborn in SSC immediately after birth can help them identify the nipple through smell and touch to facilitate early sucking. 6 It also stimulates the release of oxytocin and lowers maternal cortisol levels, which each plays a key role in facilitating maternal physiologic transitions that occur immediately after birth.7,8 In addition to increased breastfeeding rates, infants who experience SSC have been found to have higher cardiorespiratory system stability scores, higher blood glucose levels, and lower pain scores during procedures, compared to infants receiving routine hospital care.5,9
SSC is recommended by the WHO and the American Academy of Pediatrics (AAP) for all mothers and newborns immediately after birth, regardless of feeding method or mode of delivery, unless there are medically justifiable reasons to delay or refrain from its practice.10,11 They also specify that routine newborn procedures and assessments should be done while the infant is in SSC with the mother, and that painful procedures or those that require separation should be delayed until after the first hour or completion of the first breastfeed.
Birth by cesarean section is associated with decreased likelihood of breastfeeding, increased time until the first breastfeed, and delay in the onset of lactation.12,13 Some previous studies have suggested that SSC immediately after cesarean birth in healthy newborns increases the likelihood of successful breastfeeding and breastfeeding at one and 4 months, but the number of women included in these studies was too small to consider the findings conclusive. 5 Some of the potential challenges of SSC implementation unique to cesarean births include concern for newborn hypothermia due to the colder operating room temperature, maternal pain and positioning, staff availability to adequately monitor mother and infant, and staff willingness to facilitate the SSC. However, most of these barriers can be overcome with routine safety and monitoring procedures put in place, along with staff education and training.12,14,15
The prevalence of maternity facilities practicing SSC immediately after birth in the United States has not been well documented in the literature. The Centers for Disease Control and Prevention (CDC) has been collecting information on maternity care in U.S. birthing facilities since 2007 in the Maternity Practices in Infant Nutrition and Care (mPINC) survey, including SSC practice indicators. 16 Understanding how commonly SSC is being practiced, among which patients, and within what settings is key to informing interventions aimed at improving intrapartum care quality and outcomes for mothers and infants. The aim of this study is to examine trends in maternity care practice indicators related to SSC after birth in U.S. maternity facilities between 2007 and 2015, by mode of delivery. It will also explore differences in SSC practice by facility demographics in 2015.
Materials and Methods
Design
This study uses cross-sectional data from the mPINC survey, a biennial census of all hospitals and free-standing birth centers providing maternity care services in the United States and its territories. 16 mPINC has been conducted every 2 years from 2007 to 2015 to monitor facility-level practices and policies related to infant feeding and care in the United States. All U.S. facilities that routinely provide intrapartum care are eligible to participate in mPINC. The survey is completed by a key informant(s) from each facility deemed most knowledgeable about the facility's practices and policies related to infant feeding and nutrition during the intrapartum stay. Individuals are encouraged to get input from key staff as needed in responding to survey items. Respondents may submit the survey electronically or on paper.
This study examines trends in mPINC data related to maternal-infant SSC practices in maternity facilities from 2007 to 2015. The questions used for this analysis were asked specifically for all full-term, uncomplicated vaginal and cesarean births at the facility.
Measurement
Two indicators related to maternal-infant SSC were examined for both uncomplicated vaginal and cesarean section births; first, an indicator related to the frequency of patients encouraged to practice SSC after birth, and second, an indicator related to performing routine newborn procedures, while mother and infant were in SSC. The wording of these questions remained the same in all surveys between 2007 and 2015. However, facilities were not asked about performance of newborn procedures among cesarean section births in 2007, but were asked in subsequent survey years. 16
For the practice of SSC contact after birth, respondents were asked the following: “Approximately, how many mothers are encouraged to hold their healthy full-term infants skin-to-skin for at least 30 minutes within an hour of birth for uncomplicated vaginal births?” and “Approximately how many mothers are encouraged to hold their healthy full-term infants skin-to-skin for at least 30 minutes within 2 hours after delivery for uncomplicated cesarean births?” Response options included “Few (0–9%),” “Some (10–49%),” “Many (50–89%),” “Most (90%+),” or “Not Sure.”
For the practice of performing routine newborn procedures while in SSC, respondents were asked the following: “Are routine newborn procedures (e.g., newborn assessment, including Apgar, cord clamping, and identification, including foot printing) after uncomplicated vaginal births done while the mother is holding the healthy full-term infant skin-to-skin?” and “Are routine newborn procedures (e.g., newborn assessment, including Apgar, cord clamping, and identification, including foot printing) after uncomplicated cesarean births done while the mother is holding the healthy full-term infant skin-to-skin?” Response options included “Rarely (0–9%),” “Sometimes (10–49%),” “Often (50–89%),” “Almost always (90%+),” or “Not Sure.”
Data analysis
Descriptive statistics were calculated for the prevalence of encouragement of SSC after birth and performing routine newborn procedures while in SSC for each survey year from 2007 to 2015. These results were stratified by delivery mode, uncomplicated vaginal delivery or uncomplicated cesarean section. Results for vaginal deliveries included data from births at both hospitals and free-standing birth centers, while results for cesarean section deliveries were restricted to hospitals that reported the capability to perform cesarean sections. The “ideal” practices for each of these measures were then examined, defined as the percentage of birthing facilities reporting that “Most (90%+)” patients were encouraged to practice mother-infant SSC contact for at least 30 minutes after uncomplicated birth, and the percentage of birthing facilities reporting that newborn procedures are “Almost always (90%+)” done while mother is holding her infant in SSC. Trends in the prevalence of these ideal practices were examined from 2007 to 2015. Missing responses were excluded from the analyses.
Using the 2015 mPINC data, the prevalence of ideal SSC practices after birth was examined by facility demographics, including type (birth center, government hospital, nonprofit hospital, private hospital, or military hospital) and size (number of births per year). These data were also examined by U.S. state/territory, calculated as the percentage of birthing facilities within each state or territory reporting “Most (90%+)” patients were encouraged to practice mother-infant SSC for at least 30 minutes after uncomplicated vaginal and cesarean births. Results were shown in a U.S. map broken into categories with cut points chosen to highlight areas with the highest and lowest prevalence of ideal SSC practice for vaginal and cesarean births. Facility subgroups or states/territories with less than five facilities reporting data were suppressed to protect confidentiality.
Results
Response rates for the 2007 to 2015 mPINC surveys ranged from 82% to 83%, representing 2582 to 2742 maternity facilities in each survey. Across these data years, most participating facilities were nonprofit hospitals (61.4–63.1%), followed by government-run hospitals (18.3–19.8%), private hospitals (11.6–13.0%), birth centers (4.4–6.3%), and military hospitals (0.7–1.0%). Across all data years, ∼23% of facilities had between 1–249 births per year, about 38% had 250–999 births per year, about 37% had 1000–4999 births per year, and about 2% had 5000 or more births per year.
Across survey years, response rates to SSC questions ranged from 96% to 99% for those related to vaginal births, and from 89% to 94% for those related to cesarean births, among hospitals performing cesarean sections. The percentage of facilities reporting “Most (≥90%)” women were encouraged to hold their healthy, full-term infants in SSC for at least 30 minutes within 1 hour after uncomplicated vaginal birth increased from 40.4% to 83.0% between 2007 and 2015 (Fig. 1). Among hospitals performing cesarean sections, the percentage reporting “Most (≥90%)” women were encouraged to hold their healthy, full-term infants SSC for at least 30 minutes within 2 hours after uncomplicated cesarean birth also increased over each survey year, from 29.3% in 2007 to 69.9% in 2015.
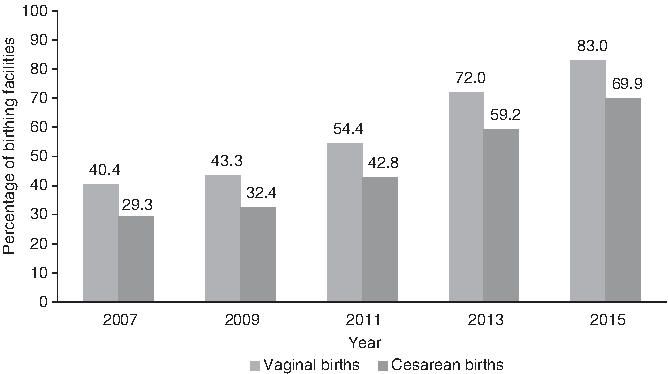
Percentage of birthing facilities reporting that most (≥90%) patients were encouraged to practice early* SSC for at least 30 minutes after uncomplicated birth, by mode of delivery, 2007–2015. *Within 1 hour for vaginal births; within 2 hours for cesarean births. SSC, skin-to-skin contact.
The percentage of facilities reporting that routine newborn procedures were “Almost always (≥90%)” performed while mother was holding the infant in SSC increased from 16.6% to 49.5% for uncomplicated vaginal births between 2007 and 2015 (Fig. 2). The percentage reporting this practice following uncomplicated cesarean births increased from 2.2% to 10.7% of facilities from 2009 to 2015; these data were not collected for cesarean section births in 2007.
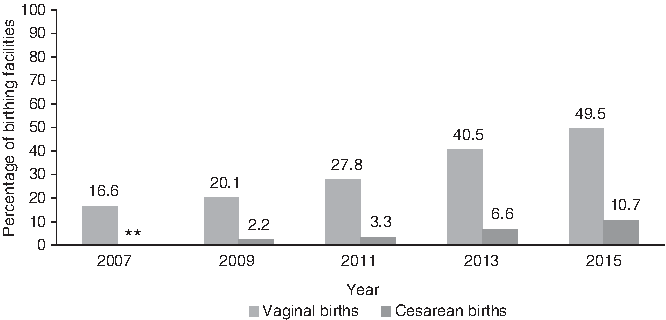
Percentage of birthing facilities reporting that newborn procedures are “almost always” (≥90%) done while mother is holding infant skin-to-skin, by mode of delivery, 2007–2015. **Data not collected for cesarean births in 2007.
In 2015, birth centers most frequently reported ideal SSC practice after uncomplicated vaginal births (98.2%), followed by military hospitals (90.0%), nonprofit hospitals (84.7%), government hospitals (76.2%), and private hospitals (75.7%) (Table 1). There was less variation in SSC practice by facility size in 2015, ranging from 78.5% of facilities performing 500–999 births per year reporting that “Most (≥90%)” patients were encouraged to practice SSC after vaginal birth to 89.3% for facilities performing 2000–4999 births per year.
Number of facilities vary due to missing response.
Cesarean births not performed in birth centers.
SSC, skin-to-skin contact.
For uncomplicated cesarean births in 2015, nonprofit hospitals were the facility type most frequently reporting ideal SSC practice (73.8%), followed by government hospitals (65.7%), private hospitals (58.4%), and military hospitals (52.6%) (Table 1); birth centers were excluded because of not performing cesarean sections. Hospitals performing 2000 or more births per year more frequently reported that “Most (≥90%)” of their patients were encouraged to practice SSC after cesarean birth than hospitals performing less than 500 births per year.
In the 2015 mPINC data, many of the states with the highest percentages (≥95%) of facilities reporting ideal SSC practice after uncomplicated vaginal births were located in the northeastern part of the United States, including Vermont, Rhode Island, New Hampshire, Massachusetts, and Maine. In addition, New Mexico had a high proportion of facilities reporting ideal SSC practice (Fig. 3). States where <75% of facilities reported ideal SSC practice following vaginal birth included Arkansas, Mississippi, Kansas, North Dakota, Nebraska, Iowa, and South Dakota.

Percentage of maternity facilities reporting most (≥90%) patients were encouraged to practice mother-infant SSC for ≥30 minutes within 1 hour after uncomplicated vaginal birth, by state, mPINC 2015 (n = 2491)^. ^Refers to data suppressed for states or territories with <5 facilities in the numerator; this includes Washington, DC, American Samoa, Guam, the Northern Mariana Islands, and the United States Virgin Islands. mPINC, Maternity Practices in Infant Nutrition and Care.
For uncomplicated cesarean births in 2015, states with the highest percentages (≥80%) of facilities reporting that ideal SSC practice included Rhode Island, New Jersey, Wyoming, Alaska, Massachusetts, Delaware, Oregon, Illinois, Connecticut, and Minnesota (Fig. 4). States where <60% of facilities reported ideal practices related to SSC after cesarean section were mostly located in the southeastern part of the United States, including Mississippi, Arkansas, North Carolina, Alabama, South Carolina, Tennessee, Florida, and Georgia. Nevada and New Mexico also had a low proportion of facilities reporting ideal SSC practice.

Percentage of maternity facilities reporting most (≥90%) patients were encouraged to practice mother-infant SSC for ≥30 minutes within 2 hours after uncomplicated cesarean birth, by state, mPINC 2015 (n = 2298)^. ^Refers to suppressed for states or territories with <5 facilities in the numerator; this includes Washington, DC, American Samoa, Guam, the Northern Mariana Islands, Puerto Rico, and the Unites States Virgin Islands.
Discussion
The percentage of U.S. maternity facilities where SSC between mothers and infants is routinely encouraged immediately after birth has more than doubled from 2007 to 2015 for both vaginal and cesarean section births. Encouragement of SSC has become a common practice, occurring for most women at 83% of hospitals for uncomplicated vaginal births and 70% of hospitals for uncomplicated cesarean section births in 2015. The proportion of infants receiving routine newborn procedures while in SSC has also been steadily increasing and was practiced in about half of vaginal births in 2015, but remains relatively uncommon for cesarean births (11%). Some of these differences may be due to challenges specific to changing operating room practices to enable the performance of newborn procedures with the infant on mother's chest during surgery. Implementation of ideal SSC practice in 2015 varied by facility type and size, indicating that differences in hospital staffing, training, policies, and capacity for practice change may play a role in SSC implementation. SSC practice also varied across states, demonstrating that there may be geographic differences in provider practices and state-level policies and interventions aimed at improving maternity care practices.
Several initiatives aimed at improving maternity care practices that support breastfeeding might have played a role in increasing the encouragement of SSC practice in U.S. maternity facilities. The Baby-Friendly Hospital Initiative (BFHI) is a program launched by WHO and UNICEF in 1991 to recognize maternity facilities who successfully implement the Ten Steps to Successful Breastfeeding. 17 SSC is a fundamental component of Step 4: to help mothers initiate breastfeeding within 1 hour of birth. Between 2012 and 2015, 89 U.S. hospitals across 29 states participated in a CDC-funded quality improvement initiative called Best-Fed Beginnings, with the aim of increasing the number of Baby-Friendly designated hospitals. 18 Seventy-six of those hospitals have since received the Baby-Friendly designation, a substantial increase from the 100 total U.S.-designated hospitals in 2011. 19 Many states have also made significant investments in improving hospital support for breastfeeding, through a variety of strategies. For example, California passed a law that all hospitals need to implement the Ten Steps to Successful Breastfeeding or a similar package of evidence-based maternity care by 2025. 20 Kentucky developed a state strategic plan for improving breastfeeding, which specifically focused on increasing the number of maternity hospitals implementing SSC 21 ; and multiple states have developed recognition programs for hospitals implementing some or all of the Ten Steps to Successful Breastfeeding.22–24 These and other initiatives have likely played a role in increasing the total percentage of births occurring in BFHI-designated facilities in the United States from less than 3% in 2007 to more than 22% in 2017. 17 In addition, CDC provides every facility participating in mPINC with an individualized report on their results, which can help them identify areas for improvement in practices related to infant feeding and monitor progress over time.
As practicing SSC after birth has become more common, some concern has been raised over the potential for safety issues, including risk of sudden unexpected postnatal collapse, suffocation, and infant falls. 10 Some of these concerns relate to the ability to effectively monitor the infant when the mother may be tired or medicated after birth, staff may not be continuously observing the infant, or parents and staff may not be familiar with safe positioning of the infant on the mother's chest. A recent systematic review of the effects of early SSC for healthy newborns on breastfeeding and infant physiology did not find any evidence of harm in any of the 38 included studies, although assessment of SSC safety was not the main objective of the review. 5 There is currently no standardized surveillance system in place to monitor for these types of adverse events; so how commonly they occur during the practice of SSC immediately after birth is not known.
In response to concerns about the safety of SSC implementation, the AAP provided guidance in a 2016 Clinical Report on how to most safely implement the practice after birth. 10 This includes a step-by-step description of how to safely place the infant in SSC after birth as well as a checklist of components of safe positioning recommended be frequently assessed while in SSC, including the infant's position, breathing, activity, color, and tone. It also recommends that maternity facilities develop standardized procedures for SSC implementation, provide direct observation of the mother and infant while in the delivery room, document maternal and infant status while in SSC, and train all healthcare providers on these aspects of safe SSC implementation.
This study is the first to provide national-level estimates for the prevalence of SSC practice indicators after birth in the United States. These data are from a census of all facilities routinely providing intrapartum care, which offered a unique opportunity to explore nationally representative trends in maternity care practices. Another strength of this analysis is that the questions related to SSC were asked in the same way across the survey years, enabling examination of trends over time. The wording of the questions also allowed for assessment of differences in SSC practices by delivery type, which is important since different challenges exist in implementing changes in practice for vaginal and surgical births.
There are, however, some limitations to these data and analyses. First, the phrasing of the mPINC questions limited us to only assessing the prevalence of the encouragement of early SSC, rather than the prevalence of the actual practice. Furthermore, there may be some inaccuracy in the SSC prevalence estimates provided by staff responding to the survey. In addition, since patient-level data are not collected, we were unable to examine differences in SSC by patient demographics to explore potential variations among population subgroups. Last, some nonresponse bias was also possible, although unlikely to have a large impact on the results since response rates were quite high for each survey year overall and for the SSC questions specifically.
Despite these limitations, these data provide valuable national-level information on recent maternity indicators related to SSC, which have previously been identified as a key practice to facilitate the initiation and continuation of breastfeeding. More work is needed to understand the characteristics of both patients and maternity facilities practicing SSC more or less frequently to identify target populations for future interventions. Evaluation of the effectiveness and safety of interventions aimed at improving maternity care practices is also needed. As SSC continues to become a routine part of intrapartum care, monitoring and surveillance of safety indicators could also help enable continual improvement of implementation practices and ensure optimal patient outcomes.
Conclusion
The encouragement of SSC between mothers and newborns after birth has drastically increased for both uncomplicated vaginal and cesarean births in U.S. maternity facilities between 2007 and 2015. Hospitals are also more commonly performing routine infant procedures while the baby and mother remain in SSC. Differences in the prevalence of encouraging SSC were noted by facility type, size, and location, indicating groups with room to increase this practice as the standard of care for healthy newborns.
Footnotes
Authors' Contributions
Dr. Boundy contributed to the analytic study design, conducted the analysis, and drafted and revised the final article. Dr. Perrine, Ms. Barrera, Dr. Li, and Dr. Hamner contributed to the analytic study design and provided critical review of the article. All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Disclosure Statement
No competing financial interests exist.