
Abstract
Abstract
Background:
Latching is an important process of breastfeeding and should be taught and practiced by the postpartum mother.
Objective:
The objective is to compare latching outcomes between video-assisted and routine teaching methods among postpartum women.
Materials and Methods:
A randomized controlled trial was conducted. Postpartum women who had deliveries without complications were randomized into two groups: 14 cases in the video-assisted teaching group and 14 cases in a routine teaching group. In the first group, the mothers were taught breastfeeding benefits, latching methods, and breastfeeding positions and practiced breastfeeding in a controlled setting for a 30-minute period and watched a 6-minute video with consistent content. In the second group, the mothers were taught a normal 30-minute period and then practiced breastfeeding. In both groups, Latching on, Audible swallowing, the Type of nipples, Comfort, and Help (LATCH) scores were assessed at 24–32 and 48–56 hours after the breastfeeding teaching modals. Demographic data and LATCH scores were collected and analyzed.
Results:
There were no statistically significant differences in the mothers' ages, occupations, marital status, religion, education, income, infants' gestational age, body mass index, nipple length, route of delivery, and time to first latching between the video-assisted and routine breastfeeding teaching groups. First and second LATCH score assessments had shown no significant differences between both breastfeeding teaching groups.
Conclusion:
The video-assisted breastfeeding teaching did not improve latching outcomes when it was compared with routine teaching.
Introduction
L
Although the breastfeeding process is natural, postpartum mothers also need breastfeeding teaching and practice with a health professional during the inpatient period. 3 Therefore, all postpartum mothers are taught, practice, and are assessed for latching on a routine schedule in a breastfeeding support hospital. The most effective breastfeeding teaching patterns are with small group teaching (3–5 people per group) and a 0.5- or 1-hour duration course. The limited teaching time may have an effect on breastfeeding practices, in particular, latching. 7
Video media plays a role in helping to teach patients knowledge and techniques for practicing various procedures.8,9 Postpartum video-assisted teaching has been reported as a technique for improving breastfeeding knowledge.10,11 Also, the video may help mothers understand the procedure and process better as the video image is animated with a narrative voice. We were interested in comparing the latching outcomes of breastfeeding teaching between video-assisted and routine teaching.
Materials and Methods
Setting
This study was performed in the Nakhon Nayok province, a rural area in the central part of Thailand. The data were collected during the period from September to December 2017 at the HRH Princess Maha Chakri Sririndhorn Medical Center. At the postpartum ward, mothers are usually taught and practice breastfeeding for 30 minutes in the morning. After this, mothers are assessed by their Latching on, Audible swallowing, the Type of nipples, Comfort, and Help (LATCH) scores once initially and daily until discharge.
Design
This study is a single-blinded randomized controlled trial. The nurses who assessed LATCH scores did not know about teaching patterns for the mothers in both groups.
Inclusion criteria
Included in this study are postpartum women who had deliveries without complications (i.e., multiple pregnancies, preeclampsia, antepartum hemorrhage, and preterm labor). Their infants had birth weights of >2,500 g and were born without complications. The mothers had suffered no acute postpartum hemorrhages and had no contraindications to breastfeeding.
Exclusion criteria
Mothers whose infants were diagnosed with galactosemia were excluded from this study.
Sample size
We set a mean difference of one point between video-assisted and routine teaching groups as this mean possibly signifies a clinical difference. The sample size was based on 0.05 of α error, 0.95 of power, and an effect size of 2. The calculated sample size totaled eight in each group. The subjects were totaled with 75% data loss added. The total samples collected were 28.
Procedure and collection of material
Randomization was done using a computer-generated list with a block of two methods. Sequential numbers would be kept in sealed envelopes. Participants who met the inclusion criteria would be randomly allocated to either video-assisted or routine teaching groups. Breastfeeding teaching was given for postpartum mothers in the morning. In the first group, the mothers were taught breastfeeding benefits, latching methods, and breastfeeding positions for a 30-minute period and watched a 6-minute video containing the same content. They then practiced breastfeeding with an instructor. In the second group, the mothers were taught for a 30-minute period and then practiced breastfeeding. The first and second LATCH scores were assessed at 24–32 and 48–56 hours after the breastfeeding teaching, respectively. Demographic data and LATCH scores were collected and analyzed.
Breastfeeding teaching
Postpartum mothers were taught breastfeeding benefits and had a mannequin demonstration on latching and breastfeeding positioning with a hands-off technique taught by an experienced nurse in small groups (3–5 persons per group). 12 In the hands-off technique, the nurse helped to modify the infant's positioning without touching the mother and the infant but through answering of the mother's questions and/or showing appropriate positioning with mannequin demonstration. Thirty minutes of teaching time was divided into 5 minutes for breastfeeding benefits, 10 minutes for latching and breastfeeding positioning, and 15 minutes for practicing latching and positioning. The nurse who taught breastfeeding must have 2 years of experience in breastfeeding teaching and pass a researcher's assessment. Both groups were taught the same.
In the video-assisted group, mothers also see a 6-minute video on breastfeeding after routine breastfeeding teaching. Six minutes of video teaching time was divided into 1 minute for breastfeeding benefits and 5 minutes for latching and positioning. The video was played on a 10-inch tablet.
LATCH scores
The LATCH mnemonic scores are assessed by the mother holding the baby to breast. The criteria of “latching on” scores are 2 if the baby grasps the breast, tongue is positioned down and forward, lips are flanged, and the baby has rhythmic suckling; 1 is scored for baby's repeated attempts, the mother must hold her nipple in the baby's mouth or must stimulate the baby to suck; and 0 is given when the baby is too sleepy, reluctant, or no latch is obtained. The criteria of “audible swallowing” scores are 2 for spontaneous or frequent audible swallowing, 1 for a few audible swallowing with stimulation, and 0 for no swallowing. The criteria of “type of nipples” scores are 2 for everted after stimulation, 1 for flat, and 0 for inverted nipples. The criteria of “comfort” scores are set as 2 for soft, tender, and intact nipples (no damage); 1 for filling, small blisters, or bruises of the breasts or the mother complains of pinching or mild-to-moderate discomfort of her nipples or breasts. The criteria of “assistance requirement” scores are 2 for no assistance required from the staff or the mother can position or hold the baby; 1 for minimal assistance, teaching on one side, and the mother utilizes the other breast or the staff helps and the mother takes over the feeding independently; and 0 for full assistance or the staff holds the infant at the breast. 13
There were two nurses who assessed LATCH scores. The nurses must have 6 months of experience in LATCH score assessment and pass a researcher's orientation and assessment. LATCH score assessment nurses would not know the mothers' breastfeeding teaching groups.
Ethical considerations
This study was approved by the Ethics committee of Srinakharinwirot University, Faculty of Medicine, and registered with Thai Clinical Trials Registry (registration number TCTR20180228003).
Statistical analysis
Demographic data are reported in means and percentages. We used the t-test to compare the mean of maternal age, income, gestational age, body mass index, nipple length, and time to first latch between the video-assisted and routine teaching groups. The data of occupation, marital status, religion, education, and route of delivery were analyzed by chi-square and the Fisher's exact test. We used the intention to treat method for analysis. A p-value <0.05 was considered statistically significant. Statistical analysis was performed using SPSS software (version 23.0; SPSS Incorporated).
Results
The number of postpartum women enrolled in our research project totaled 28. A flow chart of the number of participants is shown in Figure 1. The mean age of the mothers was 25.6 ± 6.0 years. The mean gestational age at delivery was 38.9 ± 0.7 weeks. The mean body mass index was 21.3 ± 3.4 kg/m2. The percentage of cesarean sections was 64.3. The demographic data of the video-assisted teaching group was similar to those in the routine teaching group. There were no statistically significant differences in the mother's ages, occupation, marital status, religion, education, income, gestational ages, body mass index, nipple length, route of delivery, and time to first latch between the video-assisted and routine breastfeeding teaching groups. Demographic data are shown in Table 1.
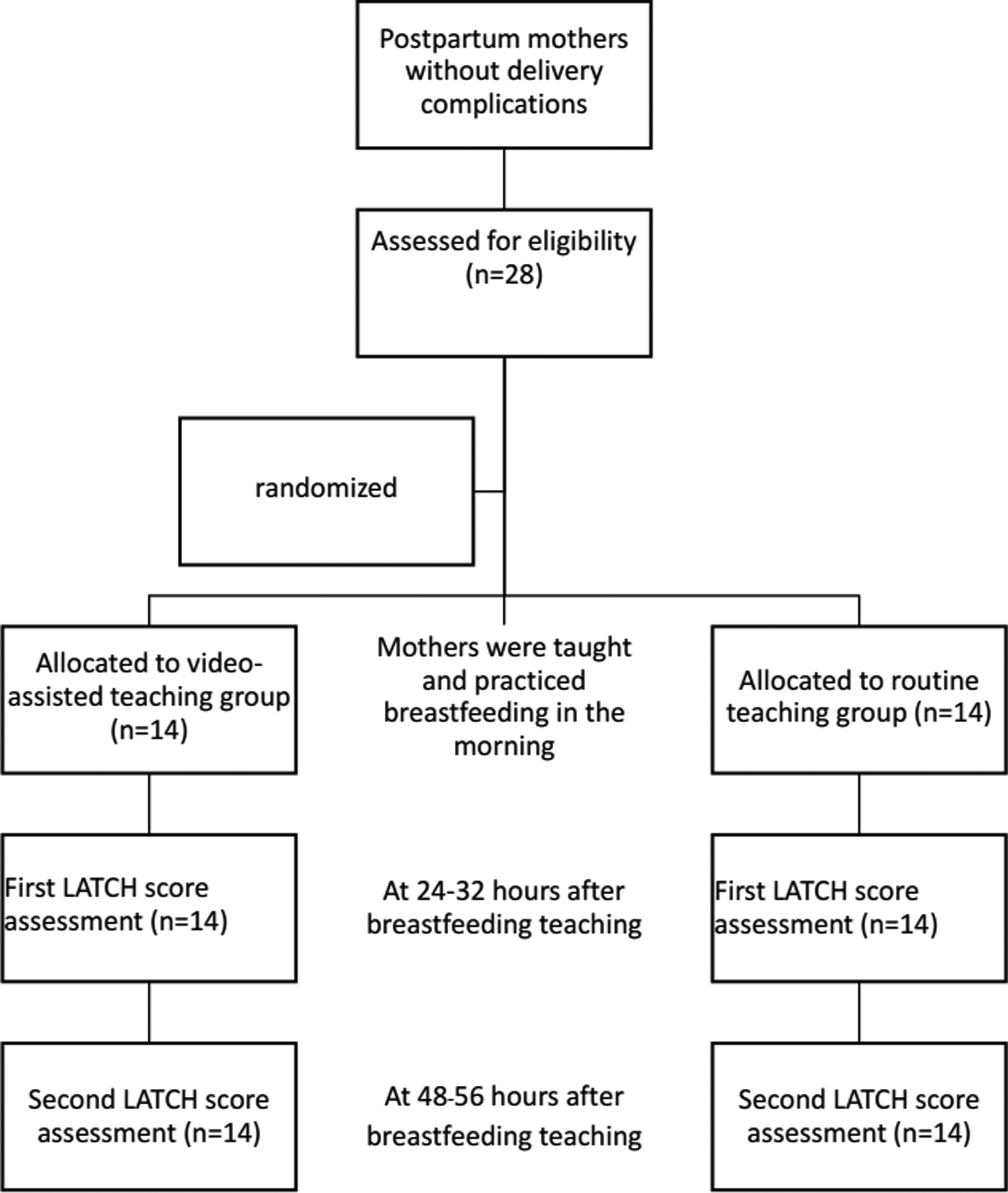
Flow diagram of participants through the study.
There were no statistically significant differences in the first and second LATCH score assessments between the video-assisted and routine teaching groups. The details of the LATCH scores at the first and second assessment are shown in Table 2.
Discussion
The LATCH score assessments between the video-assisted and routine teaching groups had no statistically significant differences. This result may be explained from the effectiveness of the hands-off breastfeeding technique and small group teachings. The hands-off technique could empower mothers to do latching themselves. This includes enabling mothers to position and attach their babies based on a physiological approach. 12 Mothers could ask the instructors any questions they may have as there is a close interaction between instructors and mothers during the teaching in small groups. Two-way communication between the mothers and instructors would help the mothers to understand and practice appropriate latching and positioning techniques without the need of video-assisted teaching. The benefits of video-assisted teaching are to improve postpartum mothers' knowledge about exclusive breastfeeding, and the management of breastfeeding problems has been reported from a previous study.10,11 But there was no difference of surgeon's skills between self-directed interactive video-based instruction and instructor-led teaching from the study of Lwin et al. 14 Therefore, the video-assisted teaching might not help mothers in breastfeeding practices.
In this study, the mothers had high cesarean section rates (64.3%). The tendencies for cesarean section rates are high in Thailand.15,16 It can delay the mothers' breastfeeding initiation.17,18 The time to first latch has shown a correlation for this. The generalization of the research results may be limited by the characteristics of the mothers.
The strength of this study is that it was a randomized controlled trial that provided experienced instructors with clear definitions of breastfeeding teaching and LATCH score assessment, and focused on the practice of breastfeeding rather than the knowledge of breastfeeding. Assessment of LATCH scores, which consists of latching and breastfeeding positioning parameters, was chosen. LATCH scores are commonly used for breastfeeding assessment in Thailand. Health professionals are familiar with these assessments. In addition, the benefits of LATCH scores are associated with the prediction of continuing breastfeeding at 6 weeks postpartum. 19 Breastfeeding knowledge was not assessed as it was not part of the main objective of this study. However, the sample size of this study was small. Increasing the sample size would help improve the generalizations of the research results.
Conclusion
Video-assisted breastfeeding teaching did not improve latching outcomes as compared with routine teaching. Routine teaching with small groups and use of the hands-off technique are important in the latching and positioning practices.
Footnotes
Acknowledgments
The authors thank the HRH Princess Maha Chakri Sririndhorn Medical Center and the Faculty of Medicine, Srinakharinwirot University, for supporting their research.
Disclosure Statement
No competing financial interests exist.