
Abstract
Abstract
Objectives:
Studies have shown that immediate postpartum initiation of long-acting reversible contraception (LARC) methods leads to increased utilization of LARC and prevention of unintended pregnancies. It is unclear if immediate postpartum levonorgestrel-releasing intrauterine device (LNG-IUD) insertion has an effect on breastfeeding success.
Study Design:
This study was a secondary analysis of a randomized trial that compared intrauterine device (IUD) use at 6 months postpartum among women who underwent intracesarean IUD placement with women who planned for interval IUD placement at 6 or more weeks postpartum. This parallel, 1:1, nonblinded randomized trial was conducted between March 2012 and June 2014 at the University of North Carolina Women's Hospital. We recruited pregnant women aged 18–45 years who were undergoing a cesarean delivery and desired an IUD for contraception postpartum.
Results:
We received breastfeeding information from 63 women who desired to use a LNG-IUD. A proportion analysis demonstrated that there was no difference in the proportion of women breastfeeding at any of the three time points, 6, 12, and 24 weeks, following placement. This remained true after adjusting for age, parity, and ethnicity.
Conclusion:
This study adds to the existing body of evidence that shows that most women are able to successfully breastfeed after immediate postpartum LNG-IUD placement. Women should be encouraged to breastfeed, and the desire to breastfeed should not preclude the initiation of a postplacental IUD. This study provides reassurance that immediate postpartum LNG-IUD placement does not adversely affect breastfeeding; however, more high-quality data are needed on the impact of hormonal IUDs on breastfeeding outcomes.
Introduction
I
The Centers for Disease Control and Prevention (CDC) consider the benefits of immediate postplacental LNG-IUD insertion to outweigh “theoretical or proven risks” for women who intend to breastfeed. 8 Although postplacental insertion of the LNG-IUD has been associated with decreased rates of exclusive breastfeeding, a recent noninferiority trial demonstrated that women who received a hormonal IUD at the time of delivery were just as likely to be breastfeeding at 8 weeks postpartum as those women who received a hormonal IUD at 4–12 weeks postpartum. 9 More evidence is needed to guide postpartum LNG-IUD recommendations, specifically for women who intend to breastfeed.
The purpose of this secondary analysis was to compare breastfeeding rates among women who underwent hormonal IUD placement at the time of cesarean delivery with women who planned for interval IUD placement at 6 or more weeks after delivery.
Materials and Methods
This study was a secondary analysis of a randomized clinical trial that compared IUD use at 6 months postpartum among women who underwent intracesarean IUD placement with women who planned for interval IUD placement at 6 or more weeks postpartum. The study was approved by the University of North Carolina at Chapel Hill Institutional Review Board and was registered at ClinicalTrials.gov (NCT01539759). The study protocol, demographics, and outcomes have been fully described elsewhere. 3 Briefly, this was a parallel, 1:1, non-blinded randomized trial conducted between March 2012 and June 2014 at the University of North Carolina Women's Hospital. We recruited pregnant women aged 18–45 years who were undergoing a cesarean delivery and desired an IUD for contraception postpartum. Additional inclusion criteria were as follows: (1) English or Spanish speaking, (2) intention to comply with the follow-up, and (3) delivery of a live-born infant greater than 24 weeks via cesarean delivery. Women were excluded if they had (1) a positive test for gonorrhea or chlamydia in this pregnancy; (2) a uterine anomaly that was known to distort the uterine cavity; (3) known or suspected cervical, uterine, or breast neoplasia; (4) an allergy to any component of the chosen IUD; (5) a diagnosis of chorioamnionitis, intrapartum fever, or ruptured membranes for greater than 24 hours before delivery.
All study activities adhered to the CONSORT guidelines 10 for reporting clinical trials.
After the consent process was completed, women were randomized to intracesarean IUD placement or interval IUD insertion at 6 or more weeks after delivery. Once randomization was complete, women could choose either an LNG-IUD (Mirena®; Bayer Healthcare Pharmaceuticals, Whippany, NJ) or a Copper IUD (ParaGard®; Teva Women's Health, Sellersville, PA). Women were assessed at a follow-up visit at 6 weeks, 3 months, and 6 months postpartum. IUDs were provided free-of-charge, and women were reimbursed a nominal amount for each study visit.
To assess breastfeeding status, women were asked whether or not they were breastfeeding at each follow-up visit. The primary outcome of this secondary analysis was continuation of any breastfeeding at 6 months in women who were randomized to either group and received an IUD. If women were not breastfeeding during the study period, they were asked why they were not breastfeeding.
Statistical analysis was performed using Stata 14.2 (College Station, TX). Primary analysis used the intention-to-treat data. Means were compared using t tests, and proportions were compared using Pearson's χ2 for the primary outcome. Logistic regression was used to determine the odds of breastfeeding at 6 weeks, 3 months, and 6 months postpartum, with adjustments for age, parity, and ethnicity.
Results
One hundred seventy-two women were screened to reach our final enrollment group of 112 (Fig. 1). Fifty-six women were allocated to the intracesarean group; of these, 53 women (95%) received their assigned IUD at the time of cesarean delivery (Fig. 1). Three women did not have their IUD placed at the time of cesarean delivery because the surgical team did not remember or did not know to place the device. Two of these women subsequently had an IUD placement at their postpartum visit. Among the women randomized to the intracesarean group, 40 (73%) chose an LNG-IUD and 15 (27%) chose a Copper IUD. Fifty-six women were allocated to interval IUD insertion; of these, 34 women (63%) had an IUD successfully placed: 30 (86%) chose an LNG-IUD and 4 (14%) opted for a Copper IUD.
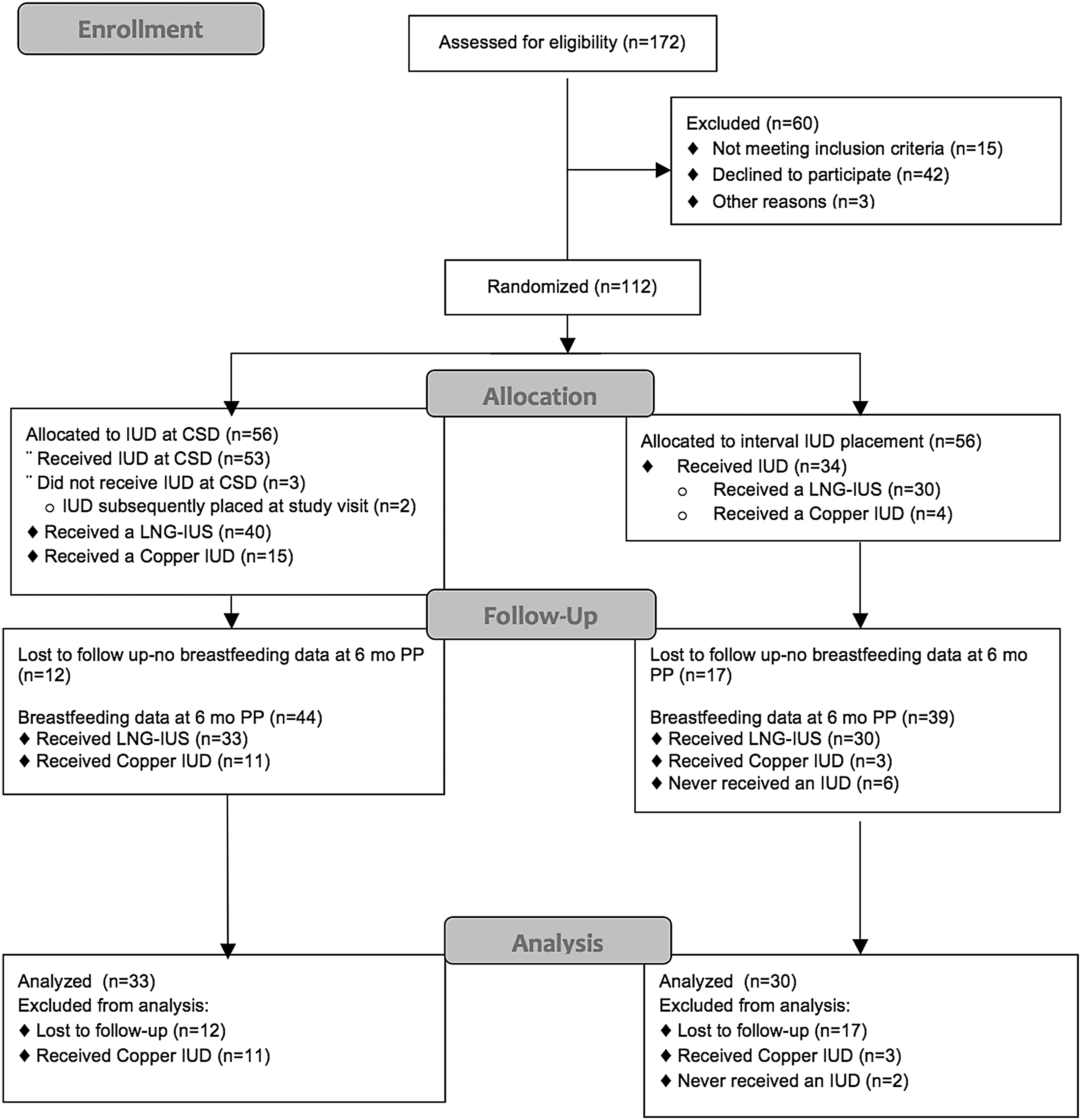
Flowchart of study participants. LNG-IUS, levonorgestrel-releasing intrauterine system; IUD, intrauterine device.
We received breastfeeding information from 83 women at 6 months postpartum. Of these 83 women, 14 had a copper-containing IUD placed and 63 had an LNG-containing IUD placed. Two of these women had been randomized to the interval group but never had an IUD placed. They were excluded from the analysis. Our final analysis groups comprised participants who chose to use an LNG-IUD from whom we collected breastfeeding data at the 6-month visit; 33 women in the intracesarean arm and 30 women in the interval arm.
There was no difference in age, parity, race/ethnicity, or breastfeeding rates in women who had a copper IUD placed compared with those who had an LNG-IUD placed. The analysis was limited to women who had an LNG-IUD placed due to the theoretical interaction between progestins and lactogenesis. Demographics from these 63 women included in the analysis are shown in Table 1. The average age was 28.9 (±5.7) years, and the participants were mostly white (49.2%), married (49%), and had one previous delivery (49%). One woman reported race/ethnicity as “something else” and was excluded from the logistic regression analysis.
Two missing.
Seven refused.
SD, standard deviation.
A logistic regression analysis noted that there was no difference in the odds ratios of women breastfeeding at any of the three time points, 6, 12, and 24 weeks, following the placement (Table 2). After adjusting for age, parity, and ethnicity, there was no difference in the odds ratios of the women breastfeeding at any of the three time points (Table 3). Among women who received an LNG-IUD, there was no difference in the reasons that women provided for stopping breastfeeding (Table 4). Three more women in the immediate placement group reported inadequate milk production than in the interval placement group (8 women versus 5 women); however, this difference was not statistically significant.
Parity before delivery.
CI, confidence interval; OR, odds ratio.
Discussion
In this study, immediate postplacental placement of a hormonal IUD did not affect women's breastfeeding success or duration. Immediate postplacental IUD placement is becoming more widespread. The American College of Obstetricians and Gynecologists (ACOG) recently released a committee opinion and practice bulletin 11 supporting this practice, 4 and increasingly, state Medicaid policies are offering reimbursement for devices placed during an admission for delivery. 12 Despite the growing popularity of immediate postpartum IUD placement, we are still lacking high-quality data on the effect that immediate postplacental placement of hormonal IUDs may have on breastfeeding outcomes, if any.
This study adds to the existing body of evidence that shows that most women are able to successfully breastfeed after immediate postpartum placement of a hormonal IUD. According to the CDC Medical Eligibility Criteria, hormonal IUDs are a category 2 in the immediate postpartum period for breastfeeding women, meaning that the benefits of this method likely outweigh the risks. 8 Breastfeeding, and appropriate birth spacing, have important benefits for both mothers and babies.13–15 Women should be encouraged to breastfeed in accordance with the ACOG and the American Academy of Pediatrics recommendations,15,16 but the intention to breastfeed should not preclude the initiation of an effective method of contraception, including a postplacental IUD.
The design of this study is one of its strengths—it is both randomized and longitudinal, allowing for assessment of breastfeeding duration over the entire 6-month period. These data also have several limitations. This is a secondary analysis of a randomized trial that was not designed to look at breastfeeding outcomes and therefore lacks the necessary power to determine any between-group differences. Additionally, all breastfeeding data were self-reported and women were not asked about breastfeeding exclusivity, formula supplementation, or infant growth. However, while the data were self-reported, the data are robust. It is unlikely that bias for or against breastfeeding would have been present in either group given the randomized design. Given the small number of breastfeeding women who completed the study, caution should be used when interpreting these results. Rigorous data are still needed to clarify the effect of immediate postpartum use of hormonal IUDs, especially in women known to be at risk for low-milk supply.
Conclusion
Women should be counseled that immediate postpartum IUDs decrease the risk of unintended pregnancies in the postpartum period and help women to achieve adequate birth spacing. 4 Women who are intending to breastfeed should be reassured that thus far studies show that progestin-only contraception in the postpartum period does not affect most women's ability to breastfeed. 17 However, data are lacking for women who are at risk for low-milk supply, including women with diabetes, polycystic ovarian syndrome, preterm delivery, and obese women. Given the lack of complete data for many women at risk of low-milk supply, and the importance some women may place on breastfeeding and birth spacing, a patient-centered approach should be taken. Healthcare providers can elicit women's preferences and values regarding their desires to breastfeed and their need for contraception and provide guidance with decision-making based on each individual patient's risks and desires.15,18 All women who experience low-milk supply should be encouraged to seek help from their OBGYN, pediatrician, or certified lactation consultant. As always, IUDs should be removed at a patient's request, for any reason, including concerns regarding milk supply.
Footnotes
Acknowledgments
We wish to thank Karen Dorman and her research team, all the residents, clinical staff, and clinical faculty at the University of North Carolina at Chapel Hill for their enthusiastic support for the study. This project was funded by the Society of Family Planning Research Fund. Teva Women's Health provided the Copper T380A devices for this project. The project was supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health (NIH), through Grant Award Number 1UL1TR001111. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Disclosure Statement
No competing financial interests exist.