
Abstract
Abstract
Background:
Infant formulas are produced to resemble human milk (HM) and to provide adequate energy and appropriate nutritional components for suitability of infant growth and development, some of which are customized for specific medical conditions. However, it has remained unclear whether formulas contain any biofunctionality equivalent to HM, particularly fetal intestinal cell growth promotion.
Objective:
To evaluate the biofunctionality in HM and various formulas by using an in vitro fetal intestinal cell growth assay.
Materials and Methods:
Nine specimens of HM collected from 9 milk donors and 16 formulas consisting of 5 regular formulas (RFs), 2 preterm formulas (PFs), 2 partial hydrolysate formulas (PHFs), 3 extensive hydrolysate formulas (EHFs), 2 amino acid formulas (AAFs), and 2 soy protein formulas (SPFs) were included. Fetal intestinal cell growth assay was performed in six replicates per milk specimen. Biofunctionality of HM digest (HMD) derived from in vitro tryptic digestion of HM was also examined. Statistical analysis was performed by ANOVA with post-hoc Tukey's Honestly Significant Difference test.
Results:
The fetal intestinal cell growth-promoting activity of HM and formula groups were sorted from the highest as follows: HM, 192.8% ± 16.7%; AAF, 153.5% ± 17.8%; EHF, 149.4% ± 12.5%; RF, 123.5% ± 14.2%; PHF, 111.2% ± 17.9%; PF, 110.3% ± 8.2%; and SPF, 109.3% ± 17.3%. Statistical analysis showed that growth promotion of HM was significantly higher than that of all examined formulas (p < 0.0001). Among formulas, EHF and AAF showed greater growth-promoting activity than the others (p < 0.0001). HM and HMD had a comparable growth-promoting effect on fetal intestinal cells (198.5% ± 27.9% versus 191.2% ± 17.9%, p = 0.724), supporting the potential impact of HM biofunctionality under physiologic gastrointestinal digestion.
Conclusions:
Our data suggested that formulas are not equivalent to HM in respect of fetal intestinal cell growth biofunctionality. Despite having less activity than HM, EHF and AAF exhibited considerable levels of growth-promoting effect that may have clinical implications, especially when HM is unavailable.
Introduction
T
There are many formulas available in the market. In general, formulas are classified by protein sources (e.g., cow's milk or soy protein), cow's milk protein composition (i.e., whole proteins, hydrolyzed proteins/peptides, or amino acid), carbohydrate content (e.g., lactose or lactose free), and calorie density (i.e., 20 kcal for term infants or 24 kcal for preterm formula, PF). Formulas are produced to resemble HM and to provide adequate energy and nutrition for term infants, whereas several formulas are customized for specific reasons, for example, higher energy density and protein contents for catch-up growth in preterm infants, cow milk protein allergy, or lactose intolerance after gastroenteritis. Iron supplement in all formulas prevents infants from iron deficiency anemia, and with this respect, formulas may be considered functional food for infants as well. Despite the benefits of using suitable formulas solely or combined enteral nutrition for infants in some circumstances and clinical contexts, it has remained unclear whether the formulas contain any biofunctionality comparable with that of HM.
Fetal intestinal epithelium lining along gastrointestinal tract is one of the first tissues that interact with enteral nutrition during the early stages of an infant's life. Promotion of fetal intestinal cell growth and survival is, therefore, a crucial HM biofunctionality that facilitates intestinal maturity and prevents necrotizing enterocolitis (NEC) in preterm infants. Several trophic factors in HM such as epidermal growth factor (EGF) and insulin-like growth factor may be responsible for this protective effect.10–12 Previous studies demonstrated that HM could directly induce fetal intestinal cell growth in vitro.13,14 To the best of our knowledge, however, there is no such functional data derived from infant formulas available at present.
This study then aimed to compare fetal intestinal cell growth biofunctionality of HM and various formulas by using an in vitro cellular assay.
Materials and Methods
This experimental study was conducted at Department of Pediatrics, Faculty of Medicine Ramathibodi Hospital, Mahidol University, during July 2016–June 2017. This study was approved by the Ethical Clearance Committee on Human Rights Related to Research Involving Human Subjects, Faculty of Medicine Ramathibodi Hospital, Mahidol University (protocol ID 10-57-27).
HM collection
After informed consent, HM (30 mL) was collected by a breast pump at Ramathibodi Human Milk Bank and was immediately transferred on ice to keep in a −80°C freezer at the research unit. HM collection was performed within 1 month period. Mothers of full-term infants, during 2-week to 6-month lactation period, were eligible to enroll in this study. Exclusion criteria were the presence of any underlying diseases or abnormal results of anti-HIV, hepatitis B surface antigen (HBsAg), or the venereal disease research laboratory (VDRL). Demographic data including maternal age (year), body weight (kg), parity, gestational age (week), birth weight (g), and postpartum age (day) were collected at the time of milk donation.
Infant formulas
Sixteen formulas that are commonly available in convenience stores in Thailand were included. These consisted of five brands of regular formulas (RFs; S-26 SMA [Wyeth], Hi-Q Super Gold [Nutricia], Dulac1 Super Mix [Dumex], Enfalac A+ [Mead Johnson], and Similac LF [Abbott]), two brands of PFs (Similac NeoSure [Abbott] and Enfalac A+ Premature [Mead Johnson]), two brands of partial hydrolysate formulas (PHFs; Hi-Q H.A.1 Prebio ProteQ [Nutricia] and Nan Optipro HA1 [Nestle]), three brands of extensive hydrolysate formulas (EHFs; Pregestimil DHA&ARA [Mead Johnson], Nutramigen LGG [Mead Johnson], and Hi-Q Pepti Prebio ProteQ [Dumex]), two brands of amino acid formulas (AAFs; Puramino [Mead Johnson] and Neocate LCP [Nutricia]), and two brands of soy protein-based formulas (SPFs; Isomil AI.Q plus [Abbott] and Hi-Q Soy [Nutricia]). Formula powder was dissolved in warm sterile water at the proportion (weight per volume) recommended by each manufacturer's instructions. All formulas were prepared and tested at least 6–12 months before their expiration dates.
Fetal intestinal cell growth assay
Fetal intestinal cells (FHs74Int; ATCC®CCL241) were purchased from the American Type Culture Collection (ATCC, Manassas, VA), propagated, subcultured, and stored as seed stocks as described previously. 13 To measure the growth-promoting activity, FHs74Int cells were placed in Dulbecco's modified Eagle's medium (DMEM) (Gibco, Paisley, Scotland) containing 10% fetal calf serum at a concentration of 5 × 10 3 cells/well in a 96-well plate for 24 hours at 37°C, 5% CO2 and then washed by serum-free DMEM to eliminate serum protein contamination. Thereafter, FH74Int cells were cultured at a final concentration of 10% HM (or 10% formula) in DMEM (Gibco) for 24 hour. Cell proliferation was measured by MTT (3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide) assay at an absorbance of 690 nm (AU690) as per manufacturer instructions (Promega Corporation, Madison, WI). FHs74Int cell culture in serum-free media served as a blank control, whereas a supplement of 3 ng EGF served as a positive condition. The measurements were performed in six replicates to ensure the accuracy of the functional data. Growth-promoting activity was calculated by the following equation: Growth-promoting activity (%) = 100 × (AU690 of milk supplement/AU690 of serum-free media) (Equation 1).
In vitro digestion of HM
To obtain human milk digest (HMD), three HM samples (0.5 mL each) were incubated in the presence of 1:500 (w/w) trypsin (Promega Corporation) at 37°C overnight. Trypsin enzyme exclusively cleaves milk protein molecules at C-terminal to lysine or arginine residues, thus releasing the digested milk peptides into liquid. The HMD (equivalent to 20 mg proteins) was checked for the digestion efficiency by 12.5% SDS-PAGE with Coomassie Blue G-250 staining in comparison with HM. To measure the growth-promoting effect, HMD was added into serum-free DMEM (10% final concentration) before FH74Int cell treatment. This experiment was performed in triplicates per biological specimen. Protein estimation was performed by Bradford assay (Bio-Rad Laboratories, Inc., Hercules, CA).
Statistical analysis
XLSTAT v.2018.1 (Addinsoft, Inc., New York, NY) was used for statistical analysis. Continuous data are presented as percentage or mean ± SD as appropriate. The statistical difference among groups was examined by analysis of variance (ANOVA) with post-hoc Tukey's Honestly Significant Difference (HSD) test. p-Value <0.05 is considered as statistical significance.
Results
Demographic data of nine independent milk donors are given in Table 1. Sixteen brands of infant formulas were included. Nine HM samples, together with 16 formulas, were then subjected to fetal intestinal cell growth assay.
Figure 1 shows the growth-promoting activities of all milk groups (HM versus various formulas), in which the individual activity data are presented in Table 2. The blank control (serum-free media) had a baseline activity of 100%, whereas the positive control (3 ng EGF treatment) showed a growth-promoting effect of 178.2% (Fig. 1 and Table 2). On average, HM group (n = 9) had the growth-promoting activity of 193.1%, which corresponded to our previous study, 13 whereas RF, PF, SPF, PHF, EHF, and AAF groups had the average growth-promoting activity of 123.6%, 110.4%, 109.4%, 111.5%, 149.6%, and 153.7%, respectively (Fig. 1 and Table 2). As expected, statistical analysis using ANOVA with post-hoc Tukey's HSD analysis showed that the HM group had higher growth-promoting activity than all examined formulas (p < 0.0001) (Fig. 1 and Table 2). Interestingly, EHF and AAF showed growth-promoting activity up to 150% and, therefore, their activities were significantly higher than RF, PF, SPF, and PHF groups (p < 0.0001).

Comparison of fetal intestinal cell growth biofunctionality of HM and various infant formulas. Fetal intestinal cells were treated with 10% milk supplement in serum-free media. Bar graphs represent the average activity of HM group (9 HM samples, 54 technical replicates), RF group (5 brands, 30 replicates), PF group (2 brands, 12 replicates), SPF group (2 brands, 12 replicates), PHF group (2 brands, 12 replicates), EHF group (3 brands, 18 replicates), and AAF group (2 brands, 12 replicates), corresponding to the detailed information given in Table 2. EGF (3 ng) served as the positive condition. Cells treated with serum-free media served as the blank control. A dotted line represents a baseline level of fetal intestinal cell proliferation. ANOVA with post hoc Tukey's HSD test was performed for multiple comparisons. AAF, amino acid formula; EGF, epidermal growth factor; EHF, extensive hydrolysate formula; HM, human milk; HSD, Honestly Significant Difference; PF, preterm formula; PHF, partial hydrolysate formula; RF, regular formula; SPFs, soy protein-based formulas.
AAFs, amino acid formulas; EGF, epidermal growth factor; EHFs, extensive hydrolysate formulas; HM, human milk; PHFs, partial hydrolysate formulas; RFs, regular formulas; SPFs, soy protein-based formulas.
The growth-promoting effect found in bovine milk-based EHF and AAF led to a question that what the potential impact of digestion on the bioactivity of HM. To address this issue, an in vitro digestion of HM was performed using trypsin, a major proteolytic enzyme in the intestines. Figure 2A shows that, after in vitro digestion, all milk proteins in the HM (protein bands with the molecular weight larger than 10 kDa) were cleaved, resulting in the HMD containing milk peptides with molecular weight <10 kDa. The bioactivity of HMD was then examined by fetal intestinal cell growth assay (Fig. 2B). As a result, there was a comparable growth-promoting effect between HM and HMD groups (198.5% ± 27.9% versus 191.2% ± 17.9%, p = 0.724) (n = 3).
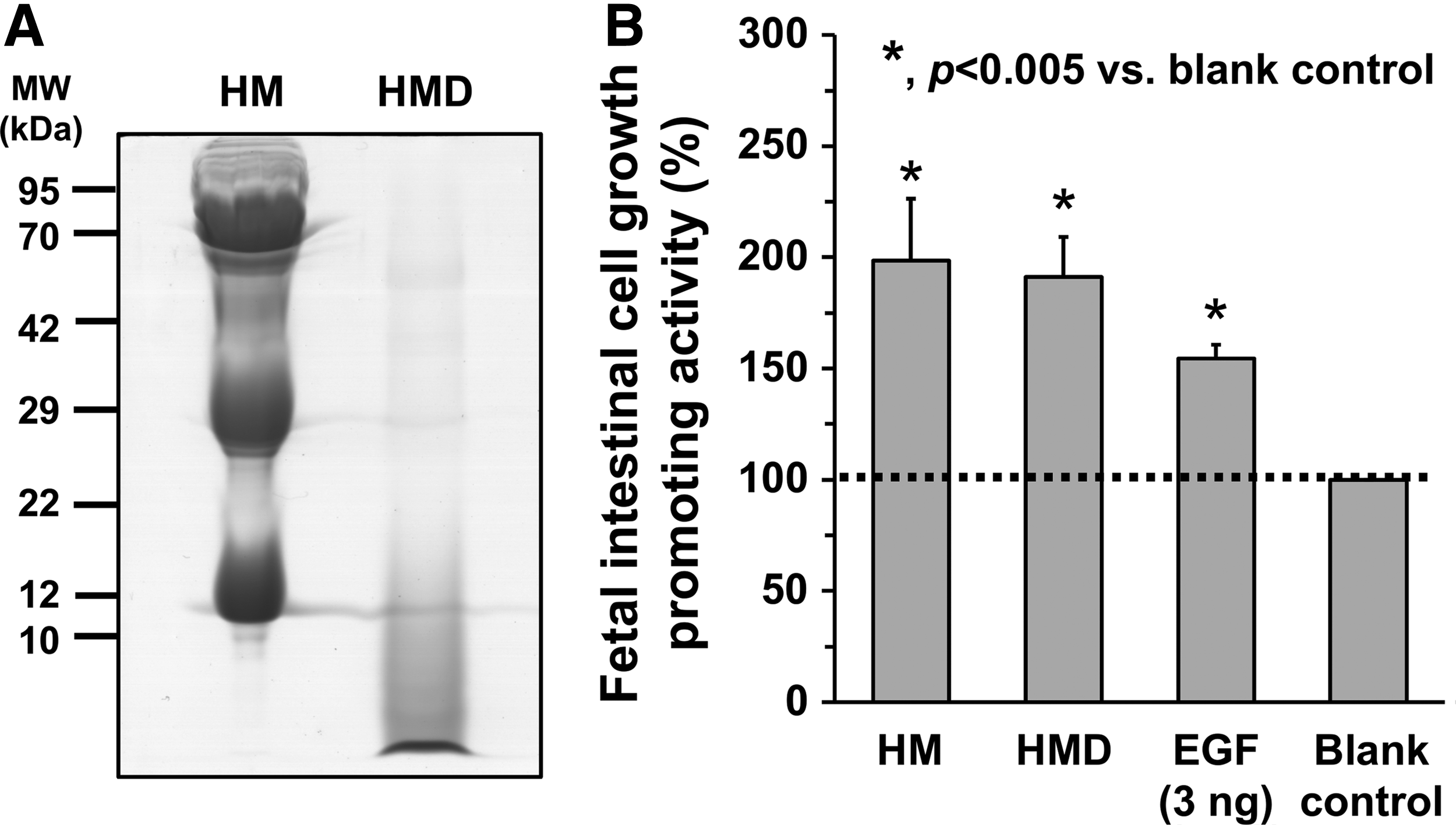
Effects of enzymatic digestion on the fetal intestinal growth biofunctionality of HM. Three HM samples were digested by trypsin enzyme at 37°C overnight to obtain HMD.
Discussion
This study demonstrated direct evidence of fetal intestinal cell growth biofunctionality of HM and various formulas. It is undoubted that HM group had the best growth-promoting activity, as shown by 1.3–1.8 times of this activity comparing with all examined formulas, thereby confirming that HM is the most suitable for the early stages of an infant's life.
From a protein biochemistry viewpoint, a low level of growth-promoting activity toward human intestinal cells of whole protein-based formulas (either cow's milk or soy in origin) may be explained by several possibilities. First, growth-promoting factors in the formulas are modified, inactivated, denatured, or degraded during industrial processing and storage. Second, there is an incompatibility of ligand–receptor binding between nonhuman growth factors presented in the formulas and human protein receptors expressed on fetal intestinal cells. Third, even though this is less likely, cytotoxic factors may be present in the formulas in combination with their growth-promoting effects. Fourth, the growth factors in the formulas are not actionable as intact proteins, but become active forms once digested.
Although further investigations are needed to address the first three issues, our functional data, together with the previous reports,7,15–18 support the last explanation. Studies showed that bioactive peptides and amino acids released from in vitro digestion of cow's milk intact protein exhibited cell growth effects. For example, bioactive peptides resulting from proteolysis of alpha lactalbumin and lysozyme had growth stimulating effect on human fibroblast IMR90 cells. 16 A peptide with growth stimulating activity on rat intestinal epithelial IEC-18 cells had been isolated from the pepsin-generated hydrolysate of bovine lactoferrin. 18 Amino acids, that is, asparagine and glutamine, can regulate intestinal mucosal growth by stimulation of ornithine decarboxylase enzyme, leading to an increase in the synthesis of polyamine, which is required for optimal mucosal growth. 19 Accordingly, the significant growth-promoting activities found in EHF and AAF groups deserve to get attention for a potential translation into clinical benefits. In the context of preterm infants at risk for NEC (or post-NEC) without mother's own milk or donor milk available, choosing EHF (more preferable) or AAF (less preferable) as temporary enteral nutrition over the other formulas is scientifically sound based on fetal intestinal cell growth promotion.
Recently, Lapillonne et al. 20 conducted a national wide survey-based, cross-sectional study in France to determine the frequency of EHF usage in 174 neonatal units, corresponding to a total of 1,969 hospitalized infants. Of 238 infants receiving EHF, shortage of HM (201/238) was the primary reason for EHF prescription, and refeeding infants who recovered from NEC (25/238) was a frequent indication. 20 The investigators pointed out that refeeding of post-NEC infants using EHF, instead of whole protein formulas, prevented cow's milk protein sensitization, which plays a direct contributory role in the pathogenesis of NEC21–23 and probably improved nutrient absorption. 20 Since the growth-promoting activity of EHF may facilitate epithelial mucosal healing of the inflamed intestine in post-NEC infants, our data, therefore, supported the rationale of EHF temporary feeding in this clinical context.
Recognizing that bioactive peptides and amino acids can be released by milk protein hydrolysis and digestion in the gastrointestinal tract, one argument is that after in vivo digestion, whole cow's milk protein-based formulas possibly exhibit a significant growth-promoting effect on fetal intestinal cells also. This argument may be valid in healthy full-term infants. Maathuis et al. 24 showed that in an in vitro model of the gastrointestinal tract, protein digestibility determined by the accessibility of nitrogen and amino acids was not different between cow's milk-based formula and HM. However, they found that cow's milk formula had lower kinetics of protein digestion during 4-hour simulation period. 24 Since preterm infants with a gestational age <32–34 weeks have gut immaturity of anatomic, functional, and biochemical development, 25 it cannot be excluded that these preterm infants probably have delayed (and incomplete) digestion of cow's milk proteins. We speculated that partially digested cow's milk proteins have less beneficial effects based on our functional data of PHF (Fig. 1 and Table 2).
In contrast, it is interesting that HM would have any change in the growth biofunctionality after in vivo digestion in preterm infants. Our findings (as shown in Fig. 2) demonstrated that HMD derived from in vitro tryptic digestion of HM still preserved the growth-promoting effect. These data supported a practical conclusion that HM, in both protein and digested peptide forms, would exert beneficial effects on the infant gastrointestinal tract over the formulas. Further investigation is needed to clarify which bioactive peptides and which intact proteins are responsible for a high activity level toward fetal intestinal cell growth. Addressing these questions at molecular levels has a translational potential into a new therapeutic strategy against NEC.
This study had several limitations. First, fetal intestinal cell growth-promoting activity was measured by the in vitro cellular assay. It is not necessary that positive effects observed in the in vitro condition would also be exhibited in the in vivo context. Instead, this functional data should be used as a marker to guide further clinical studies related to biofunctionality of milk and formulas, or serve as supportive evidence at the cellular level to help make a decision in some clinical contexts. Second, although this study included 16 infant formulas that are commonly available in Thailand, one should be aware that there are varied infant formulas available in other countries. Third, there are not only milk proteins but also nonprotein macro- and micronutrients contained in HM and formulas. These nonprotein components may also contribute to the measured biofunctionality to some extent. Fourth, cell functional studies have relied on the addition of HM (or formulas) to the final 10% concentration in the serum-free media, which was adopted from the standard cell culture protocol of 10% FBS supplement. One should be aware that after ingestion, HM (or formulas) can be mixed and diluted by saliva, gastric juice, pancreatic enzymes, bile acid, and intestinal secretion. Therefore, 10% milk supplement utilized in this study model can be either under- or overestimation. Apart from these limitations, our study conveyed a clear message that HM and its enzymatically digested form have more advantage over formulas in the aspect of growth promotion of immature intestinal cells. We hope this direct evidence at a cellular level, in support of short- and long-term health benefits of HM, would help cement maternal confidence in the exclusive breastfeeding practice.
In conclusion, infant formulas are not equivalent to HM in the aspect of fetal intestinal cell growth biofunctionality. EPH and AAF, despite having less activity than HM, exhibited a significant level of growth-promoting activity that may have clinical implications when HM is unavailable. We encourage manufacturers to reconsider biofunctionality aspects in formulas, and again, confirm by a cellular assay that HM is the best functional food during the early period of infant's life.
Authors' Contributions
S.C. initiated the conception and developed the design. P.K. gave informed consent and collected specimens and clinical data. W.C. coordinated the project and participated in sample and data collection. N.P. performed cellular assays. N.P. and S.C. analyzed the data and prepared figures and tables. N.P. wrote the first draft of the article. P.K., W.C., S.S., P.N., and S.C. revised the article. S.S. and P.N. contributed to overall research strategy. S.C. finalized the article. All authors read and approved the final version of the article.
Footnotes
Acknowledgments
We thank all mothers who donated their breast milk to Ramathibodi Human Milk Bank. We also thank Kanuengnit Emrat, Sirimon Kongthaworn, Achara Tangnoo, and Numtip Tongsawan for their invaluable help on milk donating process. P.K. was a senior pediatric resident at study initiation and a clinical fellow in neonatology at the completion of the project. This study was supported by International Health Policy Program Foundation, Ministry of Public Health, Thailand (IHPF59102559 to SC).
Disclosure Statement
No competing financial interests exist.