
Abstract
Abstract
Background:
The incidence of diabetes is rising, and with it, the number of pregnancies affected by diabetes. U.S. black women have a disproportionately high prevalence of diabetes and lower rates of breastfeeding.
Objective:
The objective of this study was to quantify the relationship between diabetes before pregnancy and breastfeeding duration among black women in the United States.
Materials and Methods:
We analyzed women from the Black Women's Health Study (N = 59,000) to assess the relationship between prepregnancy diabetes and time to breastfeeding cessation occurring up to 24 months postdelivery using Kaplan–Meier survival curves, log rank tests, and Cox proportional hazards models. The study population included primiparous women with births between 1995 and 2009 (N = 3,404). Obesity, hypertension before pregnancy, and family history of diabetes were examined for effect modification.
Results:
Survival curves demonstrated a markedly reduced duration of breastfeeding in women who had been diagnosed with prepregnancy diabetes (p < 0.01). The hazard ratio for breastfeeding cessation for women with prepregnancy diabetes was 1.5 (95% confidence interval 1.1–2.0) compared with women without prepregnancy diabetes after control for age, body mass index (BMI) at age 18, prepregnancy BMI, other metabolic factors, demographics, and health behaviors.
Conclusions:
Our results suggest that prepregnancy diabetes is a strong predictor of curtailed breastfeeding duration, even after control for BMI. This underscores the need for targeted lactation support for diabetic women.
Introduction
The incidence of diabetes is rising, 1 and with it, the number of pregnancies affected by prepregnancy diabetes (PDM), defined as the presence of type 1 or type 2 diabetes at the time of conception. 2 Unfortunately, successful breastfeeding is less likely to occur among women with diabetes, whether that is PDM or gestational diabetes (GDM), defined as diabetes that develops after conception occurs. One possible mechanism for this association could be the impairment of insulin function, which might act at the level of the lactocyte within the mammary gland causing delayed or diminished milk synthesis,3,4 thus reducing rates of successful breastfeeding among women with insulin dysregulation. The evidence for the association between all types of diabetes experienced during pregnancy and breastfeeding rates varies depending on the type of diabetes. There is robust evidence for an inverse association between GDM and breastfeeding initiation and duration,5–10 as well as an inverse association between prepregnancy type 1 diabetes9,11–14 and breastfeeding initiation and duration. There are fewer studies on the association between prepregnancy type 2 diabetes and breastfeeding duration, either alone or as the primary type of diabetes within the combined category of PDM.5–8
Black women have nearly twice the age-adjusted diabetes prevalence (15.5%) compared with white women (8.5%). 15 Black women also have lower breastfeeding initiation rates than women in the general United States population (66.3% versus 81.4%). 16 When compared with women of other races with PDM, it is unclear whether black women with PDM successfully initiate breastfeeding more or less often. In three studies, all in Ohio, one study on a hospital population demonstrated lower breastfeeding initiation among black women with PDM compared with white women with PDM. 17 The remaining two studies utilizing birth certificate data found a difference in the association by race such that among non-Hispanic white women, those with PDM had lower rates of breastfeeding initiation compared with women without diabetes, but among non-Hispanic black women, breastfeeding initiation rates were higher for women with PDM compared with those without.6,7 The only study on the association between PDM and breastfeeding duration after hospital discharge includes black women (12% of total population 5 ), but the results were not stratified by race. We used data from the Black Women's Health Study to quantify the relationship between diabetes before pregnancy and breastfeeding duration among black women.
Materials and Methods
A Cox proportional hazards model was created using PDM as the primary exposure and cessation of breastfeeding as the outcome using the Black Women's Health Study, a prospective cohort study of 59,000 self-identified black women ages 21–69. The median age at enrollment was 38. Women were recruited in 1995 largely through subscription lists of Essence magazine (95%), with small numbers of participants from the National Education Association, the Black Nurses' Association, and friends and relatives of respondents. Black Women's Health Study participants represent all regions of the United States. 18 Almost half (44%) had completed college and one in three (35%) were nulliparous at the time of recruitment.19,20 Health and demographic data were collected at baseline and follow-up surveys were completed every 2 years. These surveys included questions on births and lactation as well as health behaviors, medical conditions, and sociodemographics. Follow-up through the 2013 questionnaire cycle is complete for 87% of potential person-time. Boston University Institutional Review Board approved the study protocol.
This analysis was limited to women who were nulliparous in 1995 and who had only one live singleton birth from 1995 through 2009 (n = 4,124). Single-child families were the most common type of family (81%) among women who gave birth during this study period. We excluded women with categorical or incomplete data on breastfeeding duration (n = 707) or incomplete prepregnancy body mass index (BMI) (n = 13). The final analytic sample consisted of 3,404 women. Women with PDM who did not report breastfeeding duration were slightly less educated than the analytic sample (≤high school education 18.8% versus 7.9%), but otherwise had similar rates of diabetes and did not differ in any other included covariates.
Prepregnancy diabetes was defined as diabetes reported before pregnancy, inclusive of type 1 and type 2 diabetes. Participants were asked about a list of medical conditions, including “diabetes (not during pregnancy)” at baseline, and on each follow-up questionnaire. If a participant reported GDM and also PDM, she was categorized as having PDM. A validation study of self-reported diabetes (n = 141) demonstrated excellent specificity of self-reports. 21
Lactation duration was ascertained in 2011. Participants responded to the question: “How many months, in total, have you breastfed your children” by filling in the number of months she had breastfed. Since our analysis included women who had only one child, this response represented breastfeeding duration for that single child. There were a total of 865 women who gave birth to their first and only child during follow-up, but did not complete the 2011 questions on breastfeeding. Missing values were replaced for 158 of these women using data from 2003 and 2005, when lactation duration was collected as an integer. The remaining 707 women with missing lactation duration data were not included in the analysis.
The full multivariable model included risk factors for poor metabolic health (prepregnancy hypertension, family history of diabetes, family history of myocardial infarction, GDM, pre-eclampsia, BMI before pregnancy, and BMI at age 18) along with covariates for health behaviors (diet, exercise, smoking status, alcohol use) and demographics (education, marital status, and race of neighborhood). Covariates included metabolic risk factors and health conditions as well as demographics and health behaviors. Hypertension was defined as a report of antihypertensive drug use, or report of physician-diagnosed hypertension together with use of diuretics in the same questionnaire cycle. Two variables for family history of metabolic disease were created using baseline data. A family history of myocardial infarction was defined as the report of one parent having experienced myocardial infarction; similarly, a family history of diabetes was defined as one parent having experienced diabetes. Prepregnancy BMI (kg/m 2 ) was calculated using height at baseline and the most proximal weight to the survey in which the birth occurred. BMI at age 18 was calculated from baseline height and weight at age 18, recalled by participants at the time of recruitment. In a previous validation study of self-reported anthropometric measures among 115 participants from the Black Women's Health Study, Spearman correlation coefficients were high between self-measured and technician-measured height (0.93) and weight (0.97). 19 Categories for BMI were defined using World Health Organization categories for normal weight or less (BMI <25), overweight (BMI 25–29.9), obese (BMI 30–34.9), and very obese (BMI ≥35). 22
The following demographic and health behaviors were considered for inclusion in the final multivariable model. Dietary scores using the Dietary Approaches to Stop Hypertension criteria (DASH diet) were created using baseline dietary recall questions. 23 Average hours per week of vigorous exercise (none, <3 hours, and ≥3 hours) and current alcohol use (any, none) were ascertained from the data most proximal to the birth. We used data from the baseline survey to determine smoking status (ever, never) and education (college or more, some college, and high school or less). Education was updated in 2003 if the birth occurred after that questionnaire cycle. Marital status (presence or absence of a current partner) was ascertained from the most proximal data to the birth, available from questionnaires at baseline, 1997, 1999, or 2005. Exposure to breastfeeding was represented using self-defined segregation of current neighborhood in 1999 (predominantly white, mixed, and predominantly black). Age (integer) and year were ascertained from the same questionnaire cycle in which the birth was reported.
We visually inspected Kaplan–Meier survival curves and log rank tests to assess the relationship between PDM and time to cessation of breastfeeding up to 24 months postpartum. We additionally evaluated each indicator of metabolic disease and time to cessation of breastfeeding in the same way (prepregnancy hypertension, family history of diabetes, family history of myocardial infarction, GDM, pre-eclampsia, BMI before pregnancy, and BMI at age 18). We used these results to inform our model building process.
To test for confounding, each variable was individually removed from the fully adjusted model from highest to lowest p-value within the model (backward elimination). We used an a priori change in β coefficient of ≥5% as evidence of confounding. The resulting parsimonious model indicated that it was sufficient to control for just age and BMI at age 18. Because the order of elimination could have an effect on identification of confounding, particularly in highly correlated variables, we performed a sensitivity analysis in which we forced a reversal of the order of elimination between obesity at age 18 and obesity before pregnancy. Results were unchanged. We continued to test model fit by adding first BMI before pregnancy (model 2) and then health behaviors, demographics, and additional risk factors for metabolic health (model 3) to the basic parsimonious model (model 1).
Based on previous literature 24 and the results from Kaplan–Meier curves, we examined obesity, hypertension before pregnancy, and family history of diabetes as potential effect measure modifiers. A two-step process was used. First, each potential effect measure modifier was tested independently in unadjusted models using likelihood ratio tests (LRT) (a priori α-level of p = 0.10). Second, the interaction term for each potential effect measure modifier was added to the fully adjusted model and included in the backward elimination process for confounding as described above. All analyses were performed using SAS version 9.4 software (SAS Institute, Inc., Cary, NC).
Results
Among the 3,404 women who reported one singleton live birth in the study questionnaires from 1997 through 2009, 2.5% (n = 85) reported having diabetes before pregnancy (PDM). Among all 3,404 mothers, 22% breastfed for at least 12 months, and 6.7% were still nursing at 2 years (data not shown). Breastfeeding initiation was lower in women with PDM (60.0%) compared with those without PDM (81.5%) (Table 1). Women with PDM were also more likely to have metabolic risk factors, including hypertension, family history of diabetes, family history of myocardial infarction, GDM, and obesity, as well as being less likely to exercise, drink alcohol, or have a current partner.
Baseline Characteristics of Women in Black Women's Health Study Who Gave Birth from 1995 Through 2009 by Prepregnancy Diabetes Status
Missing: education (<1%), marital status (<1%), neighborhood (11%), BMI at age 18 (<1%), DASH diet (5.7%), vigorous exercise (<1%), smoking (<1%), alcohol (4%), family history of myocardial infarction (1.6%), pre-eclampsia (16%), family history of diabetes (1.8%).
BMI, body mass index; DASH, Dietary Approaches to Stop Hypertension; GDM, gestational diabetes; PDM, pregestational diabetes; SD, standard deviation.
The crude hazard ratio (HR) for PDM in relation to cessation of breastfeeding among women who initiated breastfeeding was 1.8 (95% confidence interval; CI 1.4–2.5) (Fig. 1 and Table 2). The relationship was somewhat attenuated with adjustment for maternal age and BMI at age 18 (HR 1.6 [95% CI: 1.2–2.2]), which was our parsimonious model. We found additional attenuation with the further addition of prepregnancy BMI (HR 1.5 [95% CI: 1.1–2.1]), but no further attenuation occurred with adjustment for hypertension, family history of diabetes, years of education, diet, or exercise (HR 1.5 [95% CI: 1.1–2.0]).
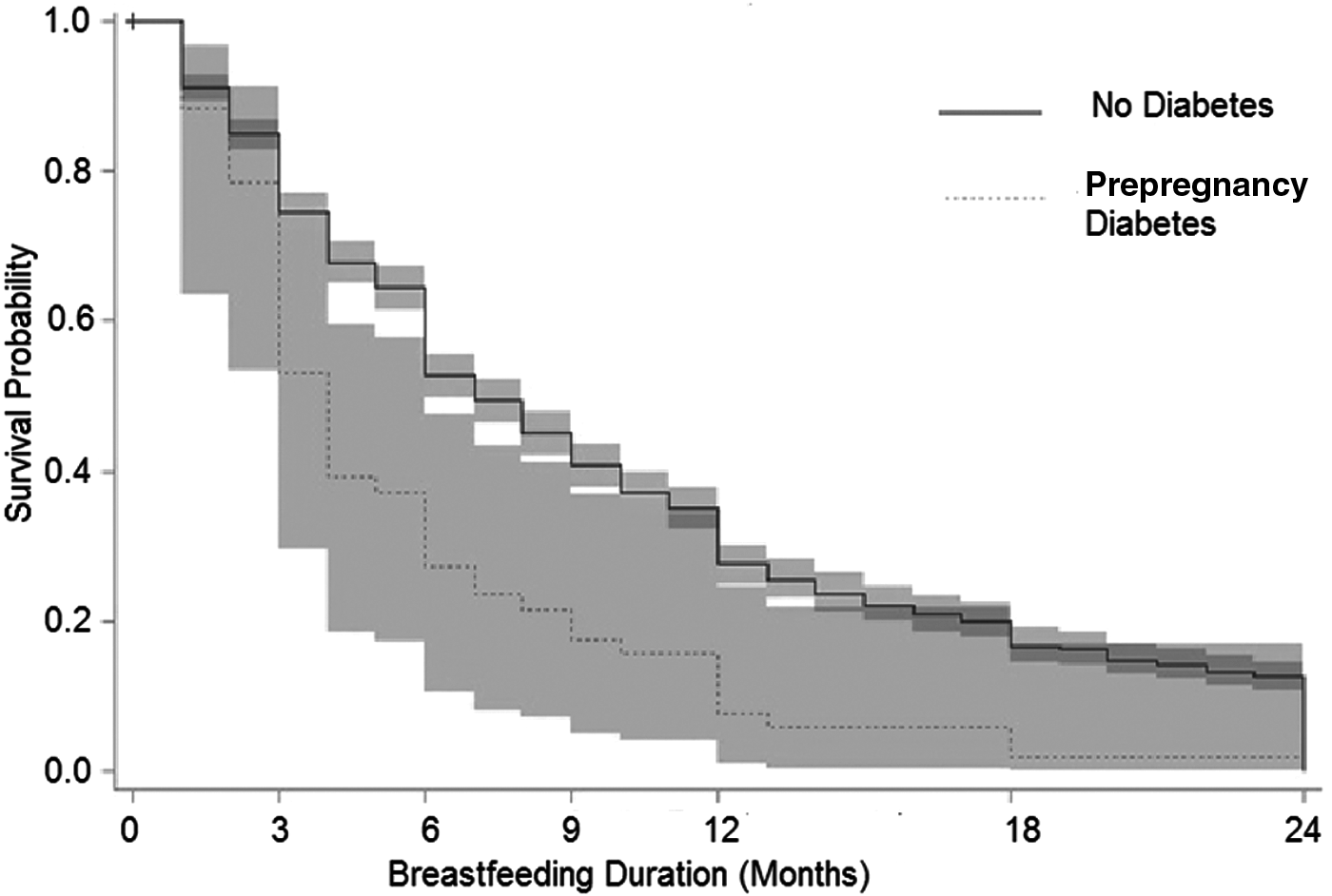
Kaplan–Meier survival curve and 95% equal precision bands for breastfeeding duration in months by prepregnancy diabetic status for women who gave birth to a single child and initiated breastfeeding. Black Women's Health Study 1995–2009 (N = 3,404). 18
Hazard Ratio for Prepregnancy Diabetes in Relation to Cessation of Breastfeeding (N = 3,404, Events = 2,526) Black Women's Health Study, 1997 Through 2009
Model 1 adjusted for age and BMI at age 18.
Model 2 adjusted for model 1 and additionally for prepregnancy BMI.
Model 3, adjusted as for model 1, model 2 and additionally, hypertension, family history of diabetes, education, diet, and exercise.
CI, confidence interval; HR, hazard ratio.
Although our primary interest was in PDM, we evaluated several other indicators of poor metabolic health to estimate their relationship with breastfeeding cessation. Survival curves for cessation of breastfeeding according to prepregnancy hypertension, family history of diabetes, family history of myocardial infarction, GDM, pre-eclampsia, BMI before pregnancy, and BMI at age 18 are shown in Supplementary Figure S1. Prepregnancy obesity, obesity at age 18, and family history of diabetes were associated with cessation of breastfeeding, but crude HRs for those factors (1.3, 1.5, and 1.2 respectively) were substantially lower than the comparable crude HR for PDM (1.8).
In simple hazard models testing for effect measure modification, the association of PDM with breastfeeding cessation differed between women with hypertension (HR 3.6 [95% CI: 2.0–6.4]) and women without hypertension (HR 0.5 [95% CI: 0.8–9.4]; LRT p = 0.03). The association was also somewhat stronger among women with a family history of diabetes (HR 2.0 [95% CI: 1.6–3.1]) compared with those without (1.3 [95% CI: 0.8–2.1]; LRT p = 0.08). These two factors were further tested in the full model using interaction terms, but failed to meet criteria for confounding and therefore were not included in the final parsimonious model. Importantly, BMI at age 18 was a significant confounder, but did not meet criteria for effect measure modification (Fig. 2), nor did prepregnancy BMI (data not shown).
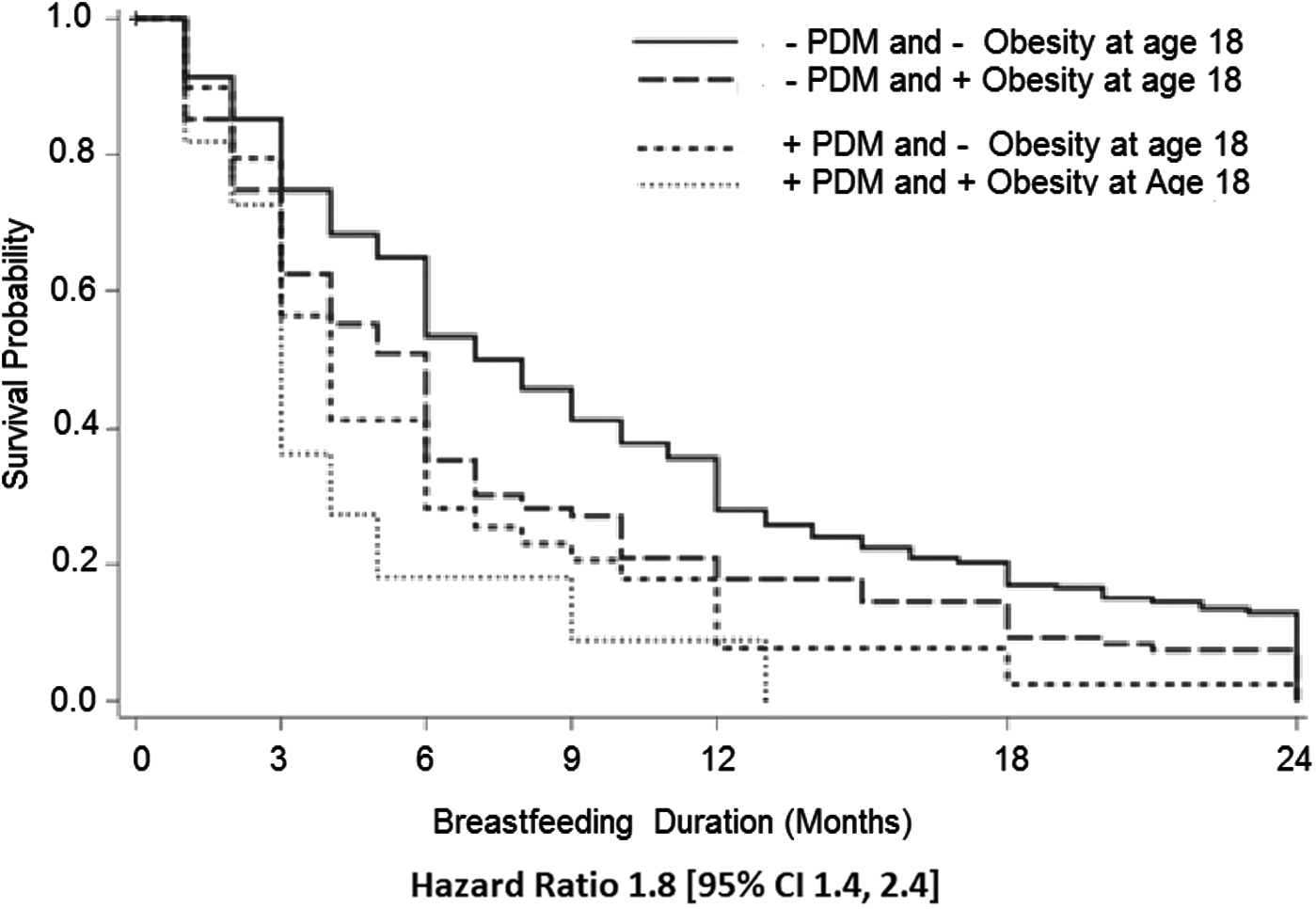
Kaplan–Meier survival curve hazard ratio, and 95% CI for breastfeeding duration in months stratified by prepregnancy diabetic status and obesity at age 18 for women who gave birth to a single child. Black Women's Health Study 1997–2009 (N = 3,404). 18 CI, confidence interval.
Discussion
We found that prepregnancy diabetes was a strong predictor of curtailed breastfeeding duration, even after adjustment for BMI, health behaviors, and sociodemographic characteristics in the African American population. Our study supports similar findings of a reverse association between prepregnancy diabetes and breastfeeding while extending the research base by confirming the association is present when breastfeeding is followed for longer durations. Studies on this topic have demonstrated an association between PDM and lower prevalence of breastfeeding initiation, defined in the study as breastfeeding at hospital discharge,6–8 and with breastfeeding duration, demonstrated at 2 months. 5 Our study followed breastfeeding for up to 2 years after the birth, extending the length of postpartum follow-up, and underscoring the potential benefit of continued breastfeeding support and encouragement beyond the early postpartum period.
Participants in the Black Women's Health Study are all self-identified African American women. Black women have been present in three analyses5–7 ; however, only two of these three studies stratified results by race.6,7 The results from these stratified studies have shown a reduced breastfeeding prevalence in women with PDM overall; however, contrary to our results, in the stratum of black women in both studies, breastfeeding was more common in those women who had PDM than in those who did not.
The prevalence of obesity is almost twice as high for non-Hispanic black women, age 18–45, compared with non-Hispanic white women. 25 Several obesity studies have presented results stratified on race, but none found an association between obesity and prevalence of breastfeeding in black women, even within the same study populations in which there were significant differences among other racial groups.26–28 In contrast to these studies, in our data, breastfeeding cessation was associated with both obesity before pregnancy and obesity at age 18. BMI at age 18 was a stronger confounder of the association of PDM and breastfeeding cessation than was prepregnancy BMI.
It is possible that the two measures of obesity reflect different life histories. Diabetes can be associated with poor metabolic health established early in life. Precursors to obesity, such as poor diet and inactivity, are often established in childhood. 29 Obese adolescents can experience dysregulation of the hormones that are associated with secondary sexual characteristics. 30 We speculate that this dysregulation might impair development of glandular tissue during breast development. Through this pathway, it is plausible that adolescent obesity may reduce glandular tissue and thereby lead to lower levels of milk production, which is a major cause of early cessation of breastfeeding. Conversely, obesity developing after age 18 would not impact adolescent breast development. Adult-onset obesity may therefore be less confounding to the relationship between PDM and breastfeeding than adolescent obesity. On the other hand, women who were obese during adolescence typically remain obese, so it is also possible that the difference in the strength of confounding between obesity at age 18 and prepregnancy obesity was not a biological difference but caused by the inclusion of the women who were obese at age 18 in both BMI variables.
Our findings must be interpreted within the context of the study design. This analytic study population was composed of women who had a single child during the study parameters. Participants were also at least 23 at the age of their first and only birth, and had higher levels of education as well as a higher prevalence of breastfeeding than the overall population of black women in the United States. 16 Consequently, the results are generalizable to first births, and may not be generalizable to all black women in the United States, particularly those with large families or without education past high school. Additionally, breastfeeding was measured using total duration, and did not include exclusivity or intensity, reducing sensitivity to specific breastfeeding difficulties, such as low milk production. For some women in the study population, data on breastfeeding duration might have been obtained years after breastfeeding occurred, introducing the possibility of recall bias; however, a study of breastfeeding recall in the Black Women's Health Study indicates reasonable reliability, 31 in accord with reports from other studies.32–34
Reasons for breastfeeding initiation and continuation are complex, particularly when the pregnancy or birth is complicated. One of the limitations of our study was that we did not include perinatal events, such as mode of delivery, or neonatal complications such as hypoglycemia, nor were we able to account for intention to breastfeed. On the other hand, a strength of our study was our use of a time-to-event model which assessed the association through 2 years of the postpartum period, rather than limiting the assessment to prevalence at particular time points or to a shorter postpartum period.
Conclusions
In conclusion, the findings from our study confirm and extend our knowledge of PDM and its association with breastfeeding. Black women with PDM were less likely to initiate breastfeeding and ceased breastfeeding earlier than those without PDM. As the prevalence of type 2 diabetes is about twice as high in U.S. black women as compared with white women, these associations may contribute to racial disparities in breastfeeding. Our results underscore the importance of targeted breastfeeding support, particularly among women with diabetes.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.