
Abstract
Abstract
Background:
Morbidly placenta accreta as a cause of postpartum morbidity is increasing in incidence. One conservative option is use of methotrexate as an adjuvant therapy for the management of placenta accreta. There is concern that use of methotrexate in a lactating mother could potentially expose her neonate to harmful effects of this medication.
Case Report:
Here we report a 29-year-old woman subjected to methotrexate treatment for placenta accreta. Her child was delivered at 32 weeks weighing 3 lbs. On postpartum day 5, this patient was diagnosed with placenta accreta and treated with intramuscular methotrexate for 3 consecutive days. She received 92 mg methotrexate intramuscularly daily, and was advised not to breastfeed. She collected milk samples on day 2, the 0 hour before the second dose and at 1, 2, 4, 8, 12, and 24 hours after taking the dose. A high-performance liquid chromatography mass spectrometry method was developed to measure methotrexate and its metabolite 7-hydroxymethotrexate levels in milk samples.
Discussion:
Very low levels were found for both methotrexate and 7-hydroxymethotrexate in the milk samples obtained. The results indicate that methotrexate or its metabolite receded to minimum concentration over a period of 24 hours.
Conclusion:
This case report found the relative infant dose of methotrexate to be 0.11%. Methotrexate does transfer into breast milk, although the levels detected were very low. However, caution should still be used in counseling mothers regarding breastfeeding with this toxic drug.
Introduction
M
The objective of this study was to determine the transfer of intramuscular (IM) high-dose methotrexate and its metabolite into milk samples of a lactating woman undergoing treatment for placenta accreta.
Case Presentation
Here we report a 29-year-old woman (180 lbs body weight) who received methotrexate treatment for placenta accreta. Her child was delivered at 32 weeks weighing 3 lbs. On postpartum day 5, she was diagnosed with placenta accreta and treated with 92 mg (1.12 mg/kg) methotrexate IM for 4 consecutive days. She was advised not to breastfeed. The mother volunteered to provide milk samples to determine methotrexate levels. On day 2, she collected samples at 0 hour, and additional samples at 1, 2, 4, 8, 12, and 24 hours after the dose. The samples were frozen at −20°C and mailed to our research facility overnight. When the samples reached our facility, they were stored at −80°C until analyzed.
Materials and Methods
A high-performance liquid chromatography mass spectrometry method was developed to measure methotrexate and its metabolite 7-hydroxymethotrexate levels in milk samples. Analyte separation was performed on an Agilent Poroshell column, 50 × 4.6 mm, 2.7 μm. The mobile phase constituted of water and acetonitrile (20:80 v/v), and an isocratic phase was applied with 0.5 mL/min flow rate. Extraction from milk samples was accomplished using protein precipitation with acetonitrile and 5 μL of injection volume was used. The calibration range of 2.4–39 ng/mL was used for methotrexate and 0.3—12.5 ng/mL for 7-hydroxymethotrexate. Data were recorded in single ion monitoring mode, m/z 455.1 for methotrexate and m/z 471.4 for 7-hydroxymethotrexate.
Results
Both methotrexate and its metabolite 7-hydroxymethotrexate levels in milk were exceedingly low. On day 2 of therapy, the methotrexate area under the curve was 205.9 ng·hour/mL and the average milk concentration was 8.6 ng/mL. The maximum concentration (Cmax) of methotrexate occurred at 2 hours and was found to be16.9 ng/mL. The levels gradually receded and were 4.9 ng/mL at 24 hours. The relative infant dose (RID) was calculated at 0.11%. The metabolite, 7-hydroxymethotrexate, was also found at very low levels as compared with methotrexate. The area under curve was observed to be 36.5 ng·hour/mL and its average concentration was calculated to be 1.5 ng/mL with the RID to be 0.02%. All the samples were processed/analyzed in triplicate and graphed as a mean of values obtained. The pharmacokinetics parameters derived for methotrexate and 7-hydroxymethotrexate are summarized in Table 1 and their average concentration curves are shown in Figure 1. These results suggest that the dose of methotrexate or its metabolite to an infant is probably minimal over this 24-hour duration after an IM maternal dose of 92 mg. Interestingly, the peak of 7-hydroxymethotrexate occurred slightly before the peak of methotrexate. Bore et al. in 1987 found that the excretion of methotrexate was ∼10 times faster than the metabolite. Thus plasma levels of the 7-hydroxymethotrexate were prolonged in the plasma and may have accumulated in the milk compartment between doses. 4
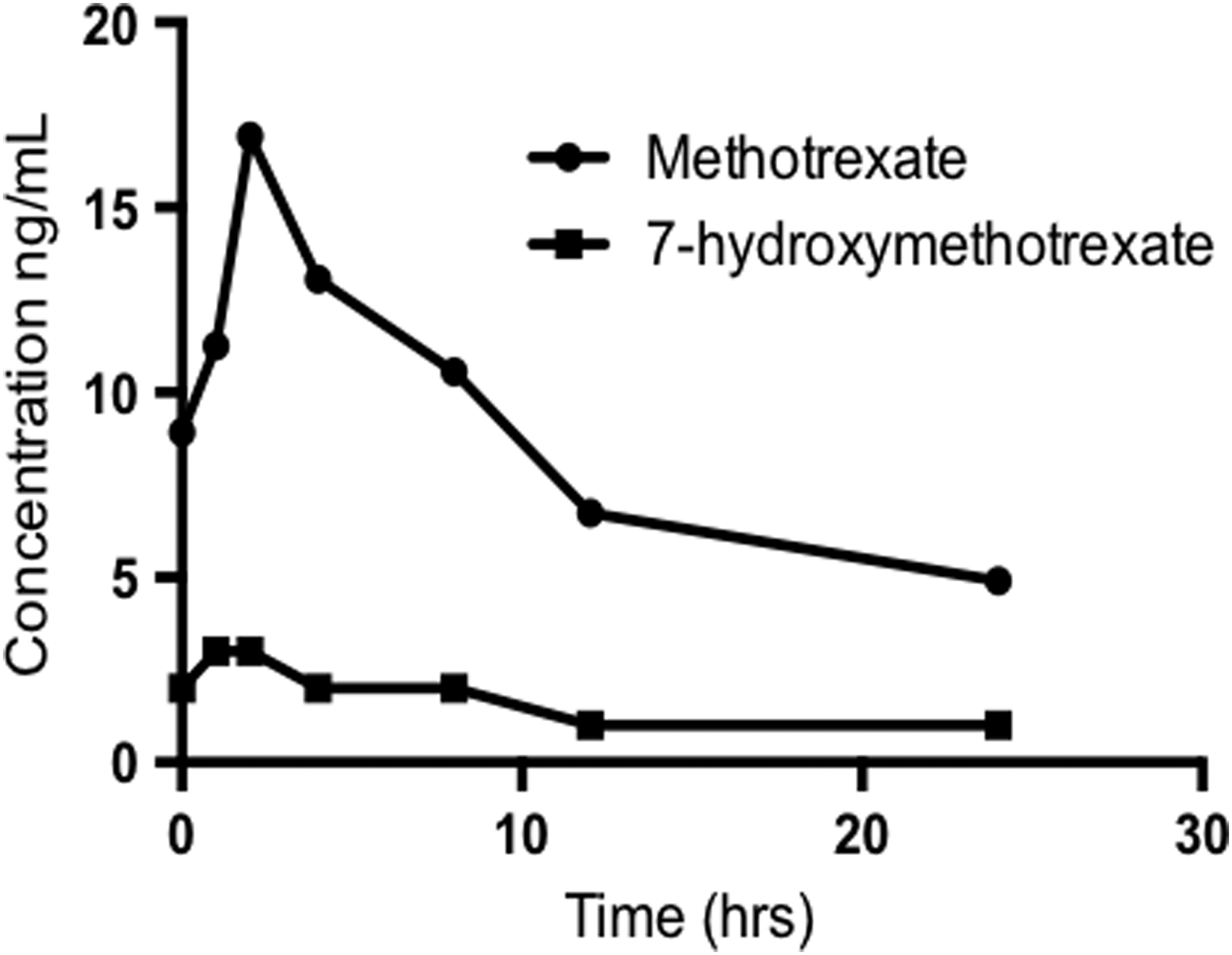
Mean concentration–time profile of methotrexate and 7-hydroxymethotrexate in human milk after 92 mg dose.
AUC, area under the drug concentration versus time curve; Cavg, average drug concentration time interval; Cmax, maximum drug concentration; RID, relative infant dose; Tmax, time at which maximum drug concentration reached.
Discussion
Morbidly placenta accreta is an increasingly common postpartum complication. Conservative management of this condition is emerging as a viable and in some cases optimal option for some patients. Methotrexate is an option for conservative management but little is known about the transfer of IM methotrexate into human breast milk. Methotrexate has been used for other postpartum indications as well, including the treatment of rheumatoid arthritis and other autoimmune disorders, the treatment of ectopic pregnancy, and the treatment of multiple cancers including placental site tumors. In this case, we collected breast milk from a woman on day 2, who was treated with a rather high dose of 92 mg of IM methotrexate daily for 4 days undergoing treatment for placenta accreta. We found the overall absolute infant dose to be 1.2 μg/kg/day and the RID to be only 0.11%. After 24 hours, the remaining levels in breast milk were 4.9 ng/mL. Interestingly, the zero hour levels fell from 8.9 ng/mL on day 1 to 4.9 ng/mL on day 3, suggesting increased metabolism or maternal clearance in the preceding 24 hours. At this time, we do not know the etiology of 55% reduction in milk levels. Because methotrexate is very water soluble, it may be due to rapid renal clearance of water postnatally.
Unfortunately, there are few studies concerning the transfer of methotrexate into human milk. In 1972, a case report was published about a woman who was taking 22.5 mg/day oral dose of methotrexate to treat choriocarcinoma. It was detected in breast milk at a peak concentration of 5 nM (2.27 ng/mL) at 9 hours, whereas maximum serum levels were reported to be 1.8 nM (0.73 ng/mL) at 6 hours with a milk to plasma ratio of 0.08. 5 The authors concluded that methotrexate therapy in breastfeeding mothers would not pose a contraindication to breastfeeding. Another case report from 2014 also reported levels of methotrexate in milk in a 34-year-old multiparous woman, taking a 25 mg of dose subcutaneous. The RID was reported to be 1% of maternal weight adjusted dose. 6 Six milk samples obtained from a woman, who was administered a single IM dose of 65 mg of methotrexate for ectopic pregnancy, were found to have undetectable levels of the given drug (<22.7 μg/mL). 7
Methotrexate is commonly used in pediatric oncology. Doses range from 50 mg/m2 to 12 g/m2. Using the 50 mg/m2 dose, a normal newborn infant would receive <1/1,000 of the calculated infant dose from the milk in this study.
Methotrexate is a powerful folate antimetabolite that inhibits DNA synthesis. Owing to the potential harmful effects of this medication on a nursing infant, caution is recommended when counseling mothers regarding breastfeeding while undergoing treatment with methotrexate. Based on the drug's poor lipid solubility, 98% of methotrexate is polar or lipid insoluble at physiological pH. This could account for its minimal secretion into breast milk. Although this is only a single case report of a rather high dose, more such studies are warranted to determine whether kinetics of transfer are similar for all women.
Conclusions
Methotrexate is a dangerous and potentially toxic antifolate drug that is commonly used in the treatment of arthritis, ectopic pregnancy, and now placenta accreta. Presently, conservative management of placenta accreta with methotrexate is emerging as a viable option for some patients. Unfortunately to date, methotrexate transfer into human milk has been poorly studied. Therefore, breastfeeding an infant after the use of this drug has been somewhat controversial.
In this case report, we found that the RID of methotrexate was exceedingly low, 0.11%, even after a high IM dose early postpartum. Although this is only a single case report, this and other studies suggest that levels in milk are generally low. Thus, mothers could probably be advised to continue breastfeeding their infant after a brief 24-hour interruption after last dose, since the levels detected are so low, and should be subclinical. However, caution should still be used in counseling mothers regarding breastfeeding with this toxic drug.
Footnotes
Acknowledgments
We are very thankful to the woman who volunteered to donate her milk sample without which this case report could not have been possible. We are also very thankful to Gayle Hall for her immense help in the collection of milk samples.
Disclosure Statement
No competing financial interests exist.