
Abstract
Abstract
Background:
This study aimed to compare the effects of adjustable fortification (AF), targeted fortification (TF), and standard fortification (SF) methods on the early growth of very low birth weight infants.
Materials and Methods:
Sixty infants <32 weeks of gestational age and weighing <1,500 g were selected. These infants were exclusively fed with breast milk and were randomized into three fortification groups: SF, AF, and TF. SF consists of adding a fixed amount of fortifier to maternal milk. Blood urea nitrogen levels are used to adjust fortifier in AF. In TF, breast milk is analyzed and fortified accordingly based on the macronutrient content to achieve the targeted intake.
Results:
A total of 76 preterm infants were eligible for the study. Sixty infants were randomized into three groups. At the end of the fourth week of fortification period, median daily weight gain of the infants was similar in the AF [23.5 g/(kg·d)] and TF groups [25.5 g/(kg·d)], and significantly higher in both groups than in SF group [12 g/(kg·d)] (AF versus SF group, p < 0.001 and TF versus SF group, p < 0.001). Weight, head circumference, and length were compared across the three groups regarding percentile. Significant improvement in the percentile groups of weight and head circumference was observed in the AF and TF groups. In the SF group, a significant decline in the percentile groups of weight, head circumference, and length was detected. Daily protein and energy intakes in AF and TF groups were significantly higher than those in SF group (SF versus AF, p < 0.001 and SF versus TF, p < 0.001).
Conclusions:
Fortifying breast milk with AF and TF methods was found to improve body weight, length, and head circumference percentiles of preterm infants, whereas SF method was found unsatisfactory. To provide optimum growth for preterm babies, breast milk that has been fortified by using AF and TF strategies should be recommended in neonatal intensive care units.
Introduction
Breast milk is the best option for very low birth weight (VLBW) infants because of its immunoprotective, nutritional, and psychological properties. It has both short- and long-term beneficial effects for VLBW infants.1,2 However, breast milk alone is not adequate to provide the recommended needs of growing preterm infants due to nutrient limitations of the milk and high variability in the nutrient content of the milk itself. In neonatal intensive care units (NICUs) that support breast milk for preterm feeding, appropriate fortification strategies are essential for a stable growth period.3,4 Current fortification practices produce significantly improved growth when compared with unfortified maternal milk. 5 There are three ways of fortifying breast milk: standard fortification (SF), adjustable fortification (AF), and targeted fortification (TF). SF is the most commonly used strategy that assumes an average composition of breast milk, and fortifiers are added in a fixed dosage. 6 The amount of fortifier added to milk is based on changes in serial blood urea nitrogen (BUN) levels in AF. Recently, TF strategy based on analysis of breast milk through human milk analyzers (HMAs) is also used to standardize the composition of breast milk.7,8
The most applicable of all these fortification strategies concerning time, cost, and labor is still unclear. Therefore, the experiences of different NICUs will contribute to determining the best feeding regimen in preterm infants.
In this study, we aimed to compare the effects of these three different fortification methods on early growth of VLBW infants in a large tertiary NICU.
Materials and Methods
This prospective randomized controlled study was conducted in Zekai Tahir Burak Maternity Teaching Hospital, NICU in Ankara, Turkey, between January 2015 and December 2015. Clinically stable infants with birth weight (BW) ≤1,500 g and gestational age ≤32 weeks who were fed only with human milk (HM) were included in the study. The study was approved by the Local Ethics Committee/Institutional Review Board, and informed consent was obtained from the parents.
Infants with significant congenital anomalies, respiratory support requirement, sepsis, and those who underwent cardiac and intestinal surgery, or who were receiving mixed feeding (preterm formula/breast milk) were excluded. Seventy-six infants were eligible for the study, and 60 of them were randomized into three groups, with 20 infants in each group (SF, AF, and TF). Sixteen infants were excluded due to transfer to other hospitals and lack of follow-up data.
Parenteral nutrition
Parenteral nutrition was initiated right after delivery for all infants. Intravenous fluid intake was started at a volume of 70–80 mL/(kg·d) with 15–20 mL/(kg·d) increases up to 160 mL/(kg·d). Amino acids (TrophAmine 6%; Baxter, Istanbul, Turkey) were started at a dose of 2–3 g/(kg·d) and reached 4 g/(kg·d) on the third day of life, whereas lipid emulsion (Lipofungin MCT/LCT 20%; B. Braun Melsungen AG, Germany) was started at a dose of 1 g/(kg·d) on the second day of life, reaching 3–4 g/(kg·d) on the fourth day life. Parenteral glucose was started at 6 mg/(kg·min) on the first day of life and increased as tolerated to 12 mg/(kg·min). All enrolled patients received 80–100 kcal/(kg·d) at the end of the first week.
Enteral nutrition
Minimal enteral nutrition with full-strength HM was initiated within the first day of life at a dose of 10–20 mL/(kg·d), and it was increased as tolerated due to the nutrition protocol of the nursery. Parenteral nutrition was gradually reduced to maintain a daily total fluid intake. Full enteral feeding was defined as 160 mL/(kg·d). Milk was unfortified initially.
SF was commenced when the milk intake reached 100 mL/(kg·d) of enteral feeding in all of the study infants. HM was fortified with commercially available fortifier Eoprotin® (Milupa, Germany), which was derived from a cow's milk product. Infants who met the inclusion criteria were randomized into three fortification groups when the feeding volumes reached 160 mL/(kg·d) (full enteral feeding). Randomization was performed by using sequential numbers generated at the computer center of the NICU. The allocations were contained in opaque sequentially numbered sealed envelopes. Infants were followed up for 4 weeks after randomization.
In Group 1 (SF), 1 g (1 scoop) of HMF Eoprotin® (Milupa) was added in every 25 ml of HM. Infants in the SF group received HM fortified with human milk fortifier (HMF) in the standard amount (2.3 g/100 mL of HM). HMF provided 0.8 g of protein and 10 calories per 100 mL of breast milk.
In Group 2 (AF), infants were also fed with an SF regimen at the beginning. The AF was based on BUN levels tested twice a week and performed according to the study by Arslanoglu et al. 9 Protein supplement (Milupa Aptamil® protein supplement) was added to HM according to BUN results.
Fortification started at level 0 (0.8 g protein/100 mL) and reduced one level when the BUN level was >14 mg/dL or increased one level when BUN was <9 mg/dL.
In Group 3 (TF), breast milk analyses were performed at two different days of the week in the morning from batches collected by mothers to measure the protein content of breast milk for each infant. Milk samples that were collected and frozen by mothers for 24–72 hours were thawed. A 1.5 mL aliquot from each batch of thawed breast milk was used for macronutrient analysis. Thawed milk samples were homogenized using an ultrasonic homogenizer (Sonicator®, Uppsala, Sweden) and analyzed using a HMA (Miris®, Uppsala, Sweden). An appropriate amount of protein supplement was added right before the milk was consumed to achieve target protein intakes that the infant needs. The additional protein levels were calculated by the European Society for Pediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) recommendations. The goal was to reach daily protein intake of 3.5–4.5 g/kg. 1
Characteristics of the infants were initially recorded. Anthropometric measurements (daily weight gain and weekly increase in head circumference and length of the infants) were recorded both at the beginning of the study period [when the feeding volumes reached 160 mL/(kg·d), and randomization occurred] and during the 4 weeks after randomization. All measurements were performed by trained nurses; all nurses were experienced in the neonatal care, and they were blind to the study groups. Body weight was measured daily using electronic scales (±10 g). On average, at least two measurements were taken. The length was measured at every week by two measures to the nearest 0.1 cm using a measuring board with a fixed headboard and movable footboard. Head circumference was measured around the widest part of the occipital frontal circumference, twice weekly to the nearest 0.1 cm using a nonstretch tape measure. Weight gain in grams per day was calculated as the difference between the initial and the final weight, divided by the number of days elapsed, and this was converted to grams/(kilogram per day) by dividing gain in grams per day by the average weight during the observation period.
Results and measurements are expressed as percentiles. Percentiles were categorized according to international percentile curves. 10
The infants were considered to have completed the study if they undertook 4 weeks in the study.
Feeding intolerance (gastric residuals, abdominal distension, and withheld feedings), the frequency of defecation, and vomiting were evaluated daily. Calcium, phosphorus, and alkaline phosphatase (ALP) levels were obtained every week during the study period. Weekly analyses for blood gases were performed. Serum urea, calcium, phosphorus, ALP levels, and blood gases were detected with automatic analyzers using routine laboratory techniques (Siemens® ADVIA 2400 biochemistry analyzer).
Statistical analysis
Data were analyzed using SPPS version 21. Data are expressed as a median (interquartile range). All analyses were performed with nonparametric tests because of a low number of patients in the groups. Kruskal–Wallis test was used to compare continuous variables across the groups, and chi-square test was used to analyze differences in categorical variables. The primary outcome of the study was the change in the percentile of body weight, head circumference, and height before and 4 weeks after the initiation of fortification. Percentiles were grouped in ordinal six-ordered categories: <3% as Group 1, 3–10% as Group 2, 10–50% as Group 3, 50–90% as Group 4, 90–97% as Group 5, and >97% as Group 6. Pre- and postfortification percentile group distributions were compared using the marginal homogeneity test for nominal/ordinal variables. p-Value <0.05 was considered to be statistically significant.
Results
A total of 60 preterm infants were randomized into three groups, with 20 infants in each group (SF, AF, and TF). Baseline characteristics of the groups were similar concerning gestational age, BW, head circumference and length at birth, Apgar scores, morbidities of prematurity, and age at randomization (Table 1).
General Characteristics of Study Populations
AF, adjustable fortification; BPD, bronchopulmonary dysplasia; NEC, necrotizing enterocolitis; PDA, patent ductus arteriosus; RDS, respiratory distress syndrome; ROP, retinopathy of prematurity; SF, standard fortification; TF, targeted fortification.
At the end of 4 weeks, median daily weight gain of the infants was similar in AF [23.5 g/(kg·d)] and TF groups [25.5 g/(kg·d)] and significantly higher in both groups than in the SF group [12 g/(kg·d)] (AF group versus SF group, p < 0.001 and TF group versus SF group, p < 0.001) (Table 2).
Growth Characteristics of the Infants
Data shown as median (interquartile range).
HC, head circumference.
At the end of 4 weeks, significant improvement in the percentile groups of weight and head circumference was observed in the AF and TF groups. In the SF group, a significant decline in the percentile groups of weight, head circumference, and length was detected. Changes in the percentile groups of the fortification groups are shown in Table 3.
Infants in Each Percentile Group Before and After 4 Weeks of Fortification Period
Marginal homogeneity test, pre- versus postvalues.
Weight percentile did not deteriorate in any of the infants in AF and TF groups.
Shifts in percentile groups in relation to weight, head circumference, and length after 4 weeks of fortification period across the three groups are shown in Figure 1a.
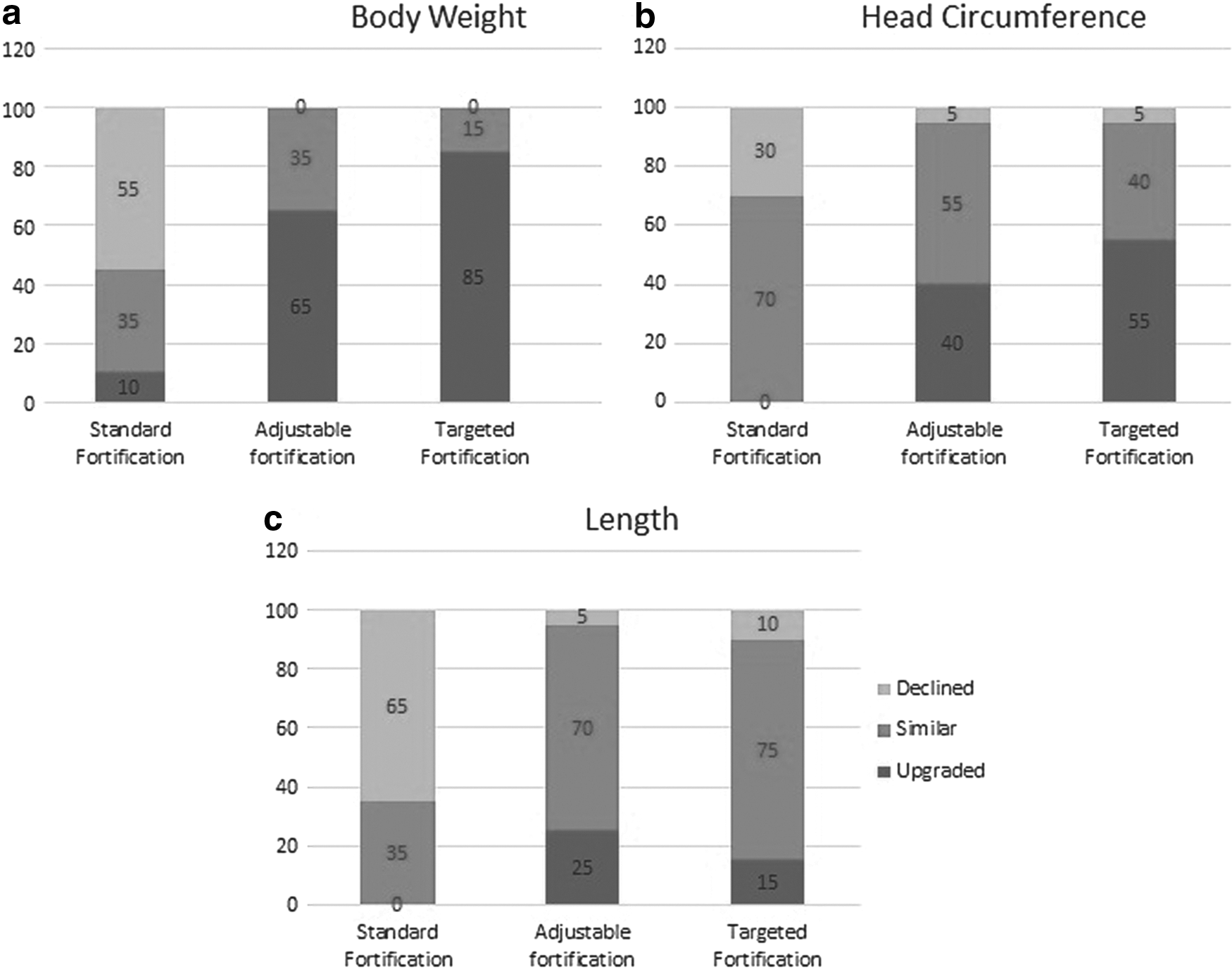
Changes in head circumference and length are also illustrated in Figure 1b and c.
During the study period, median daily protein intakes were 3.6 g/(kg·d) in SF, 4.3 g/(kg·d) in AF, and 4.5 g/(kg·d) in TF groups, and energy intakes were 128 kcal/(kg·d) in SF, 131 kcal/(kg·d) in AF, and 133 kcal/(kg·d) in TF groups. Daily protein and energy intakes in AF and TF groups were significantly higher than those in SF group (SF versus AF, p < 0.001 and SF versus TF, p < 0.001). There were no differences regarding protein and energy intake between AF and TF groups.
There was no statistically significant difference between AF and TF groups considering the effects on postnatal growth. There was no difference among groups regarding feeding intolerance and weekly blood tests.
Discussion
In this study, we showed that AF and TF strategies are more effective than SF strategy concerning improvement in growth parameters, including weight, length, and head circumference. To the best of our knowledge, this is the first study that compares AF and TF with SF in the same study population.
The optimal method for HM fortification remains to be determined, and various protocols are currently used in the NICUs. Although SF is the most commonly used method, it does not account for any variation of nutrient content in milk sample and may result in inadequate nutrient supply. 11 AF 9 necessitates BUN follow-up twice weekly and does not always completely reflect protein intake. Both SF and AF have a risk of feeding the baby with nutrient-deficient milk since their adjustments are based on outcomes. TF 12 is a promising method that corresponds better to the optimum requirements of VLBW infants, but requires extra equipment, which is not always available in the NICUs due to its high cost. Benefits of TF on the growth of preterm infants have been reported by many authors. In a retrospective study, the growth of 41 extremely low birth weight infants fed breast milk fortified with TF was assessed, and the mean weight increase was found as 16.04 ± 3 g/(kg·d). 13 Growth rate of the infants was higher than that of the fetus in the uterus [15 g/(kg·d)]. However, infants failed to remain in the same percentiles of birth and, at discharge, only 27.7% weighted >10 centiles in this study. Median daily weight gain of the infants in TF was about 25 g/(kg·d) in our study. The infants improved to 50 percentile and more after the fortification period. We have speculated that weight gain at rates of 20 g/(kg·d) and more might reflect better growth.
On the contrary, two previous studies showed similar outcomes with TF and SF. In the study by Rochow et al., 7 protein, fat, and carbohydrates were analyzed and individually added to routine fortification. Those infants who had TF grew similarly to the controls at a rate of about 20 g/(kg·d). It was speculated that this result might be due to higher milk intake of the routinely fortified group [155 ± 5 mL/(kg·d)] than the target fortified group [147 ± 5 mL/(kg·d)]. To avoid the effect of volume difference, infants in our study were fed with similar volumes of breast milk [160 mL/(kg·d)] during the study period in all of the fortification groups. Different from our study, fortification of breast milk was also performed by measuring and adjusting the nutrient levels on a daily basis by Rochow et al. 7 In the study of McLeod et al. 14 who compared the effect of TF with that of SF, they did not find any difference in growth rate between groups that was lower than both recommended growth rates and our results. We suggest that metabolic and biological responses to similar fortification regimens might be the reason for different growth outcomes in different populations.
Desired postnatal weight gain in VLBW infants is 15–20 g per day, and in our study we have achieved same daily weight gain ratio with AF and TF. Furthermore, we have demonstrated that weight, head circumference, and length percentile after 4 weeks of fortification period were improved by AF and TF when compared with those by SF. Daily protein and energy intakes in AF and TF groups were higher. After the supply of optimal energy and protein intake in preterm infants, we have achieved the postnatal weight gain >15–20 g per day in the preterm infants fed fortified HM with AF and TF methods.
In this study, we showed that TF of breast milk is feasible in daily clinical routine. The analyzer is a bedside device, and it is easy to use. Recently it was reported that daily analysis for TF increases workload by 10–15 minutes/(patient per day). Even twice per week measurements led to mean macronutrient intake within a range of ±5% of targeted levels. 15 Therefore, we have also performed the analysis of breast milk twice a week. Breast milk was fortified to achieve protein levels as recommended by ESPGHAN guidelines. All safety measurements during the intervention were within normal ranges, and plasma BUN levels suggested adequate protein intake.
The increase in head circumference, which is an indicator of better neurodevelopment outcomes, was more prominent in AF and TF groups than in the SF group in our study. However, Lucas et al. assessed developmental outcomes at 18 months of age and did not find any improvement in developmental scores with the use of a commercially available fortifier. 16 Further studies are needed to clarify the association between fortification and neurodevelopmental outcomes. Neurodevelopmental assessment of our cohort will explain the effect of different types of fortification.
In clinical practice, there are still concerns about feeding intolerance due to the use of formula-derived HMF. The Cochrane review, 17 from the small number of infants for whom this outcome was reported, showed a nonsignificant trend toward an increased risk of feeding intolerance in treated infants (Relative risk 2.85, 95% confidence interval 0.62–13.1). As we did not have a nonfortified group in this study, we have not seen any feeding intolerance in groups. We were also unable to measure the osmolality of the enteral feeds. However, no cases of necrotizing enterocolitis were observed in our study after randomization. It was also reported that fortification of HM with multicomponent fortifiers induces a significant increase in osmolality, but the clinical consequences of this effect are not clearly defined. 18
There are some limitations to our study. First, we could not assess the effect of fortification methods throughout the entire hospital stay. Second, our physicians were not blind. To avoid this problem in the evaluation of growth rate, all measurements were performed by nurses who were blind to the study groups.
In conclusion, AF and TF of breast milk improve body weight, head circumference, and length percentiles in VLBW infants after 4 weeks of fortification period. Both AF and TF are practical, safe, and suitable for routine clinical use.
Different fortification strategies aim to optimize the macronutrient intake and growth of premature babies. The most applicable of all these fortification strategies is still unclear.
Adjustable fortification and targeted fortification of breast milk improve body weight, head circumference, and length percentiles in very low birth weight infants more than standard fortification.
Footnotes
Disclosure Statement
No competing financial interests exist.