
Abstract
Abstract
Background:
Scaling-up human milk banks (HMBs) is a promising solution for saving vulnerable newborns. Exploring perceptions and practices on donor human milk (DHM) and HMBs is essential to strengthen and scale-up an integrated HMB system resting on a model called the “Mother Baby Friendly Initiative Plus” (MBFI+), which includes promoting breastfeeding, encouraging kangaroo mother care, and providing safe DHM to vulnerable babies without access to mother's own milk.
Materials and Methods:
A qualitative research was conducted among 56 service recipients including mothers and key influencers and 9 service providers to understand their perceptions and practices on DHM and HMBs.
Results:
Service providers opined that DHM is safe and lifesaving for vulnerable babies. Challenges shared were limited supply of DHM because of low awareness on milk donation, shortage of trained staff, and risk of milk contamination. They stated that although most mothers were comfortable in donating milk, few were reluctant to donate milk as they feared shortage of milk for their own babies, or milk expression may cause weakness. Recipient mothers accepted use of DHM as per facility norms but had concerns about donor mothers' health and hygiene and measures for ensuring milk safety. Most grandmothers were resistant toward donating or receiving DHM for their grandchildren. Many fathers were comfortable with donating once they knew it is lifesaving and did not compromise supply for their babies. Service providers shared opportunities for scale-up, like improving awareness and infrastructure, lactation counseling by skilled personnel, supportive hospital environment, and establishing HMBs in every city and district.
Conclusions:
Human milk banking should be strengthened as part of the MBFI+ model. For this, behavior change communication targeted at mothers and influencers about breastfeeding and HMB from the antenatal period, capacity-building among service providers, and government ownership is necessary.
Introduction
D
Among a plethora of approaches, including resuscitation, prevention, detection and treatment of neonatal infections and kangaroo mother care (KMC), early, exclusive, and continued breastfeeding has the greatest potential impact on child survival and development. 3 At present, only 41% in India receive human milk in the first hour of life. 4 A non-breastfed child's risk of death is six times more than that of a breastfed child born in resource-limited settings. 5 Improving breastfeeding practices can prevent 160,000 under-5 deaths in India each year, 87% of whom are <6 months of age. 3
Many vulnerable newborns, who are at greatest risk of negative health outcomes in the absence of human milk, lack access to mother's milk for reasons, including mother's illness or death, baby's illness or inability to suckle or delay in milk production.
The World Health Organization (WHO) recommends the use of donor human milk (DHM) from a human milk bank (HMB), as the next best option as it ensures exclusive human milk feeding until mother's own milk is available. 6 HMBs collect, pasteurize, test, and store safe DHM from lactating mothers and provide it to neonates and infants in need. The advantages of feeding DHM to vulnerable infants as compared with formula milk include reduced risk of sepsis and necrotizing enterocolitis, greater feeding tolerance, fewer days of stay in neonatal intensive care unit (NICU), and substantial cost savings.7–23
Asia's first HMB was established in Mumbai, India in 1989 and was the only HMB in the country till 2005. During 2005 to 2015, 22 HMBs were added. This number has more than doubled in the past 2–3 years. There are >50 HMBs in the country at present, grossly inadequate to meet the massive demand of DHM. Expanding HMBs has been challenging because of lack of systems to effectively integrate it within newborn and breastfeeding programs, lack of standard operating procedures, limited collaboration between obstetricians and pediatricians, shortage of lactation counselors, and low awareness among service providers. 24 The “National Guidelines on Lactation Management Centers in Public Health Facilities” was launched in 2017 by the Government of India and has set a target to make breast milk available to all babies. 25 HMBs shall be strengthened as part of lactation support centers to encourage breastfeeding, provide safe DHM to sick and vulnerable newborns without access to mother's own milk, and support KMC as an integrated newborn care approach. 25 The model is called Comprehensive Lactation Management Centre (CLMC) and was adapted from PATH's Mother Baby Friendly Initiative Plus (MBFI+) model (Fig. 1).26,27
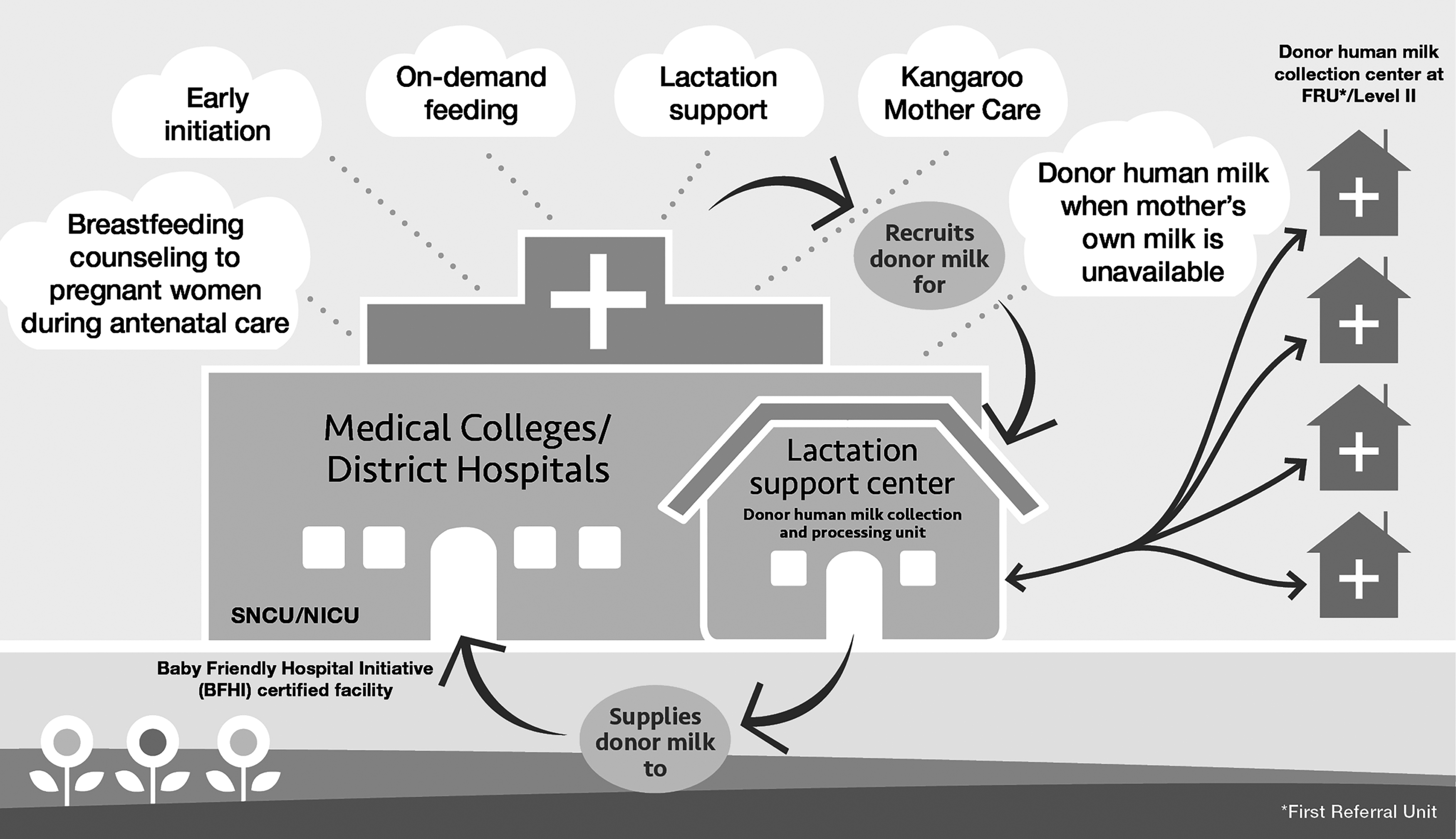
Mother Baby Friendly Initiative Plus model adapted for India. NICU, neonatal intensive care unit; SNCU, sick newborn care units.
In India CLMC is the term assigned for globally known term HMB. Although the effectiveness of the MBFI+ model has been proven in a variety of contexts, there is a need for country-specific insights to create robust evidence base for national-level scale-up. Therefore, a formative research was undertaken to understand the perceptions and practices, on all three components of the model—breastfeeding, KMC, and DHM among service providers and service recipients (mothers, fathers, and grandmothers).
This article illustrates the results of a part of this research that focused on understanding the perceptions and acceptability of DHM and HMB among service providers, individual mothers availing services and influencers (fathers and grandmothers) in two health facilities in Mumbai, one with and one without a HMB. There is lack of such studies in the Indian context. This adds important and interesting dimensions to this area.
Materials and Methods
Two health facilities under the Mumbai Municipal Corporation were purposively selected as case studies; a Level III facility with a HMB and a Level II facility without an HMB. The study obtained clearance from the Institutional Ethical Committee of respective health facilities. Qualitative research methods were used to collect data. In-depth interviews were conducted with nine service providers including HMB in-charge, manager, technician, NICU in-charge, staff nurses, and lactation counselors. Seven focus group discussions were conducted with 56 service recipients (Table 1). These were audio recorded after taking informed consent from the participants. Service providers at the facilities who had been providing new born care services for at least 6 months and were aware of HMB policies and functioning were selected. The inclusion criteria of the service recipients are given in Table 2.
DHM, donor human milk; FGD, focus group discussion; HMB, human milk bank; NICU, neonatal intensive care unit.
DHM, donor human milk; HMB, human milk bank; NICU, neonatal intensive care unit; PU, preterm unit.
Cultural and religious contexts were given due sensitivity while framing the focus group discussion (FGD) guides. All the tools were piloted and modified before data collection. FGDs were conducted in local languages (Hindi and Marathi) by a trained facilitator who was assisted by two researchers. All audio records were transcribed in local languages (Hindi and Marathi) and then translated into English. Transcribed data quality was cross-checked with audio recordings to ensure completeness, accuracy, and quality of the transcription. Data were analyzed separately for each category of participants (service providers, mothers, and influencers) and then reanalyzed to assess similarities and differences in perceptions across respondent groups. Triangulation was performed at two levels—across methods and across respondents. The steps to analyze data included open coding (free listing or fracturing of responses, domain formation, coding, and organizing the data), axial coding (relationship or connection between categories and subcategories), selective coding (identifying core themes to which several other categories and subcategories were related), and reduction (getting the big picture).
Results
The results elaborate the perceptions and practices about DHM and HMB among service providers and recipients.
Data pertaining to service providers
Perceptions about human milk banking
All respondents at the Level III facility opined that the HMB has enabled access to lifesaving human milk for every neonate in the hospital and reduced the need for top feeds (Table 3). This has protected babies from infections and provided them with nutritional benefits.
DHM, donor human milk; HMB, human milk bank; NICU, neonatal intensive care unit; PDHM, pasteurized DHM; PU, preterm unit.
Milk from the HMB was perceived to be safe because it is tested for presence of microbes. The pediatrician and the senior resident of Level III NICU felt that there was not much resistance among mothers to donate milk.
Banking practices
Although there is a set criterion in the hospital for feeding babies, DHM was mostly given to preterm (∼70%) and LBW babies admitted in the NICU, followed by babies separated from their mothers because of maternal illness, and a small proportion of full-term babies whose mothers had limited milk. Babies of mothers who were unable to breastfeed because of caesarean section, whose initial milk output was low, or who had died were also DHM recipients. There were varied responses with respect to informing parents about feeding DHM to their babies. Some said that the parents are not informed that DHM was being given. However, a senior resident stated that while parents of babies admitted in the NICU were informed about the feed being given to their babies, consent was not taken from parents of babies in transitional care unit and preterm unit (PU). The service providers reported challenges, such as difficulty in maintaining adequate supply of DHM to meet the high demand and discarding DHM because of microbiological contamination leading to further shortage. Shortage of human resources was also responsible for less collection of milk. Nearly 50% to 60% of milk was collected in the outpatient department's well-baby clinic and the rest from mothers in postnatal care (PNC) ward and mothers of babies admitted in the NICU.
Laboratory technicians attributed microbial contamination of the donated milk to lack of precautions while expressing milk, improper cleaning and drying of milk containers and pasteurization machine, through ice used for cooling milk, or while transporting expressed milk from the wards to the HMB. On an average, 3% post-pasteurization samples were discarded every month. HMB equipment repairs are carried out on an “as is-where is” basis without annual maintenance contracts as no funds are allocated for recurring expenses.
Perceived barriers among mothers and influencers for donating milk
The senior resident and the lactation counselor mentioned that some mothers were reluctant to donate milk because of the fear of shortage for their own babies, or apprehension that milk expression may cause weakness. There were few instances of refusal to donate because of religious reasons. One lactation counselor mentioned that less educated family members are more likely to refuse donation.
Mothers whose babies were fed DHM were concerned about nonavailability of milk for their babies after discharge. A lactation counselor opined that families often assume that babies would continue to get milk from the HMB after discharge. Fathers of babies admitted to the NICU had positive opinions about HMB, whereas those whose babies had never received DHM opposed the concept as they were uncomfortable with the new phenomenon.
Sustaining an adequate supply of DHM
The team at the Level III facility adopted several approaches to motivate and counsel mothers to breastfeed their own babies and donate excess milk. The pediatrician reported that counseling was done during the ward rounds and no dedicated time was allocated for counseling. The lactation nurse said that counseling was done in the PNC wards for mothers facing lactation challenges. Mothers were counseled before and while expressing milk to donate excess milk to the bank. According to the senior resident, the best time for counseling for donation was just before discharge as mothers whose babies were fed DHM were aware about HMB and milk donation. Mothers should preferably not be counseled early (during first 2 days after delivery) about donation as they required some time to feel comfortable.
The staff agreed that mothers attending the well-baby clinics must be motivated to donate milk and mothers in PNC wards and NICU area should be counseled to express milk to sustain and improve milk collection for the HMB. The prevailing practice was that the mothers expressed milk only when required and in small quantities for feeding their own babies.
Most providers suggested that more information, education, communication (IEC) materials such as posters, videos/films, and pamphlets on HMB can be displayed in the hospital premises. Other suggestions included engaging more lactation counselors to support mothers to breastfeed and express milk, encouraging use of breast milk pumps for mothers with breast engorgement and creating supportive and stress-free environment in the hospital for mothers. It was opined that impolite behavior of the staff increases stress among mothers, thus reducing oxytocin levels, which leads to low milk production.
Majority of the staff agreed about the lack of awareness about HMB among parents of babies admitted to the NICU. The dean and pediatrician in-charge suggested strengthening the infrastructure and reducing overcrowding, particularly in the NICU. There was a suggestion that IEC materials should also be displayed in the community to improve awareness about HMB. There was a unanimous demand that the government should take up the issue of scaling-up HMB as high priority and mandate the establishment of HMB in every metropolitan city, state, and district.
Data pertaining to service recipients
Perception regarding DHM
All recipient mothers were aware of their babies receiving banked milk from another mother and recognized it to be supplied in “steel ka dabba” (steel containers).
Recipient mothers had concerns about the health and hygiene of donor mothers (Table 4). They were not aware of the sterilization measures followed in HMBs and had concerns about the safety of the DHM fed to their babies. However, once their concerns were addressed, they understood the benefits of DHM and accepted it. Some mothers reported feeling guilty for their inability to breastfeed their babies themselves.
DHM, donor human milk; HMB, human milk bank; NICU, neonatal intensive care unit.
Most donor mothers were comfortable to donate milk to the bank. Although many were not familiar with the term “human milk bank,” they were aware that their donated milk is given to babies in need of mother's milk.
Donor mothers were unanimous that donating milk did not affect their own babies in any way because only the excess milk was donated. Some potential donors and recipients did not have full information and had concerns about donating and receiving milk.
Perception of influencers
Many fathers were comfortable with their wives donating milk but only after their own babies were sufficiently fed. Like mothers, most had similar concerns about the safety of milk. However, they became comfortable with receiving DHM for their babies once they learnt about the processes followed at the HMB to make the milk safe. Very few were aware that their babies were receiving milk from the HMB. Most grandmothers were uncomfortable with allowing their daughters or daughters-in-law to donate milk; they were worried that it might reduce supply for the newborns.
They were also uncomfortable about receiving DHM for their newborns and felt that the milk from other women might not be safe for the baby. There was no awareness about HMB among grandmothers. Only one grandmother said she knew about human milk banking as she had seen something about it on television at the Level III NICU, but was not aware of the processes. One grandmother felt that there would be lifelong obligation if milk was taken from someone else. All the respondents confirmed that they had not seen any IEC material on HMBs in the hospitals.
Discussion
As the government plans the scale-up of HMBs as part of CLMC model in all tertiary hospitals and high performing sick newborn care units with high delivery load, the case studies of these two institutions will contribute toward strategizing ways to ensure acceptance and utilization of HMB services. Understanding perceptions of mothers, influencers, and service providers are crucial in optimizing the supply and demand chain of HMBs. Very few studies exist in this area and hence this study assumes critical importance in the Indian context.
In this study, the service providers agreed about the critical role of HMB in improving access to exclusive human milk feeding for vulnerable neonates and infants. Although the providers and the recipients expressed positive opinions about expanding human milk banking as a lifesaving intervention for vulnerable babies, few challenges and opportunities remain. Our study emphasized the need to strengthen quality and processes of HMB including taking informed consent from donors and recipient families and following respectful patient care, especially in light of the finding that very few fathers were aware that their babies were receiving milk from HMB. Challenges such as limited supply of DHM because of low awareness on milk donation, shortage of trained staff, and risk of milk contamination need to be addressed by ensuring adequate safety measures and educating recipients about HMBs and its processes are necessary. The findings are similar to the study conducted in Hong Kong that flagged the importance of a strict monitoring system to address safety concerns on milk donation and banking. 28
In this study service providers stated the inability of the mothers (whose babies were in the NICU) to breastfeed after discharge. The mothers of babies who were admitted in the NICU express milk only when required and in small quantities for their own babies. The study also highlighted that in case of cesarean deliveries, breastfeeding is delayed because of the practice of separating the mother and baby. These findings bring forth the need for skill-based counseling of mothers starting as early as antenatal care (ANC) period, support at the time of birth and teaching milk expression early on so as to increase their milk output and sustain breast milk supply for the babies after discharge. Having adequate number of lactation counselors, strengthening lactation support and counseling by the service providers, especially nursing staff, will improve breastfeeding and milk expression for sufficient feeding of own babies and donation. The practices of unnecessary separation of mother and child need to be looked at by hospital administration and corrective actions taken. Leung and Yau emphasized on the quality of lactation care for the mother–infant dyad especially when the infants are ill; careful monitoring of the lactation experience and the commitment of service providers to guide the family through the process contribute to positive outcomes. 28 A supportive hospital environment will further help in reducing stress and building confidence among mothers. In another study it was highlighted that mothers need and want professional advice on lactation for term and preterm infants, for making the best choices for themselves and their infants. 29 Spatz et al. also pointed out that knowledge of nurses needs to be updated with the latest research. 30
Our study brings to light few apprehensions and concerns among mothers related to milk donation. The attitude of mothers toward donation was generally shaped by the concurrence from their husbands and mothers-in-law who had minimal information about benefits of breast milk donation. Shortage of trained and skilled staff meant that adequate time was not allocated for informing and motivating mothers and other family members for milk donation. Counseling during ANC regarding the potential to donate excess milk postpartum can be worthwhile to improve awareness among new mothers. Specific concerns and misconceptions of mother and families on milk donation like shortage of milk for their own babies, perceived weakness after donation, quality and safety of donated milk, decrease in milk supply after donation should be addressed during counseling sessions through personalized approaches and greater involvement of family members during counseling. Generating awareness among these key influencers regarding DHM and HMB practices will help overcome the obstacles that hinder acceptability of DHM and subsequent donation. Perceptions among family members of particular religious community that breast milk donation causes life-long obligation, should also be addressed during counseling.
Motivating mothers in postnatal phase to donate milk, identifying existing donors from the community and creating mother support groups where mothers link potential donors to the HMB and, improving infrastructure and reducing overcrowding, particularly in the NICU will be helpful in encouraging donation. Our study found the need for having IEC materials both in the hospital and in the community to increase awareness about HMB and motivate mothers to breastfeed and donate milk. Dissemination of information on milk donation in the community will help not only to fulfill the milk requirement of babies in the government hospital but also for babies who are delivered at home or private facilities. A study in South Australia made similar suggestions that benefits and processes of HMBs should be well publicized to increase public awareness and acceptance from mothers and families. 31 In a study carried out in Brazil, it was reported that although mothers had difficulties in donating, a rewarding feeling, acknowledging the value of this practice, and the support received from people were important factors in increasing their readiness to donate. 32 Another study conducted in Mumbai reported that donation rates were higher in more educated women and promoting education will aid in improving awareness about importance of milk donation. 33 A study carried out in South Africa also concluded that education level of mothers can play an important role in supporting HMBs by improving mothers' perceptions and acceptance of breastfeeding, DHM, and milk banking. 34
There was an emphasis on the need for expansion of HMBs across India. The Brazilian model could be an apt example in this regard, which has established collection centers in maternity homes and secondary hospitals. The model prides of the largest network of HMBs and collection centers in the world and has successfully demonstrated the effectiveness of a government supported, nationalized, integrated HMB program that includes breastfeeding promotion, lactation support, and provision of donor milk, all of which contributed to achieving single-digit neonatal and infant mortality rate. 26
Conclusion
Hospitals providing newborn care can improve access to human milk by increasing investments in HMBs as part of integrated, newborn care and nutrition programs. With launch of the “National Guidelines on Lactation Management Centers in Public Health Facilities,” the national government is committed to improve newborn and child health and reduce mortality by providing the best nutrition available to all infants. However, for effective scale-up, it will be important to ensure improved government ownership, mandate availability of standard operating procedures at all facilities, provide a supportive hospital environment for lactation and donation, adhere to and monitor implementation of baby-friendly hospital initiative policies and practices in facilities and hire more lactation counselors. Improved awareness through interactive IEC materials in hospitals and communities, skill-based counseling from the ANC period with messages addressing concerns on HMB and DHM and building trust among mothers and influencers in the institution of HMB is essential. To address the supply–demand gap, HMBs need to be established at tertiary-level facilities with collection centers at secondary-level facilities. Strengthening human milk banking as part of the MBFI+/CLMC model that focuses on aligning human milk banking with breastfeeding promotion and KMC and integrating them into the mother and child health programs will be a step toward achieving the Sustainable Development Goals to end preventable newborn and under-5 deaths.
Footnotes
Acknowledgments
This study is the result of the contribution of many people particularly the participants who invested their valuable time to discuss the issues of human milk banking in the health facility and their homes with the study team. The formative study is a result of the joint efforts of Lokmanya Tilak Municipal Medical College and General Hospital (LTMMC) and PATH. While LTMMC led the efforts on implementation of the research, PATH played a key role in providing technical expertise. PATH conceptualized the research design and the protocol, LTMMC provided the inputs, and both teams finalized the report and the manuscript. Our special gratitude and acknowledgment is extended to Sudip Mahapatra, Regional Monitoring and Evaluation Specialist, PATH, for reviewing the research design and report. Our sincere thanks to Manu Bhatia for providing editorial assistance. We also acknowledge the human milk banks in India that are committed to increasing access to human milk to all infants by promoting breastfeeding and providing safe donor human milk and saving lives. This project was funded through a grant from the Margaret A. Cargill Foundation to PATH.
Declarations
The study has been approved by Lokmanya Tilak Municipal Medical College & Lokmanya Tilak Municipal General Hospital, Staff and Research Society (Reference number—IEC/60/16), and the consent was obtained from all participants.
Disclosure Statement
No competing financial interests exist.