
Abstract
Abstract
Introduction:
Hypertension is relatively common in pregnancy, and pregnancy may unmask hypertension among women who are predisposed to it. Lactation may be a means through which to mitigate pregnancy-related vascular risk. The impact of lactation on maternal blood pressure, and the duration of any effect, remains unclear. This study aimed at systematically reviewing the literature evaluating the impact of lactation on the development of hypertension.
Materials and Methods:
We searched PubMed, including EMBASE and MEDLINE, for studies that reported on the association between breastfeeding and maternal risk of hypertension that were published in a peer-reviewed source. The quality of the studies included was assessed by using the Newcastle-Ottawa Scale.
Results:
Nineteen studies met all inclusion criteria for this review. Of the four studies with short-term follow-up, 50% showed a protective association. The fifteen studies with longer-term follow-up were stratified by outcome assessed. Sixty-seven percent of the studies that evaluated for elevated blood pressure and 100% of the studies evaluating for an outcome of hypertension showed a protective association. The minimum duration of lactation associated with a benefit was 1 month. This association was demonstrated in follow-up periods as long as two to three decades. Studies that showed a protective association had overall higher quality ratings.
Discussion:
Lactation is associated with a beneficial effect on maternal blood pressure that persists for decades. These results add to the growing body of literature demonstrating the protective association of lactation on maternal cardiovascular risk. Providers may incorporate the decreased risk of hypertension into their counseling on the maternal benefits of lactation.
Introduction
H
Though some studies have shown that lactation decreases risk of maternal hypertension, data have not been conclusive. We systematically reviewed the literature on the impact of lactation on hypertension in parous women. We aimed at reviewing and summarizing this literature, including an assessment of both the duration of lactation required to avoid subsequent risk of hypertension and the duration of this protective effect after cessation of lactation.
Materials and Methods
Search strategy and study selection
Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 18 we searched PubMed, which includes MEDLINE (1946–present) and EMBASE.com (1974–present), to identify studies assessing the relationship between lactation and maternal hypertension at any point in the postpartum period. Search strategies were developed by a health sciences librarian (C.W.). Using each database platform's command language and search fields, various combinations of the following Medical Subject Headline and keyword groupings were investigated: breastfeeding, lactation, blood pressure, hypertension, and metabolic syndrome. Searches were finalized in August 2015.
Two reviewers (E.B. and H.J.) independently evaluated all records for eligibility by using DistillerSR, a web-based systematic review data management system. Any discrepancies regarding inclusions were resolved by review from the senior author (J.C.) and by group consensus.
Study eligibility criteria
We included original, published peer-reviewed studies that met the following inclusion criteria: (1) human participants with any prior lactation; (2) ≥1 full term birth; (3) investigated association between breastfeeding and maternal risk of hypertension at any future time point, outside of subsequent pregnancies; and (4) included a parous comparison group with no lactation, or a shorter duration of lactation. To achieve a comprehensive review, it was not possible to limit inclusion to a more homogeneous comparison group given the nature of the lactation literature. As in prior studies, the terms “lactation” and “breastfeeding” were used interchangeably. Cross-sectional, prospective cohort, case–control, nested case–control, and randomized controlled trials were included. Full inclusion and exclusion criteria are described in our protocol registered on PROSPERO and can be accessed at: www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42015025933.
Data abstraction
Data were abstracted and independently confirmed by using a custom study database using the REDCap platform, 19 a secure web-based data collection and management application hosted by the University of Pittsburgh. Study abstraction forms consisted of fields including: sample size, study type (e.g., cohort, cross-sectional, case–control, etc.), follow-up period, exposure definition (e.g., breastfeeding reported as total lifetime duration, or breastfeeding months per child, etc.), duration of breastfeeding, description of comparison groups, exclusivity of breastfeeding, results based on recall versus clinical documentation, whether the study's primary outcome was hypertension or blood pressure, lack of preexisting hypertension at baseline, adjustments, and associations calculated.
Assessment of risk of bias
Two authors (E.B. and H.J.) independently performed quality assessment by using the Newcastle-Ottawa Scale (NOS). This tool was developed for use in systematic reviews, to assess the quality of non-randomized studies, such as case–control and cohort studies. 20 Scores were reported as total values between 0 and 9. Disagreements in quality were adjudicated by the senior author (J.C.) and with group discussion to reach consensus.
Data synthesis
The results were stratified by duration of follow-up, as well as by the outcome evaluated. Those studies that followed participants for <6 months were categorized as short-duration follow-up, and those studies that included follow-up for >6 months were included in the longer-term follow-up group. The longer-term follow-up group was further stratified by outcome, grouping together those studies that evaluated blood pressure values versus those that evaluated for a diagnosis of hypertension. Meta-analysis was not performed given the heterogeneity of both methods and outcome measures used in the studies included in our systematic review.
Results
Study selection
We retrieved a total of 5,342 citations in PubMed and EMBASE in August 2015. After screening for duplicate records, 4,817 citations remained. A total of 4,771 records were excluded based on title and abstract screening. Forty-six articles underwent full text review, and 19 studies met all inclusion criteria. Reasons for exclusion for the remainder of the articles, as well as the number of articles excluded for each reason, are delineated in the PRISMA flow diagram (Fig. 1).
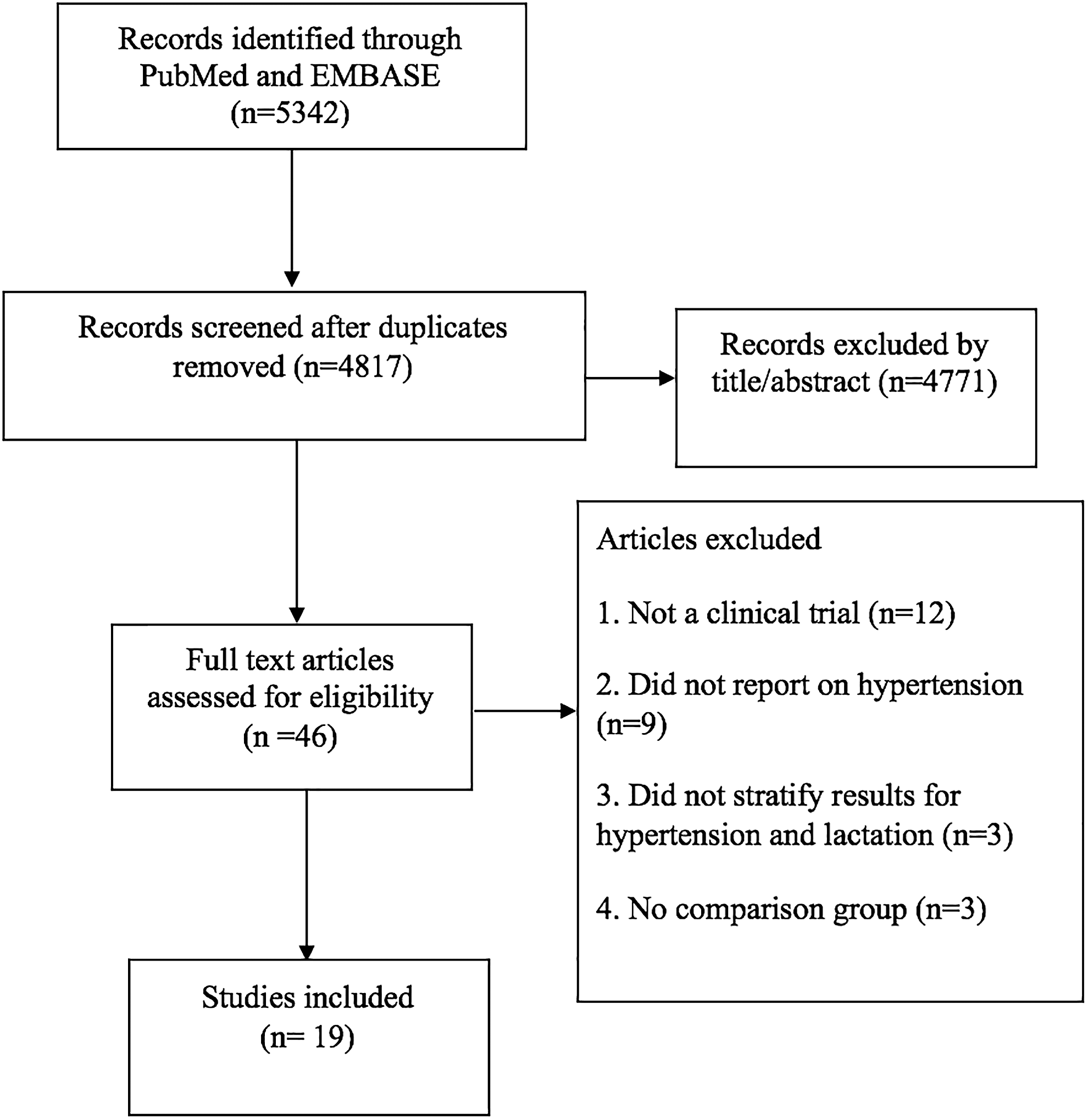
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of studies identified in systematic review.
Study characteristics
Of the 19 studies that met all inclusion criteria, 10 were prospective cohort studies, 4 were retrospective cohort studies, 4 were case–control studies, and 1 study was cross-sectional. The studies were geographically diverse, including studies from China, Japan, South Korea, Australia, Norway, Republic of Belarus, Iran, and Finland; seven of the studies included U.S. populations. Regarding baseline characteristics, nine studies documented that participants were normotensive at baseline. Twelve of the 19 evaluated for potential confounders for the data relating to hypertension and blood pressure, although confounders assessed varied across studies. These included tobacco use, body mass index (BMI), family history of hypertension, parity of participants, physical activity, diet, age, education, race, presence of pregnancy complications, use of oral contraceptives, and marital status (Table 1).
BMI, body mass index; HTN, hypertension; OCP, oral contraceptive pill; SD, standard deviation.
Synthesis of results
Of the 19 studies included in this systematic review, 14 showed a protective effect of lactation on the development of maternal elevated blood pressure. The majority (14/19) of the studies did not describe the intensity of lactation (i.e., whether infants were exclusively breastfed).
There were four studies that followed participants for <6 months, with total follow-up ranging from 4 days to 5 months. Two out of four (50%) of these short-duration follow-up studies showed a protective effect of breastfeeding (Table 2).
CI, confidence interval; DBP, diastolic blood pressure; HR, hazard ratio; N/A, not applicable; NOS, Newcastle-Ottawa Scale; NS, nonsignificant; OR, odds ratio; SBP, systolic blood pressure.
Among studies with longer-term follow-up that evaluated blood pressure as an outcome, six out of nine (67%) studies showed a protective effect of lactation (Table 3). The duration of follow-up ranged from 3 to 35 years. In those studies with longer-term follow-up that evaluated the relationship between history of lactation and a future diagnosis of hypertension, six out of six (100%) showed a protective effect (Table 4).
No significant difference in women without gestational diabetes.
LDB, long duration breastfeeding; MDB, medium duration breastfeeding; RR, relative risk; SDB, short duration breastfeeding.
No significant difference in women without gestational diabetes, 12–18 months, 18–24 months, >24 months. Lifetime breastfeeding duration ≥6 months associated with lower odds of HTN women aged 45–64 years versus parous women who did not breastfeed.
No significant difference in women >50 years of age.
Risk of bias of included studies
The overall mean NOS score of all of the studies in our review was 6. Those studies that showed a protective effect had a higher average NOS score, with an average of 6.5 compared with 4.8 in those that did not show a protective effect of lactation on maternal risk of hypertension.
Discussion
Our results demonstrate that most studies examining the impact of lactation on maternal hypertension show a protective association, including among mothers who had durations of lactation ranging from only 1 to 4 months.
Among studies that had <6 months of follow-up, the two studies without findings of a protective association between breastfeeding and blood pressure21,22 followed women for only 4 and 14 days postpartum, compared with 1 and 5 months for the studies that did show a benefit.23,24 These results suggest that the physiologic mechanisms by which lactation affects maternal risk of hypertension develop over the first weeks to months postpartum. With short durations of follow-up, women who lactated had significantly lower blood pressure than those who did not, though the magnitude of this difference was small. The protective association at 1 month of lactation has also been demonstrated in studies evaluating the positive association of lactation on the development of diabetes, suggesting that although not immediate (i.e., <2 weeks), the maternal benefits develop quickly. 12 Notably, the two studies that did not show a protective association also had lower quality scores, and also did not comment on exclusivity of breastfeeding, when compared with the ones that did show a protective effect, suggesting that there may also be methodologic differences that could impact the results.
When compared with the short-term follow-up studies, those that included longer durations of follow-up were more likely to show a protective association with lactation.9,12,17,25–33 Though follow-up times in most studies were quite variable, benefits were seen in studies that included participants up to 58 years of age at the time of enrollment. Similar findings have also been shown in studies of the long-term effect of breastfeeding on other markers of cardiovascular health, including visceral adiposity and diabetes.11,13,14 The results of this systematic review offer further evidence that the impact of lactation on maternal health, including future hypertension risk, persists decades after lactation is complete. This duration suggests that the impact may, indeed, be lifelong, although to date no studies have been of sufficient follow-up to answer this question. Overall, women should be counseled that being able to sustain lactation for the first weeks to months after delivery is associated with reduced blood pressure in later life, and this association appears to persist for decades.
Lactation appears to favorably alter maternal physiology in a multifactorial, and potentially permanent, manner, though the exact mechanism through which this protection is conferred is unclear. Further, the protective association demonstrated in the literature across multiple distinct diseases (e.g., hypertension, diabetes) suggests the potential for a common underlying physiology. Among the several physiologic mechanisms that have been proposed is the reset hypothesis, which suggests that lactation's protection from the development of cardiovascular disease is mediated by fat stores. According to this hypothesis, fat is accumulated during pregnancy both to support the pregnancy and in preparation for lactation, which remains if lactation does not occur,34–36 or is “reset” if lactation does occur. This has been supported not only in murine models 37 but also by the increased basal metabolic rate 38 in lactating women when compared with non-lactating parous women. It is likely that lactation's positive impact on blood pressure is due to factors beyond weight loss, as this benefit persisted in many studies after controlling for BMI.24,26,29,30,32,33 A second proposed mechanism for decreased blood pressure and cardiovascular risk factors includes hormonal mediation, 39 which may be part of the mechanism through which lactating women have been shown to have lower blood pressure than non-lactating women after only 1 month. 23 Studies have shown lower stress reactivity in breastfeeding mothers when compared with bottle-feeding mothers, leading to decreased systolic and diastolic blood pressure when confronted with the stressor of preparing and giving a speech. 40 However, there are potential confounders in this association, as a recent study has suggested that increased levels of postpartum anxiety are associated with a mother being less likely to breastfeed. 41 Another intriguing finding is that premenopausal women with estrogen-therapy-induced elevated levels of oxytocin, which are also elevated during lactation, have decreased total vascular resistance and lower blood pressure versus women with lower oxytocin levels. 39
The many benefits of lactation on future maternal health underscore the importance of counseling women on the personal health effects of breastfeeding. Previous studies have indicated that counseling of women who are pregnant, recently postpartum, or planning pregnancy can impact both breastfeeding rates and duration of breastfeeding. Many women decide about their intention to breastfeed before or early in their pregnancy. Mothers who are advised that lactation has important effects on maternal health appear to have stronger intentions to breastfeed. 42 Pre-conception and early pregnancy offers a unique opportunity for counseling, given the frequent encounters with healthcare providers for otherwise healthy patients who may not otherwise see physicians often. A large systematic review found that interventions to support breastfeeding have a beneficial effect on the number of women who continue to breastfeed at 6 months. 43 In a study about breastfeeding counseling and maternal actions, when postpartum women received positive advice, they were less likely to stop lactating than those who received mixed or negative advice. 44 In addition, a systematic review that evaluated the effectiveness of interventions aimed at increasing the number of women who initiate breastfeeding found that particularly in low-income women in the United States, breastfeeding education increased breastfeeding initiation rates. 45 However, many physicians are not aware of the potential benefits or do not feel adequately trained to provide counseling about the health benefits for future maternal health.46,47 This is an important barrier to overcome. It is clear that both primary care providers and obstetricians have an imperative to counsel women about breastfeeding not only on the beneficial effects for their infants but also for their own future health. This should ideally be done before pregnancy and reinforced throughout pregnancy and the postpartum period.
These results also have implications from a health policy perspective, as there are many societal barriers to initiation and duration of breastfeeding that in many cases will outweigh the impact of physician counseling and/or patient education about lactation benefits. 48 It is important to note that there are significant disparities in breastfeeding among U.S. populations. Breastfeeding rates for Black infants are 50% lower than those for Caucasian infants. 49 The reasons for this are not fully clear; however, the authors' proposed barriers include an earlier return to work, and less supportive working environments for Black women. 48 These facts are particularly relevant to our results, as the rates of hypertension are disproportionately higher in Black women when compared with Caucasian women (42.9% versus 27.7%) in a National Health and Nutrition Examination Survey conducted between 2007 and 2012. 50 Our results also underscore the need to support policies that facilitate breastfeeding among all U.S. populations.
A limitation of this literature is that the studies included have a wide variability of length of lactation exposure, exclusivity of lactation, and follow-up time. The heterogeneity of these methods and outcomes preclude the ability to perform a meta-analysis on their results. It is important to note that the NOS, which is the only validated method to assess quality of observational studies, 51 is not optimal to evaluate lactation literature. Specifically, many studies included in this review scored lower on the NOS because the lactation literature often assesses breastfeeding through self-report. However, this is believed to be both a valid and a reliable method of assessing lactation history, 52 and it is important to note that lower scores on the NOS in this review do not necessarily imply lower study quality. A strength of the retrospective study design is that it allows for a more long-term assessment of the health impact of lactation than would generally be feasible with prospective studies. However, it does largely preclude confirmation of lactation through other means such as chart review. Therefore, some methodologically strong studies may have lower NOS scores for this reason, so these quality scores should be interpreted with this limitation of the scores in mind. Another potential limitation to the interpretation of these data is that the reported results on the association between lactation and hypertension are subject to potential confounders. As the hypertension data may not have been a primary outcome in the study, the majority of studies did not adjust these data for known factors that may affect hypertension, including smoking status, race, and BMI.
Conclusions
Overall, the majority of studies that examined the relationship between lactation and maternal hypertension and/or blood pressure showed a positive association, including studies that examined short durations of lactation. These results further support the body of evidence that lactation alters maternal physiology in diverse and multisystem ways to confer cardiovascular benefit through mitigation of different disease processes. The beneficial association of breastfeeding on future maternal health should be incorporated into routine counseling for women before and throughout pregnancy, as well as during the postpartum period.
Footnotes
Disclosure Statement
No financial disclosures.