
Abstract
Abstract
Background:
Oral mesalamine (5-amino salicylic acid [5-ASA]) is an anti-inflammatory agent commonly used to treat inflammatory bowel disease such as ulcerative colitis and Crohn's disease. The transfer of mesalamine into human milk has to date been poorly described at the current dosages and newer formulations. This study was designed to determine transfer of mesalamine into human milk as a function of maternal dose and time, and dosage form.
Study Design:
Ten breastfeeding mothers (age 28–41 years) suffering from inflammatory bowel disease were recruited who provided milk samples at 0, 1, 2, 4, 8, 12, and 24 hours after a single daily dose of oral mesalamine in pH-dependent gastroresistant coated tablets (1.2, 2.4, 3.6, and 4.8 g). Milk samples were analyzed using liquid chromatography/tandem mass spectrometry.
Results:
A total of 10 women were enrolled for the study. The calibration curve for mesalamine was linear over a concentration range of 0.32–200 ng/mL. Irrespective of maternal dose, mesalamine levels in milk were exceedingly low. However, a wide range of mesalamine levels were observed among all the participants. The relative infant doses were all lower than 0.1% (range 0.003–0.085%).
Conclusion:
Regardless of dose and high variability, mesalamine levels in human milk were present in exceedingly low levels. The mothers in this study reported no side effects with their infants. These results suggest that the transfer of mesalamine into milk is very low and poses minimal risks to the breastfed infant.
Introduction
Mesalamine (5-amino salicylic acid [5-ASA]) is used in the treatment of inflammatory bowel diseases such as ulcerative colitis and Crohn's disease.1–3 Mesalamine relieves symptoms such as diarrhea, rectal bleeding, and abdominal pain. While the mechanism of action is not fully understood, mesalamine seems to act locally at the colonic mucosa to inhibit local prostaglandins and leukotriene synthesis in the gastrointestinal mucosa, 4 and therefore produce an anti-inflammatory effect. It is minimally absorbed orally (28–30%). 5 Other studies have suggested that it also acts as a free radical scavenger,6–8 thus suppressing toxicity of free oxygen species. In the presence of N-acetyltransferase I enzyme, 5-ASA is rapidly metabolized to its N-acetyl-5-ASA (N-Ac-5-ASA) derivative,9–11 all of which takes place in the intestinal wall and liver. It is considered to be inactive and is therefore therapeutically inert. 12 Mesalamine is recommended as an initial therapy in adult patients suffering from mild to moderate ulcerative colitis.
The U.S. Food and Drug Administration (FDA) approved the multimatrix formulation of mesalamine (Lialda®), which has a gastroresistant coating designed to dissolve at a pH of 7 in the colon. 13 Once exposed, the hydrophilic and lipophilic matrices in the tablet expand to form a viscous gel that spreads in a homogeneous manner throughout the colon. Another formulation Asacol HD® is comprised of an outer protective coat, which consists of a combination of acrylic-based resins, Eudragit S and Eudragit L (methacrylic acid). The inner coat, which consists of Eudragit S resin, is a pH-sensitive polymer that disintegrates at pH ≥7, thereby releasing mesalamine in the terminal ileum and beyond. 14 Two formulations studied are considered bioequivalent (AB rated). 15 The absorption of mesalamine, however, varies among individuals possibly as a function of the degree of severity of the disease. The release profiles of this drug are also variable across different pH levels and among the various commercially available formulations. 16 Although the use of mesalamine in breastfeeding mothers with inflammatory bowel disease is quite common, the safety of mesalamine in breastfeeding women has not been addressed, particularly in mothers taking the newer multimatrix formulations.
Rare but existing reports suggest the occurrence of diarrhea among breastfed infants exposed to the older mesalamine formulations. 17 The objective of this study was to analyze the newer multimatrix mesalamine formulations and their transfer of mesalamine into human milk at different dosages.
Materials and Methods
Sample collection
Milk samples were collected from 10 breastfeeding mothers (mean age = 32.2 years) at 0, 1, 2, 4, 8, 12, and 24 hours after administration of mesalamine. Eight of the 10 women were taking the formulation called Lialda (Shire Pharmaceuticals, Lexington, MA), and the remaining two consumed Asacol HD (Procter & Gamble Pharmaceuticals, Cincinnati, OH) and all but one took the drug once daily. They were all suffering from inflammatory bowel disease, and some of them have been on this drug for years. Milk samples were collected and frozen at −80°C until analysis was done. Each mother received a daily dose of mesalamine ranging from 1.2 to 4.8 g of mesalamine, and all were exclusively breastfeeding. Mothers who supplemented their infants with formula or were pregnant were excluded from the study. Demographic data of volunteer participants are described in Table 1. IRB approval was obtained for this study (IRB No. A12-3721) in Texas Tech University, and written consent was obtained.
Demographic Data of Mothers and Infants Who Participated in the Study
Age in days at the time of milk sampling.
Mesalamine and internal standard (Rotenone) were quantified by ultraperformance liquid chromatography tandem mass spectrometer. The assay used a Kinetex Biphenyl column (100 × 4.6 mm, 5 μm) from Phenomenex with a mobile phase of 16% (vol/vol) water and 84% acetonitrile with a flow rate of 0.6 mL/minute. To enhance recovery and increase sensitivity, the pH was increased to 11 by addition of a strong base. The m/z transitions used were from 154.2 to 108.3 for mesalamine and 395.1 to 213.2 for internal standard. Blank milk samples obtained from normal breastfeeding women who were not undergoing any drug therapy were used for the calibration curve. The milk concentration time datasets were subjected to pharmacokinetic analysis, using log-linear trapezoidal method to calculate area under the curve (AUC) for 0–24 hours and average concentration (Cavg); peak concentration Tmax and relative infant dose (RID). The data were calculated for each individual, as there was significant variation observed among these individuals.
Results
We developed a simple and efficient method with the aim to optimize the chromatographic and mass spectrometric conditions. Calibration curves were obtained by analyzing the standards prepared by spiking the blank milk according to the above procedure. The linear concentration range determined for mesalamine was from 0.32 to 200 ng/mL. The resulting data were analyzed by linear regression, and a correlation coefficient of 0.99 was obtained. The method was successfully applied to investigate the levels of mesalamine in human milk.
Mean age of participants was 32.2 years (range 28–41 years). The mean infant age at the time of the study was 92.5 days (range 35–251 days) as represented in Table 1. All maternal subjects were at steady state when samples were collected, they had been taking the drug for many years. As shown in Figures 1 and 2, the milk levels of mesalamine exhibited considerable interindividual variability. For instance, the AUC for mothers receiving the same 4.8 g dose ranged from 396 to as high as 12,295 ng/hour/mL. Even milk levels at lower doses were highly variable. Despite the variability, the absolute RIDs were still quite low ranging from 0.003% in subject 5 to 0.085% in subject 10. These results suggest that mesalamine is poorly transferred into the milk compartment. The pharmacokinetic measures are summarized in Table 2.
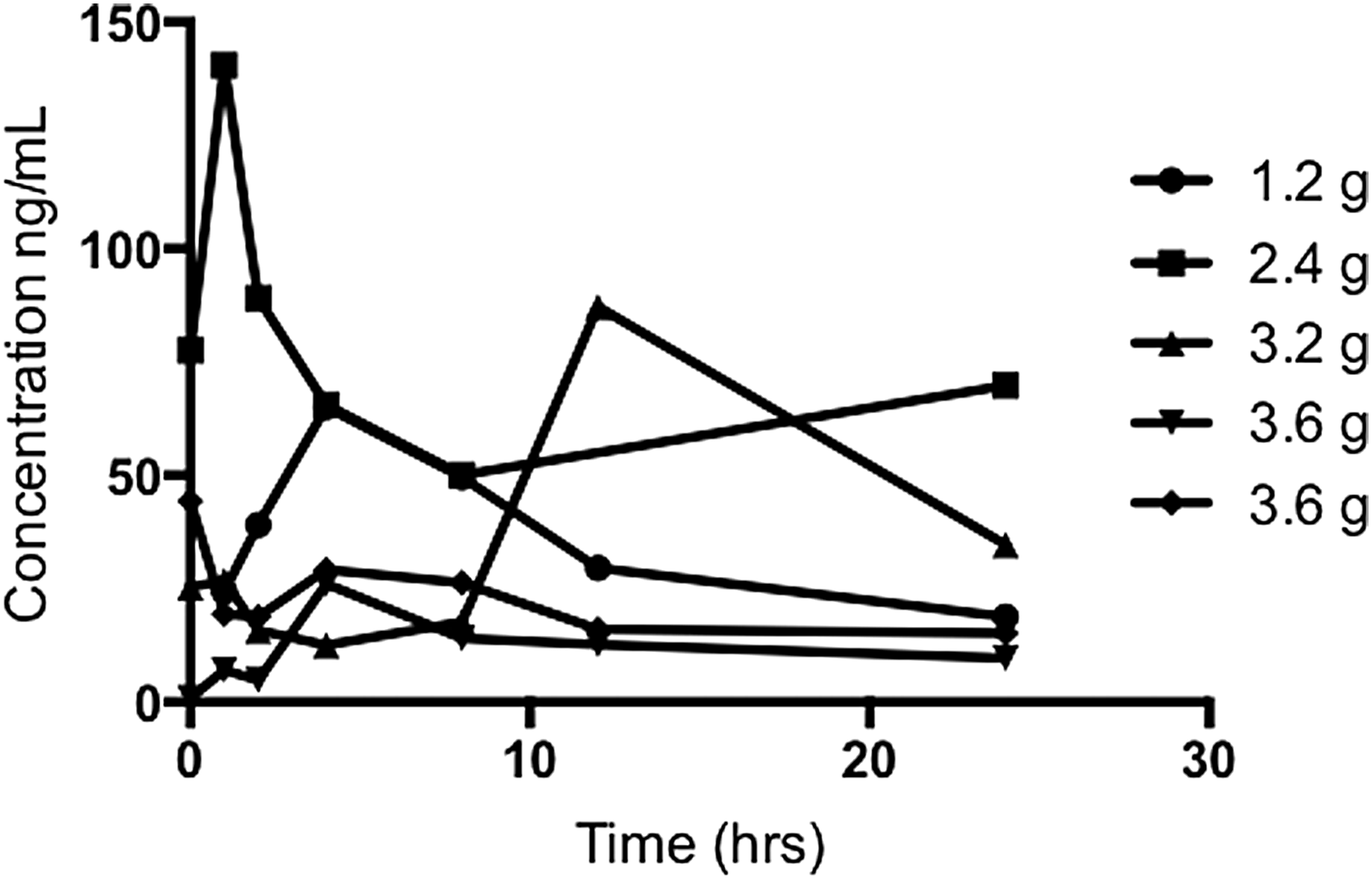
High variability observed in concentration time curve in different individuals taking low daily dosages of mesalamine.

High variability observed in concentration time curve in different individuals taking high daily dosages (4.8 g) of mesalamine.
Pharmacokinetics Parameters of Various Dosages of Mesalamine in Breastfeeding Women (n = 10)
SEM, standard error of the mean.
Discussion
While all drugs are transferred into human milk, fortunately most drugs present in milk are not in ranges that are clinically relevant. To our knowledge, this is the first description of levels of mesalamine in human milk in mothers consuming multimatrix formulations. Our study suggests that mesalamine levels in the milk samples of 10 breastfeeding mothers were very low and likely safe during breastfeeding.
Both formulations (Lialda and Asacol HD) use a pH-dependent gastroresistant coating designed to delay the release of mesalamine until entry into the colon, a so-called “colon-delivery system.” While this complex dosage form is designed to limit the systemic absorption of mesalamine 18 in the small intestine, it also apparently produces highly variable plasma levels of both 5-ASA and its inactive N-acetylated metabolite (Ac-5-ASA) in patients. 19
Breast milk levels in our study were highly variable, indicative of the wide variability in gastrointestinal transit time using these new multimatrix colon-delivery system formulations in patients with inflammatory bowel disease. This could well be explained by differential absorption of these formulations for which two theories exist. One, the gastrointestinal transit time for mesalamine varies enormously from patient to patient, as a result of the severity of the disease. Another plausible explanation is that the pH in the colon of patients suffering from ulcerative colitis may be lower than pH 7, thus delaying dissolution. This may be due to reduced secretion of mucosal bicarbonate, increased mucosal bacterial lactate production, and impaired short-chain fatty acid absorption and metabolism.20,21
There are very few studies reporting mesalamine levels in milk samples. In 1989, Nelis found that a mother using mesalamine suppositories reported occasional watery diarrhea in her infant, which ceased when stopped using the suppositories. This case suggested that mesalamine absorbed after the rectal administration could be excreted in breast milk and subsequently produce diarrhea in breastfed infants. 17 A case report by Klotz in 1993 stated that only traces of mesalamine (dosage of 3 g per day) were absorbed, and thus dose-dependent side effects in infants were unlikely. 22
Another study by Silverman et al. in 2005 reported low levels of mesalamine in breast milk. They obtained milk samples from four breastfeeding mothers with inflammatory bowel disease who were taking mesalamine. Concentrations of mesalamine in the breast milk found were between 4 and 40 ng/mL, while those of its inactive metabolite N-Ac-5-ASA were 5–14.9 μg/mL. Unfortunately, the dosage and formulation of mesalamine administered to the mothers were not mentioned in the above study. 23 For the purposes of our study, we did not measure the N-Ac-5-ASA metabolite, as it is inert and inactive.
Corresponding blood samples were not collected along with milk samples to correlate the milk/plasma ratio of mesalamine, posing a potential limitation to our study. Nonetheless, the RIDs are found to be in low amounts irrespective of different dosages and different formulations.
Conclusions
The concentrations of mesalamine in the breast milk of mothers receiving the newer multimatrix mesalamine formulations were found to be exceedingly low in our study. While the variability of reported levels was high, this is clearly due to the altered kinetics induced by this disease state. Ultimately, the levels of mesalamine in milk in this study are likely subclinical to the infant. No side effects were reported in any of the infants in this study.
Footnotes
Disclosure Statement
No competing financial interests exist.