
Abstract
Abstract
Background:
Gestational diabetes mellitus (GDM) and its complications are major concerns because of the negative effects of GDM during antenatal period and on the future health of mothers and infants. Breastfeeding is beneficial for GDM mothers and their babies to reduce future health risks. Little is known about the link between GDM and the duration of “any” breastfeeding. Therefore, the aim of this study was to investigate the relationship between GDM and the duration for which Vietnamese women breastfeed their babies postpartum.
Materials and Methods:
A prospective cohort of 2,030 pregnant women between 24 and 28 weeks of gestation was recruited. GDM status was determined using a 75 g oral glucose tolerance test. Included mothers were then followed up from discharge after childbirth until 12 months postpartum to determine their breastfeeding duration. Kaplan–Meier estimates, log-rank tests, logistic and Cox regression models were used to examine the association between GDM and breastfeeding outcomes.
Results:
In our cohort, 94.4% of all women reported “any” breastfeeding at discharge and 72.9% of women were still breastfeeding at 12 months postpartum. The risk of early breastfeeding cessation was higher in GDM women than their non-GDM counterparts after adjustment for demographic factors (hazard ratios [HR] = 1.39, 95% confidence intervals [CI] = 1.13–1.71, p = 0.002), and all potential confounding factors (HR = 1.38, 95% CI = 1.12–1.70, p = 0.002). There were no significant differences in breastfeeding outcomes at discharge (early initiation, prelacteal feeding, and “any” breastfeeding rate) between GDM and non-GDM mothers.
Conclusions:
GDM was associated with shorter breastfeeding duration. Women with GDM require ongoing support after hospital discharge to maintain long-term breastfeeding.
Introduction
Gestational diabetes mellitus (GDM) is defined by the World Health Organization (WHO) as carbohydrate intolerance resulting in hyperglycemia with onset or first recognition during pregnancy. 1 The prevalence of GDM is increasing worldwide, which can have long-term effects on maternal health. In 2016, the reported prevalence of GDM was highest in the Middle East and North African region at 12.9% (8.3–24.5%), followed by Southeast Asia at 11.7% (8.1–18.3%). 2 However, a recent meta-analysis of the prevalence of GDM in Eastern and Southeastern Asia indicated that the pooled prevalence of GDM was 10%, and Vietnam had the highest prevalence at 20%. 3
It is well documented that mothers with GDM have higher rates of gestational hypertension, preeclampsia, and later type 2 diabetes.4,5 The health of infants may also be affected during the perinatal period with increased rates of macrosomia, neonatal hypoglycemia, as well as the future development of obesity and chronic diseases.5,6 Previous studies have suggested that women with GDM who breastfeed their infants are associated with a lower risk of adverse health outcomes.7–12 Similarly, results from a meta-analysis indicated that breastfed infants were less likely to develop type 2 diabetes later in life compared with their nonbreastfed counterparts. 13
Infants born from GDM mothers are more likely to suffer from neonatal complications such as preterm birth, low birth weight, admission to intensive care unit, which result in delaying breastfeeding at discharge. 14 Besides, mothers with GDM are at higher risk of having lactation difficulties including pain after caesarean section, breast engorgement, obstetric complications, and delayed onset of lactogenesis II.7,15–18 Therefore, rates of exclusive and predominant breastfeeding seemed to be lower for mothers with GDM at hospital discharge.19–21 However, previous studies have shown inconsistent results concerning the impact of GDM on “any” breastfeeding duration.22–26 There has also been a lack of studies in Asia, apart from two studies in Singapore and India, where the prevalence of GDM was rising.25,27 The objective of this study was to investigate the association between GDM and “any” breastfeeding duration within 12 months postpartum in Vietnamese women.
Materials and Methods
Design
This study utilized data from a multicenter prospective cohort study on maternal lifestyle and diet in relation to pregnancy, postpartum, and infant health outcomes in Vietnam. 28 Data were collected from August 2015 to December 2017, at six hospitals across three cities of Vietnam. A total of 2,248 pregnant women were invited at their antenatal care visits between 24 and 28 gestational weeks; among them, 218 women refused (9.7%) and 2,030 (90.3%) agreed to participate in the study. No difference in mean age was found between participants and nonparticipants. Detailed information about the recruitment and the catchment area, including a flowchart of the cohort, was given elsewhere. 28 These women and their babies then were followed up at hospital discharge (after child birth), and at home at 1, 3, 6, and 12 months postpartum. The study protocol was approved by the Curtin University Human Research Ethics Committee (HR32/2015) and Hai Phong University of Medicine and Pharmacy Human Research Ethics Committee (No. 05/PHUMPRB).
Participants
Participants were pregnant women who (1) were permanent residents in the study locations, (2) ≥18 years of age, (3) at 24–28 weeks of gestation, (4) had a singleton pregnancy, (5) did not have any serious preexisting health conditions (as indicated in medical records), and (6) were able to read the information sheet and sign the consent form. However, during the course of the study, 25 women were removed from the analysis based on our exclusion criteria, as follows: (1) with serious maternal health problems or who did not otherwise allow their babies to be breastfeed (n = 2 with human immunodeficiency virus, n = 1 baby transferred to an orphanage); (2) who terminated their pregnancy because of intrauterine growth restriction (n = 1), endured a still birth (n = 8) or infant death within 12 months (n = 7); and (3) mothers with prepregnancy type 1 or type 2 diabetes (n = 6).
Main exposure
The 2-hour 75 gram oral glucose tolerance test (2 h 75 g OGTT) was used to determine the GDM status of participants. It is routine practice at the participating hospitals for all mothers to have the 2 h 75 g OGTT between 24 and 28 weeks of gestation. The test involves collecting three blood samples at fasting, at 60 and 120 minutes. As indicated by the criteria from the International Association of Diabetes and Pregnancy Study Groups for GDM, GDM is evident if at least one glucose value is above the thresholds. The thresholds are as follows: fasting plasma glucose ≥5.1 mmol/L, 1-hour plasma glucose ≥10.0 mmol/L, and 2-hour plasma glucose ≥8.5 mmol/L 29
Outcome measures
In this study, breastfeeding practices were defined according to the WHO criteria. Reference to “any” breastfeeding meant “when a child had received breastmilk (direct from the breast or expressed or stored breastmilk) with or without other drink, formula or other infant food.” Early initiation of breastfeeding signified the situation where “the mother puts her newborn to the breast within one hour of birth.” Prelacteal feeds were categorized as any feeds given to the infants before the initiation of mother's breastfeeding. 30
Infant feeding was assessed in five face-to-face interviews through the question “How are you feeding your baby?” at discharge, 1, 3, 6, and 12 months. Breastfeeding duration was recorded in weeks by asking “How old was your baby when you stopped breastfeeding?” Early initiation of breastfeeding and prelacteal feed were recorded at hospital discharge using the following questions “What was your baby's first feed after he/she was born?” and “How long after delivery did you first breastfeed your baby?”
Other variables
Factors to be considered as confounders were determined from the literature.23,24,26,31 These included maternal demographic characteristics (age [years], occupation, education, and parity) collected at the baseline interview. Obstetric complications and birth outcomes were obtained from medical records at hospital discharge, including gestational age (weeks), birth weight (g), caesarean section (yes/no), and infant admission to neonatal intensive care unit (yes/no).
Statistical analysis
The main outcome measure was “any” breastfeeding duration and the primary exposure was GDM status. Data were analyzed using the IBM SPSS package version 22 (IBM, Armonk, NY). Group comparisons were made between women with and without GDM using the chi-square test for categorical variables and the t test for continuous variables. Kaplan–Meier curves were used to compare breastfeeding duration for subgroups of interest. Crude and adjusted hazard ratios (HR) and associated 95% confidence intervals (CI) were reported using Cox's regression model. Logistic regression with odds ratio was used for the multivariable analysis of breastfeeding rates. Covariates included in the regression models were maternal age, occupation, maternal education, parity, gestational age, birth weight, caesarean section, and infant admission to neonatal intensive care unit. The rationale was to ascertain the association between GDM and breastfeeding outcomes accounting for the effects of such mediators and confounding factors.
Results
A total of 2,030 pregnant women (462 GDM, 1,561 non-GDM, and 7 prepregnancy diabetes) were recruited at baseline. In addition to the 25 women excluded based on the previously mentioned exclusion criteria, 296 women subsequently refused to participate or were unable to follow-up during the 12-month postnatal period. The final sample consisted of 1,709 women (Fig. 1). There were no differences in maternal age, parity, and other demographic characteristics between the loss to follow-up group and the completion group, except occupation and education level (p < 0.05).
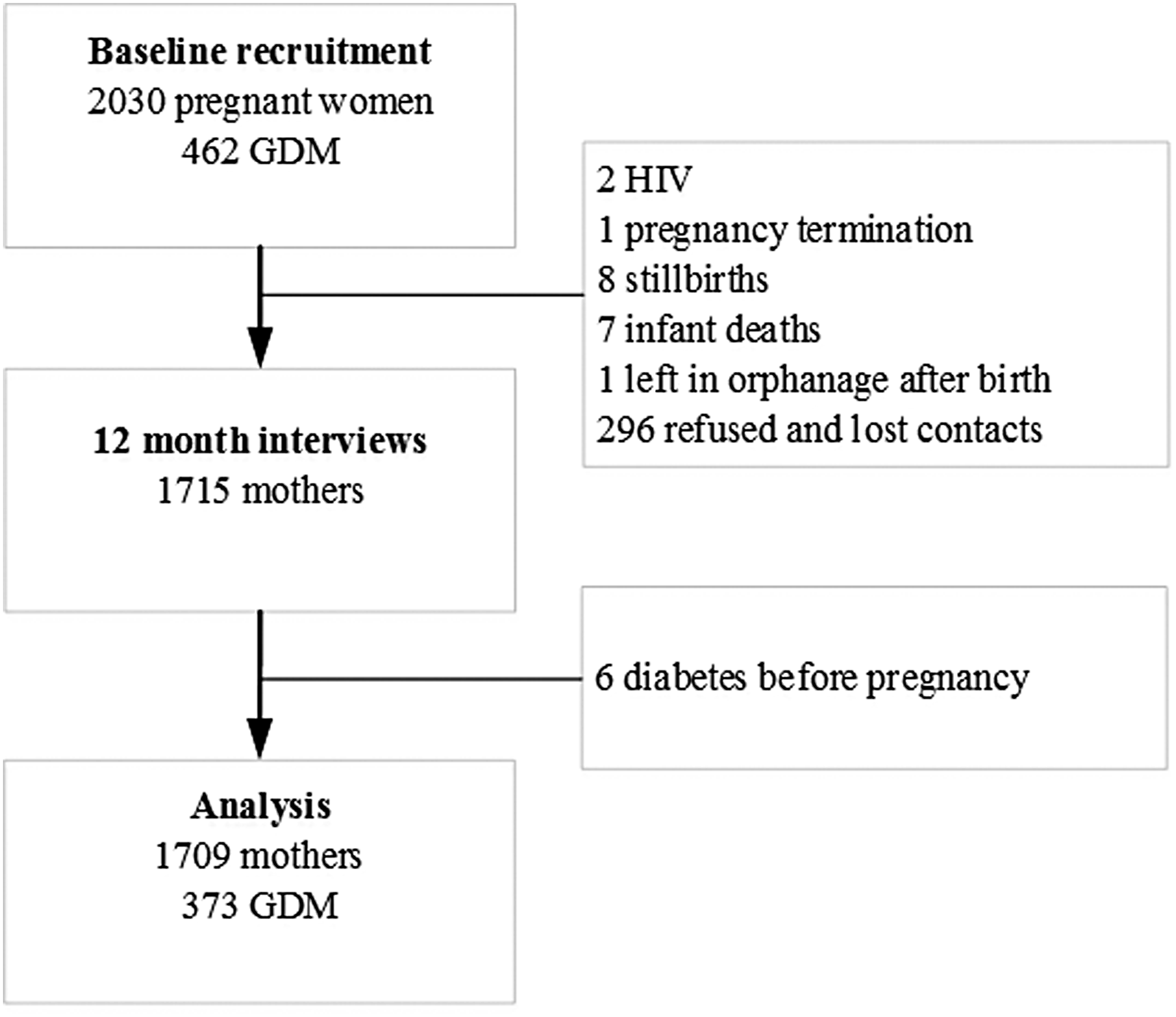
Flowchart of included participants.
Table 1 describes the demographic and perinatal characteristics of participants with GDM (n = 373) and without GDM (n = 1,336). In the GDM group (21.8% of the final sample), 17 women were diagnosed as having diabetes according to the diagnostic criteria of WHO 2013. 32 Women with GDM were significantly older, had shorter gestation, and were more likely to have caesarean section compared with those without GDM.
Characteristics of Participants With and Without Gestational Diabetes (N = 1,709)
GDM is confirmed based on criteria of the International Association of Diabetes and Pregnancy Study Groups criteria. 29
GDM, gestational diabetes mellitus; SD, standard deviation; NICU, neonatal intensive care unit.
In Table 2, other breastfeeding outcomes namely rate of early breastfeeding (within 1 hour), rate of prelacteal feed, rates of “any” breastfeeding at discharge, at 1, 3, 6, and 12 months postpartum were compared between GDM and non-GDM women. About one in three women initiated breastfeeding within the first hour of delivery, and 56.6% of the infants received something other than breast milk within 24 hours of birth. The “any” breastfeeding rate at discharge was 91.4%, and nearly 73% of women still breastfed at 12 months. Breastfeeding rates at 1, 3, and 6 months were higher in the non-GDM group but no significant differences were found after adjustments for first demographic factors, and second for all confounders, with the exception at 12 months postpartum (Table 2).
Breastfeeding Outcomes for Mothers With and Without Gestational Diabetes (N = 1,709)
GDM is confirmed based on criteria of the International Association of the Diabetes and Pregnancy Study Groups criteria. 29
Adjusted for maternal age, occupation, maternal education, and parity.
Adjusted for maternal age, occupation, maternal education, parity, gestational age, birth weight, caesarean section, and infant admission to Neonatal Intensive Care Unit.
Breastfeeding within 1 hour after birth.
OR, odds ratio; CI, confident interval.
Only 18.8% of women “exclusively” breastfed and 20.8% of women “predominantly” breastfed at discharge, and the rates of “exclusive” and “predominant” breastfeeding at 6 months were 2.0% and 2.5%, respectively. “Exclusive” and “predominant” breastfeeding rates at the various time points were lower among GDM women and for early initiation of breastfeeding, but not statistically different from those of the non-GDM group.
Assuming all women started breastfeeding at the same point after delivery (week 0), results from the rank-sum test showed a significant difference between the two groups of women (p = 0.0008). That is, women with GDM had shorter duration of breastfeeding than the non-GDM women. The Kaplan–Meier curves comparing the difference in any breastfeeding duration within 12 months between GDM and non-GDM women are given in Figure 2.
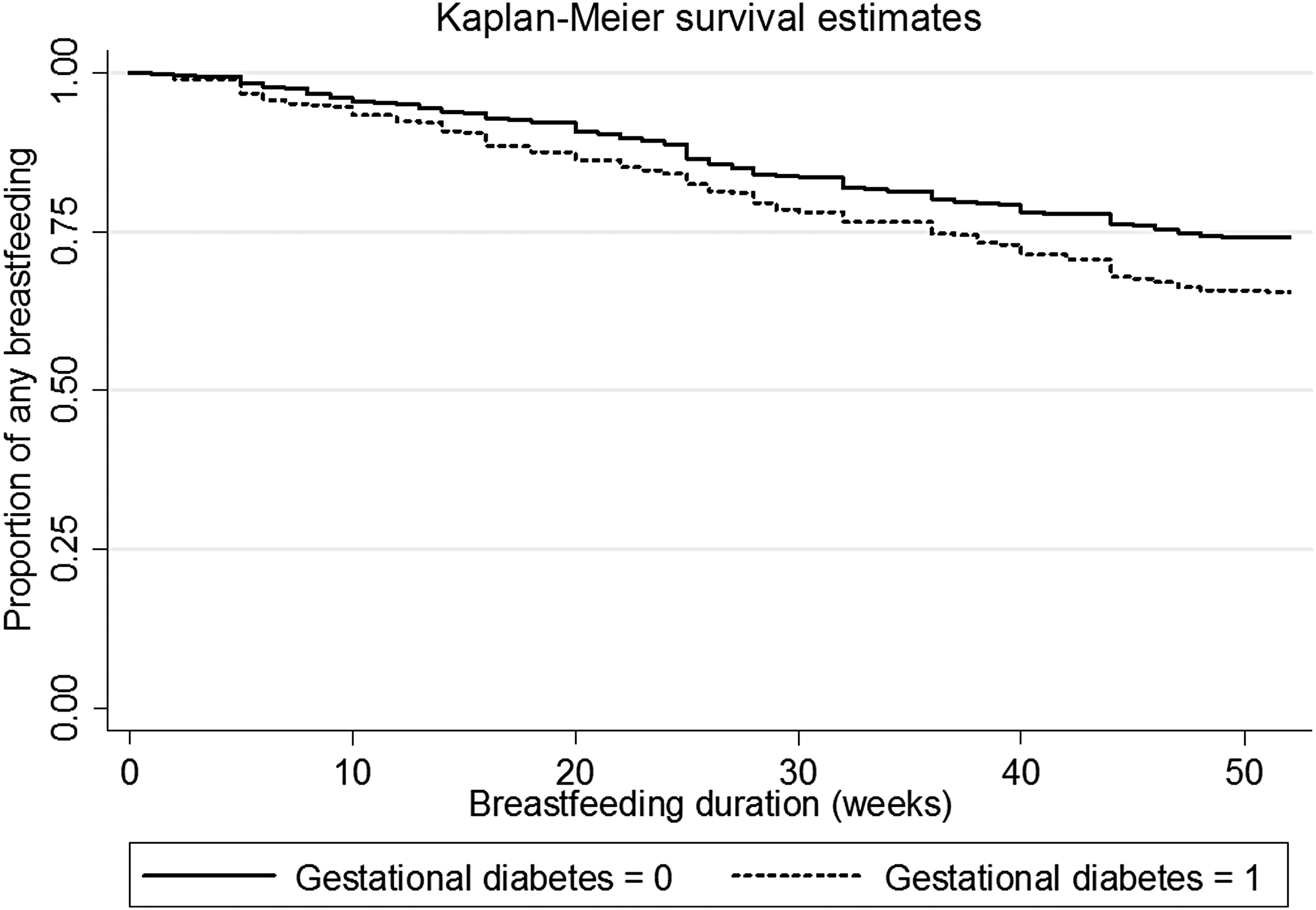
Kaplan–Meier curves of any breastfeeding in the first 12 months postpartum for mothers with and without gestational diabetes.
The crude model without covariates suggested that GDM was associated with early breastfeeding cessation (HR = 1.41, 95% CI = 1.15–1.73, p = 0.001). After adjusting for both demographic factors and all potential confounders, the inverse association between GDM and breastfeeding duration remained significant (Table 3). Moreover, maternal age, occupation (office staff and housewives), maternal education, and caesarean section were found to be influencing factors on the breastfeeding duration, as evident from their corresponding adjusted HR (95% CI) given in Table 3. We further investigated glucose intolerance using the blood glucose levels from the 2 h 75 g OGTT, which showed their significant association with the early cessation of any breastfeeding; details of the Cox regression results are not presented for brevity.
Adjusted Hazard Ratios of Gestational Diabetes Mellitus and Breastfeeding Duration Using Cox's Regression (N = 1,709)
Adjusted for maternal age, occupation, maternal education, and parity.
Adjusted for maternal age, occupation, education, parity, gestational age, birth weight, caesarean section, and infant admission to neonatal intensive care unit.
HR, hazard ratio.
Discussion
This study indicates that mothers with GDM tend to have shorter breastfeeding duration. Our findings from Vietnam are consistent with the literature reports from western countries.24,26,33 We also confirmed that glucose intolerance was significantly associated with early breastfeeding cessation. 34 However, the rate of “any” breastfeeding at discharge was the same for GDM and non-GDM mothers, similar to the results from the United States.19,35,36 Other studies that examined “any” breastfeeding duration by predominantly dividing into categorical scales found no differences, including two Asian studies.25,27,31,37,38
Several studies have examined “exclusive/predominant/full” breastfeeding outcomes. In comparison, despite the finding of this study that “exclusive” and “predominant” rates were slightly lower among GDM women at different time points, no significant differences were evident because of their very low rates in Vietnamese women.18–21,35 Although two previous studies mentioned GDM and breastfeeding in Asia,25,27 this is the first study in a developing country that examined the association between GDM and both short- and long-term breastfeeding outcomes. Strengths of this study are as follows: multicenter longitudinal study with a large sample size, involving prospective measurements of breastfeeding duration (weeks) with five times interviews from discharge to 12 months; standard definitions of WHO were applied for breastfeeding indicators; GDM status was assessed at baseline using the International Association of Diabetes and Pregnancy Study Groups criteria; and use of regression models adjusting for the effects of demographic and other plausible confounding factors.
The possible causes of adverse breastfeeding outcomes at discharge among GDM women in previous reviews include the following: the higher rates of obstetric and neonatal complications for both infants and GDM mothers, and delays in the onset of lactogenesis II.7,15 Consequently, the suboptimal breastfeeding at hospital discharge lead to early breastfeeding cessation. 8 Women with insulin-treated GDM were less likely to breastfeed than other women. 21 Although the advantages of breastfeeding for GDM women had been documented, GDM status was not associated with the perceived benefits of breastfeeding and breastfeeding duration. 22 Recently, a study about breastfeeding knowledge, attitudes, and beliefs during pregnancy and hospital breastfeeding experiences found that women with GDM were less likely to say that “breastfeeding is the best way to feed an infant,” and more likely to say “their physicians prefer formula.” 39 However, programs that aimed to educate and support them with breastfeeding showed effectiveness in terms of increasing breastfeeding duration. 40
There are several limitations to be considered when interpreting the results of this study. Although participants were recruited from six hospitals of three cities, the sample might not necessarily be representative of the entire Vietnam. Moreover, the regression models focused on confounding factors related to maternal and birth outcomes, but not social, parental factors and professional supports. Information on any GDM treatment(s) was also not available that may affect a mother's decision to breastfeed. 21
Conclusion
In this prospective cohort study of Vietnamese pregnant women, it was found that GDM was significantly associated with a shorter duration of any breastfeeding. Given the well-recognized benefits of breastfeeding for women and their infants, midwives and medical staff should be aware of the increased risk of early breastfeeding cessation among mothers with the condition. Extra support for these women to prolong and sustain their duration of breastfeeding after hospital discharge should be routinely provided.
Footnotes
Acknowledgments
The authors thank all women who participated in this study and the hospitals and data enumerators for their support in data collection.
Funding
This work was partially supported by Curtin University, Perth, Western Australia, Australia.
Disclosure Statement
No competing financial interests exist.