
Abstract
Abstract
Background:
Human breast milk (HBM) is considered inadequate in meeting protein requirements, especially for very low birth weight (VLBW) infants, which could affect body composition.
Objectives:
The primary objective was to determine the effect of HBM on body composition of HIV-exposed and unexposed preterm VLBW and extremely low birth weight infants. The secondary objectives were to ascertain the effect breast milk fortification and days nil per os (NPO) have on body composition.
Materials and Methods:
A descriptive cross-sectional study was conducted. Preterm infants with a birth weight of ≤1,200 g were included. Infant nutritional intakes and body composition measurements were recorded during the 28-day follow-up period.
Results:
One hundred ten of 113 preterm infants received HBM and 91 infants received fortified HBM. HIV-exposed and unexposed infants receiving fortified HBM displayed differences in fat mass percentage (FM%) (0.88% versus 1.36%, p = 0.01; 0.97% versus 1.49%, p = 0.03) and fat-free mass percentage (FFM%) (98.98% versus 98.68%, p = 0.03; 99.02% versus 98.49%, p = 0.02) on days 21 and 28, respectively. Infants kept NPO displayed differences in FM% on days 7, 21, and 28 (0.9% versus 1.3%, p = 0.03; 0.99% versus 1.4%, p = 0.02; and 0.9% versus 1.6%, p = 0.0004) as well as differences in FFM% (99.1% versus 98.4%; p = 0.0005) on day 28 of life.
Conclusion:
There were no significant differences in the body composition of infants who received HBM versus fortified HBM. However, significant differences in body composition were reported between HIV exposure groups for infants who received fortified HBM. Infants who were kept NPO were generally smaller, shorter, and had lower FM% and more FFM%.
Introduction
Over the past two decades, South Africa has experienced a serious HIV epidemic and is home to the world's largest HIV population. 1 HIV-infected pregnant mothers on highly active antiretroviral therapy have a considerably higher risk (13–34%) of delivering an infant preterm.2,3
A recent study conducted in Africa by Omoni et al. 4 found that HIV-exposed uninfected (HIV-EU) infants had poorer growth than HIV-unexposed uninfected (HIV-UU) infants during infancy. Previous literature confirms that HIV-EU infants grew more poorly and had increased early mortality and morbidity rates compared with HIV-UU infants.4–6 For the purposes of this article, the terms HIV-EU and HIV-UU infants will be referred to as HIV-exposed and HIV-unexposed infants, respectively.
The aggressive nutritional management recommended for preterm and small-for-gestational-age infants by the American Association of Pediatrics to achieve appropriate fetal growth rates and body composition could result in an increased risk of cardiovascular diseases and metabolic syndrome later on in life. These risks are related to high early postnatal weight gain.7,8 This was supported in a meta-analysis by Johnson et al., 9 detailing the relationship between nutritional intakes and body composition in preterm infants. Nutritional intakes include micronutrients and macronutrients (energy and protein), and their effect on the successful growth and body composition of preterm infants at term-equivalent age. Preterm infants, especially those born with a birth weight <1,500 g (very low birth weight [VLBW]), are a challenge to feed because of the high recommended daily allowance of energy, protein, and nutrients required to achieve in-utero growth rates.8,10
Human breast milk (HBM) alone is considered inadequate to meet the nutritional requirements of preterm infants during early neonatal life, especially among infants born with VLBW. 11 When fed in amounts that satisfy energy requirements, HBM provides only ∼60% of the protein requirements.12,13Therefore, HBM from mothers with preterm infants is not nutritionally adequate, and must be fortified to ensure adequate growth and body composition in terms of fat mass (FM) and fat-free mass (FFM). There are three main fortification strategies, namely standard fortification, super fortification, and individualized (adjustable and targeted fortification). These strategies range from simple, quick, safe, and inexpensive to complex, sophisticated, and expensive.12,14,15,a Supplementation of HBM with a fortifier (energy, protein, vitamins, and minerals) is common practice in many neonatal intensive care units (NICUs) to achieve nutritional requirements and successful intrauterine growth rates in preterm infants, while the many benefits of HBM such as better neurodevelopmental outcomes and a decrease in late-onset sepsis and necrotizing enterocolitis (NEC) continue to be recorded.10,12,16
The Baby Friendly Hospital Initiative (BFHI) was launched by the World Health Organization (WHO) and United Nations Children's Fund as a global initiative to protect, promote, and support breastfeeding practices by adhering to and implementing the minimum global criteria contained in “The ten steps to successful breastfeeding” guidelines. 17 These guidelines are critical to the prevention of mother-to-child transmission (PMTCT) program.18–20 The attending doctor should only prescribe a formula feed once all other options to administer HBM have been exhausted, such as when the mother is unable to produce or express breast milk, also known as mother's own milk (MOM), and donor breast milk (DBM) is unavailable.
Strydom et al. 21 recently reviewed the various assessment techniques to assess body composition on preterm infants. This review concluded that the Dauncey anthropometric model method, which includes skinfold thickness at two primary sites and measures nine body dimensions, is one of the best methods to determine body composition in terms of FM and FFM in a low-middle income country (LMIC) with limited resources. This method of assessing body composition is accurate, safe, inexpensive, and noninvasive, and can be performed at the bedside table. 22
There is a gap in published research regarding the relationship between HIV, breast milk intake, body composition, and preterm infants and the effect thereof on the quality of growth and body composition, in terms of FM and FFM.9,23,24 The purpose of the study was to evaluate the effect of HBM intake (and the fortification thereof), and the body composition of HIV-exposed and HIV-unexposed preterm VLBW and extremely low birth weight (ELBW) (<1,000 g) infants.
Materials and Methods
Study design and setting
This descriptive cross-sectional study, which formed part of a larger cohort, was conducted from May 16 to October 22, 2016, in the Neonatal Unit of Tygerberg Children's Hospital (TBCH) situated in Tygerberg Academic Hospital (TAH), Cape Town, South Africa. More details pertaining to this cohort (background, demographic information, methods, and measurements) have previously been published.21,22
Sample size
The sample sizes needed of the study populations were determined according to the live birth statistics for infants born with a birth weight <1,500 g (VLBW) at the institution. A power analysis using two-way analysis of variance (ANOVA) with a power of 90% to detect interaction effects of δ = 0.49 (regarded as a medium effect size) yielded a required sample size n = 23 in each of the exposure groups. Of the total sample size of n = 113 preterm infants, 83 were HIV-unexposed preterm infants and 30 were HIV-exposed preterm infants.
Participants
Participants were included in this study for a 28-day follow-up period (day 1 was considered as the first 24 hours of life). Infants were included if the following inclusion criteria were met: (1) all male and female HIV-exposed and HIV-unexposed preterm infants with a gestational age (GA) of ≥25 to <37 weeks; (2) birth weight ≥500 to ≤1,200 g; (3) receiving nutritional support in the form of enteral nutrition (EN) and/or parenteral nutrition (TPN) (EN: breast milk and supplementation thereof [FM85], formula feed and TPN); and (4) written parenteral consent. Infants from multiple gestations meeting these criteria were included in the study. Infants were excluded from the study if the following occurred: (1) all male and female HIV-exposed and HIV-unexposed preterm infants with a GA <25 or ≥37 weeks; (2) birth weight <500 and >1,200 g; (3) major congenital malformations and/or developmental disabilities; (4) infants who displayed disorders or conditions that could affect body composition (edema, myopathy); and (5) infants with major gastrointestinal abnormalities; and infants who had a positive PCR at birth. The researchers collected the maternal medical background of each infant with inclusion. Infant clinical, medical, and nutritional data were collected on a daily basis, and anthropometric and skinfold measurements were taken weekly.
Outcomes
The primary outcome of the study was to determine the effect of HBM intakes on the body composition of HIV-exposed and HIV-unexposed preterm, VLBW, and ELBW infants. The secondary outcomes also included the effect of Breast Milk (BM) fortification, feeding intolerances and days on which infants were nil per os (NPO). The Dauncey anthropometric model method was used to determine body composition in terms of FM and FFM.
Methods
Participants were included in this study for a 28-day follow-up period (day 1 was considered as the first 24 hours of life). The researchers collected the maternal medical background of each infant with inclusion. Infant clinical, medical, and nutritional data were collected on a daily basis, and anthropometric and skinfold measurements were taken weekly.
The researchers documented all fluid input and output from the patients' fluid balance charts. The daily clinical assessments were done by the attending doctors, and were recorded by the researchers or research assistants. For the duration of the study, milk feeds were advanced according to the standard ward protocol, and feeds were increased in daily increments of ∼25–30 mL/kg/day. The time of initial feeding was at the discretion of the attending physician.
The primary nutritional intake prescribed for preterm infants (according to the national consolidation guidelines regarding the PMTCT of HIV)18,20 for this research study was HBM, which included MOM, DBM, pasteurized breast milk (PBM), and HBM fortified with a standard agent known as FM85. 25 Furthermore, in line with ward protocol, infants of HIV-infected and HIV-uninfected mothers received PBM or DBM or unpasteurized BM (expressed, donor, or breastfed), respectively. The BM of HIV-infected mothers was pasteurized using the Pretoria pasteurization method, 26 which was the standard protocol in the ward.
The ward protocol prescribed the fortification of MOM in TBCH 25 for breastfed preterm infants who were born <34 weeks GA and weighed <1,800 g, and breastfed preterm infants who did not grow at a rate of 15 g/kg/day and had to receive full fluid requirements (150–180 mL/kg/day). For the duration of the study, the standard protocol was applied, namely the BM fortifier was added at a ratio of 1 g to 20 mL MOM. The standard addition of 5 g of fortifier to 100 mL MOM increased the energy and protein concentration from ±67 kcal to 85 kcal/100 mL BM and 1.2 g to 2.2 g/100 mL, respectively. 25
In addition, the following data were assessed and recorded daily: feeding route, the volume of HBM, formula, TPN, Neonatalyte (glucose–electrolyte-containing solution) and saline provided to the infant, standard BM fortifier and medium-chain triglyceride oil, multivitamin supplementation, phototherapy and blood products received, medication administered, urinary output, stool frequency and color/consistency, and feeding intolerance frequency.
The researcher assessed body composition using the Dauncey anthropometric model method, by measuring nine dimensions and two skinfolds. The body dimensions included circumferences (head, chest, mid-upper arm, mid-thigh, and mid-calf) and lengths (upper arm, lower arm, supine length, and crown-rump length). Skinfold thickness was measured at two primary sites: triceps and subscapular. The skinfold thickness measurements of each infant were taken on day 1 of the study and subsequently measured on a weekly basis. Upon exiting the study (day 28), the skinfold thickness was measured again. Five measurements were thus recorded: on days 1, 7, 14, 21, and 28. Skinfold thickness was determined using Holtain skinfold calipers, with a calibration sensitivity of 0.1 mm and divisions of 0.2 mm. The same pair of calipers was used for all measurements and was calibrated before each measurement period. All skinfold measurements were taken on the right-hand side of the body, and only two measurements at each body site were assessed owing to the fragility of the study population and to ensure minimal invasion.27–30 In cases where the results differed by >0.5 mm, a third measurement was taken. No skin fold measurements were done while infants weighed ≤700 g.
The Dauncey anthropometric method was used to determine total FM and FFM by assessing skinfold thickness at two sites (triceps and subscapular) in conjunction with nine other body dimensions. These body dimensions were circumferences (head, chest, mid-upper arm, mid-thigh, and mid-calf) and lengths (upper arm, lower arm, supine, and crown-rump length).31,32
Ethical approval
Ethical approval was granted by the Health Research Ethics Committee of the Faculty of Medicine and Health Sciences, University of Stellenbosch and TAH, Ethics Reference No. N15/10/102.
Statistical analysis
Data analyses were performed using Statistica version 13 (Dell, Inc. [2016], Dell Statistica [data analysis software system]) in Stellenbosch, South Africa. When comparing continuous variables between two groups (anthropometric and body composition measurements for HIV exposure), one-factor ANOVA was used; if residuals were not normally distributed, a nonparametric test, the Mann–Whitney test, was used to confirm conclusions for ANOVA. Nominal variables (e.g., GA and sex) were compared between groups with contingency tables using the maximum-likelihood chi-square test. Descriptive statistics were reported in terms of the mean, standard deviation, and maximum and maximum values. Confidence intervals of 95% were used to report the mean of each group, and a p-value of <0.05 was used to determine statistical significance in this study.
Results
A total of 131 preterm infants conformed to the inclusion criteria and of these, 18 infants (14%) were excluded: 8 (6%) of the exclusions were due to the mother being unable to give consent for medical or social reasons; 6 infants (5%) died before consent was obtained, 3 mothers (2%) declined participation, and 1 infant (1%) was transferred to the NICU. The final study population consisted of 113 preterm infants; however, 2 of these infants died before enteral feeds were initiated and 1 infant exited the study due to being transferred to the NICU. Therefore, a total of 110 infants (HIV-exposed [n = 29] and HIV-unexposed infants [n = 81]) received MOM, DBM, or PBM at a given point in time during the 28-day follow-up study (Supplementary Fig. S1).
Table 1 indicates the HBM composition 33 and nutritional intake of HIV-exposed and HIV-unexposed infants. No significant difference was noted in the HBM volume (mL/kg/day), energy density (kcal/kg/day), and macronutrient concentration in terms of protein and fat (g/kg/day), in HIV-exposed and HIV-unexposed preterm infants.
Human Breast Milk Composition and Nutritional Intakes of HIV-Exposed and HIV-Unexposed Preterm Infants
Values are mean (
SD, standard deviation.
Infants in both groups were generally initiated with minimal feeds on days 2–3 of life. Even though the HBM volume was similar between the two groups for the duration of the study period, it was noted that infants in the HIV-exposed group received slightly more HBM from day 14 of life than the HIV-unexposed group. The macronutrient intake is directly proportional to the volume of HBM; therefore, HIV-unexposed infants generally had lower energy, protein and fat intakes when compared with HIV-exposed infants.
The HIV-exposed and HIV-unexposed preterm infants were compared per birth weight category (VLBW and ELBW) by a two-way ANOVA. According to this analysis, there was no statistically significant difference in the HBM composition and nutritional intakes throughout the 28-day follow-up period between the two groups.
Fortified breast milk
For the duration of this study, the standard fortification formulation, which was in existence then, was used. From 2017, however, a reformulation has been implemented in South Africa.19,a
Of the 110 infants who received HBM, 91 (83%) received fortified HBM. Of these infants, 25 (27%) and 66 (73%) were HIV-exposed and HIV-unexposed preterm infants, respectively (Table 2). There was no significant difference (p = 0.48) between the two groups in the mean number of days the infants received the BM fortifier. The HIV-exposed group did however receive the BM fortifier for fewer days 8.63 (±7.14) and for a maximum of 19 days compared with HIV-unexposed infants who received the fortifier for 9.64 (±6.73) days and for a maximum of 21 days.
Human Breast Milk Fortification and Nutrient Intakes of HIV-Exposed and HIV-Unexposed Preterm Infants
Values are mean (
NOD, number of days.
For the duration of the study, there were no statistically significant differences in body composition in terms of skinfold thickness measurements, FM% and FFM%, between infants who received fortified HBM and those who did not. However, it was noted that, for the duration of the study, infants who received the fortifier were generally smaller and did not grow at a rate of 15 g/kg/day (Supplementary Table S1).
Comparisons for a two-way ANOVA for infants receiving the fortified HBM and HIV exposure could not be made from day 7 onward as there were no HIV-exposed infants in the group “infants receiving HBM alone.” Therefore, the anthropometric and body composition measurements were determined for infants receiving fortified BM only and HIV exposure
Weekly Anthropometric and Body Composition Measurements of Infants Receiving Fortified Breast Milk
Values are mean (
These values are based on unfortified breast milk, refer to Table 2.
Statistically significant when p ≤ 0.05.
FFM%, fat-free mass percentage; FM%, fat mass percentage; SSSF, subscapular skinfold; TSF, triceps skinfold.
Significant differences were found for infants who received fortified HBM and HIV exposure for weight [on days 14, 21 and 28 (p = 0.04, p = 0.02 and
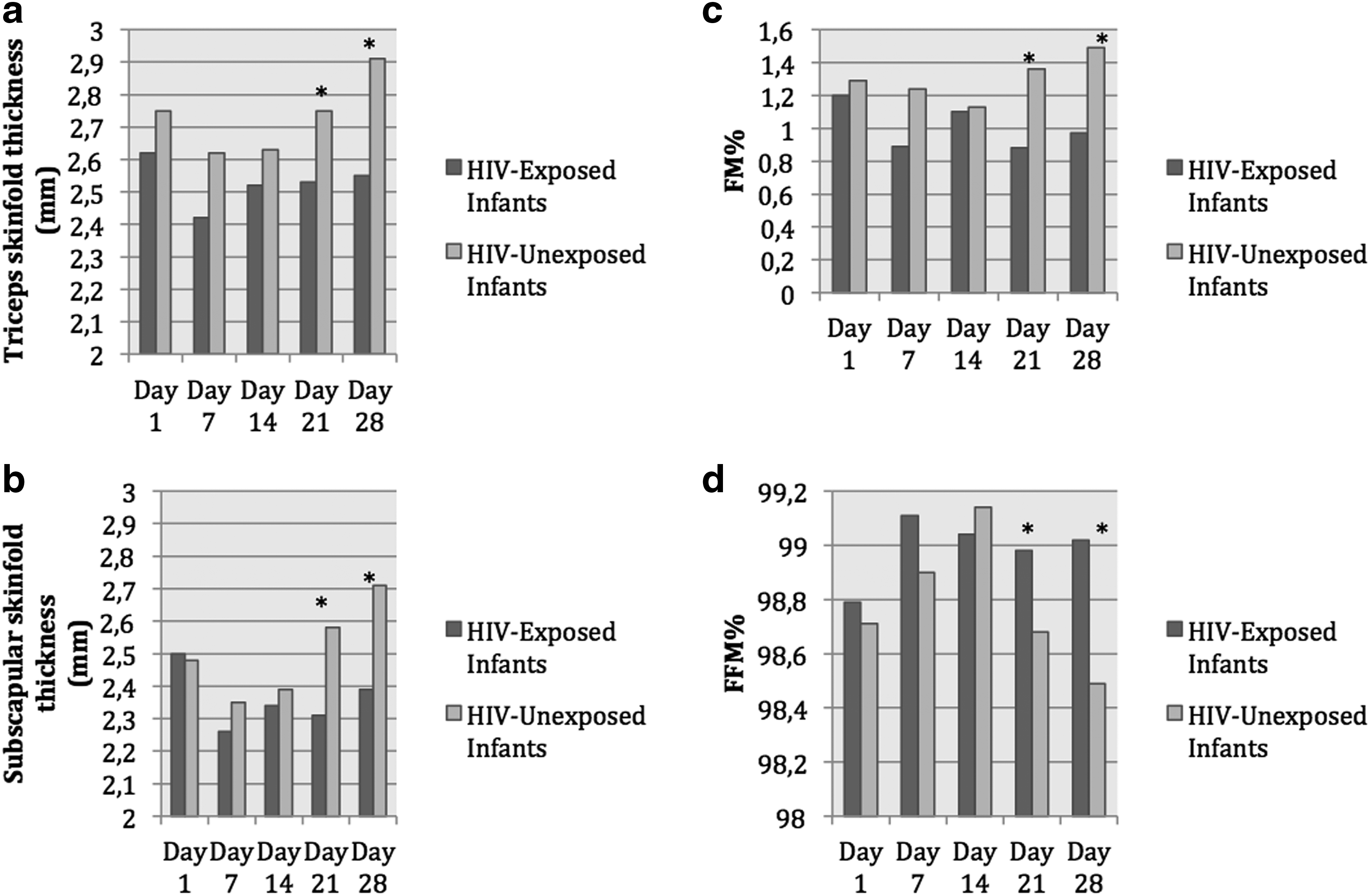
Bar graph comparing the skinfold thicknesses
Formula and total parenteral nutrition
During the 28-day follow-up study period, 5 infants (4%) received infant formula for an average of 7.6 days and 11 infants (10%) received TPN for an average of 5 days. Owing to the small number of infants who received these nutritional intakes for a short period of time, no conclusive evidence regarding body composition could be determined. However, as expected, the 10 infants (91%) who received TPN were classified as ELBW and had a significantly lower (p = 0.0012) mean birth weight 822.73 g (±132 g) when compared with infants who did not receive TPN during the 28-day follow-up period. Infants who received TPN displayed a consistent trend of being leaner with smaller TSF and SSSF thicknesses, lower FM%, and higher FFM% for the duration of the study.
All five infants who received formula were HIV unexposed. Only one HIV-exposed infant (9%) received TPN, and the remainder, that is, 10 (91%) were HIV-unexposed infants, therefore adhering to BFHI and PMTCT guidelines. Of the HIV-unexposed infants who received TPN, seven (70%) completed the 28-day follow-up study, one infant was diagnosed with NEC Bells stage II, and two infants passed away.
The effect of NPO
Table 4 depicts the anthropometric and body composition measurements of all 113 preterm infants included in this substudy, divided into the total number of days infants were kept NPO at any given time during the 28-day follow-up period. For the purposes of this study, feeding intolerance was recorded with the occurrence of a vomit or aspirate. A total of 41 infants (36%) were NPO due to suspected intolerance during the study period. Of these infants, more than three quarters (76%) were kept NPO for ≤3 days, and the remainder for >4 to ≤8 days. No infants were kept NPO for a total number of 6 days.
The Effect of Nil Per Os on the Anthropometry and Body Composition of Preterm Infants
Values are mean (
Statistically significant when p ≤ 0.05.
“—” Indicates that no measurements were obtained for the following reasons: length, infants received NCPAP, therefore length measurements were unable to be conducted; TSF and SSSF, the researchers did not conduct skinfolds on infants if they appeared critically ill or had a weight ≤700 g; FM% and FFM%, unable to calculate values according to the Dauncey anthropometric method if all anthropometric and body composition measurements were not conducted.
NPO, nil per os.
Infants who were NPO at any given point during the study revealed that, generally, the longer total number of days they were kept NPO, the smaller, shorter, and leaner they were and the higher their FFM% was. These infants displayed significant differences in FM% on day 7 (p = 0.04), day 21 (p = 0.04), and day 28 (p = 0.02) of life as well as significant differences in FFM% on day 21 (p = 0.02) and day 28 (p = 0.03) of life. Skinfold thickness was measured concurrently with FM%, and infants who were kept NPO had significant differences in TSF thicknesses on day 21 (p = 0.02) and day 28 (p = 0.04) of life, as well as significantly different SSSF thicknesses on day 28 (p = 0.02) of life (Table 4).
Discussion
This study represents one of the first to assess the nutritional intakes, and their effects on the quality of growth and body composition of HIV-exposed and HIV-unexposed preterm infants in a tertiary academic hospital in a resource-poor setting of South Africa.
Very few study infants received nutritional intakes other than HBM or fortified HBM and for a very short period of time, thereby adhering to the BFHI and PMTCT guidelines. 19 Conclusive evidence could not be determined for the effect of nutritional intakes, such as formula milk or TPN, and the possible effect of these on the body composition of HIV-exposed and HIV-unexposed preterm infants.
The European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) recommends enteral and parenteral energy intakes of 110–135 and 110–120 kcal/kg/day, respectively, and a protein intake of 3.5
Body composition, in terms of FM% and FFM%, was determined using the Dauncey anthropometric model method, which included nine dimensions and two skin fold measurements. Performing skinfold thickness measurements on this vulnerable population could perhaps be seen as an invasive method of determining body composition due to the size of the caliper when compared with the infant and the possibility of injuring the friable skin, especially in the ELBW infant. A recent review by Strydom et al. 21 concluded that the use of this method to determine body composition is accurate, safe, inexpensive, and nonexpensive, and can be performed at the bedside, especially in a LMIC with limited resources. However, great care and attention should be given by skilled and trained professionals when conducting skinfold thickness measurements on ELBW and VLNW preterm infants due to their overall fragility.
Strydom et al. 22 conducted one of the first studies in Africa to assess the body composition of HIV-exposed and HIV-unexposed preterm infants. This study found that HIV-exposed preterm infants had significantly lower birth weights and poorer growth rates, and presented with a significantly leaner body composition in terms of FM%, lower skinfold thickness measurements, and FFM% when compared with their HIV-unexposed counterparts.
A Cochrane review by Roberts et al. 35 comprising 14 randomized controlled trials and 1,071 preterm infants addressed multinutrient fortification of HBM for preterm infants. This review found that multinutrient fortification of HBM had small but statistically significant increases in growth rates (weight, length, and head circumference) for preterm infants during hospital admission, but there was a lack of data on the long-term effects of growth and development. A recent review on fortification strategies of HBM for improved in-hospital growth of preterm infants conducted in a resource-poor setting such as South Africa concluded that standard fortification did not lead to suitable in-hospital growth for preterm infants, and alternative fortification strategies should be considered. 12 In our study, the inclusion criteria comprised of the smallest and most preterm infants (GA ≤37 weeks and a birth weight ≤1,200 g) born in the institution. It was anticipated that these infants would generally have been smaller and not grow at the required rate of 15 g/kg/day, and therefore would require supplementation of fortified HBM according to the fortifying HBM indications. According to the simplified energy and protein requirement guidelines commonly used in TBCH, it is recommended that preterm infants receive 110–150 kcal/kg/day energy and a minimum of 9% protein of total energy. 25 When comparing the composition and nutritional intakes, these requirements are met when HBM is fortified with a standard agent (Table 2). It is however noted that the HBM composition used in our study was based on the average composition of preterm MOM. 33
There were no significant differences in body composition in terms of FM% and FFM% of infants who received fortified HBM and infants who did not. However, it was found that infants who were receiving fortifier generally had smaller skinfold measurements, indicating less FM% and higher FFM% compared with infants who did not receive fortifier (Supplementary Table S1). There were no HIV-exposed infants who received BM alone from day 7 onward. This could be because HIV-exposed preterm infants had poorer growth rates when compared with their HIV-unexposed counterparts. When comparing HIV exposure and infants who receive fortified HBM, it was noted that the HIV-exposed infants were generally smaller, shorter, and leaner for the duration of the study when compared with the HIV-unexposed infants. Significant differences were found in terms of TSF, SSSF, FM%, and FFM%, especially nearer to the end of the study, on days 21 and 28 of life.
A review by Hay and Thureen 36 stated that preterm FFM growth was dependent on protein intake and insufficient nutrition, and that decreased protein intakes could lead to muscle mass breakdown. Therefore, while growth alone is an important factor and requires increased amounts of amino acids and protein included in the nutritional intakes of preterm infants these are also essential for cell and tissue replication and growth.36–38
This study noted that the weight and body composition of preterm infants who were kept NPO at any given point in time during the 28-day study period generally had a negative association and displayed significant differences in FM% on day 7 (p = 0.04), day 21 (p = 0.04), and day 28 (p = 0.02) of life, and significant differences in FFM% on day 21 (p = 0.02) and day 28 (p = 0.03) of life. This study also found that infants who were NPO for the longest duration, a total number of 8 days during the 28-day study period, were the smallest; weighing generally <700 g for the duration of the study. Therefore, the researchers were unable to conduct skinfold thickness measurements using the Dauncey anthropometric method, and consequently body composition measures in terms of FM and FFM were inconclusive. Limited literature exists elucidating the relationship between preterm infants being kept NPO and the effect it could have on weight, growth, and body composition. 39 For this reason, a more comprehensive study should be conducted in this area.
Recommendations for future studies include a longer follow-up period to identify the effects nutritional intake has on the long-term growth and body composition of HIV-exposed and HIV-unexposed preterm infants. This study made use of reference values for the calculation of nutrient content for the feeds that were prescribed to the infants. None of these feeds (BM, DMB, PBM, or fortified HBM) were analyzed for nutrient content. Future studies should consider milk analyses to determine the exact quantity of micronutrients, energy, and macronutrients in terms of protein and fat. The strengths of this study are that it was one of the first studies in Africa to assess the effects of nutritional intakes on the growth and body composition of HIV-exposed and HIV-unexposed preterm infants.
Conclusion
This descriptive cross-sectional study of HIV-exposed and HIV-unexposed preterm VLBW and ELBW infants was conducted at an institution that has been BFHI accredited since 2005. For this reason, the majority of the study infants received nutritional intakes from HBM and fortified HBM. HIV-unexposed preterm infants achieved full fluid requirements earlier than HIV-exposed preterm infants. Preterm infants receiving fortified HBM were smaller and presented with a poorer growth rate of <15 g/kg/day. There were no significant differences in body composition of infants receiving HBM or fortified HBM. Significant differences in weight, skinfold thickness, and body composition measurements (in terms of FM% and FFM%) were found for HIV-exposed and HIV-unexposed preterm infants who received fortified HBM. This study found that infants who were kept NPO for any duration during the 28-day follow-up period were generally smaller, shorter, and had lower FM% and higher FFM%.
Footnotes
Acknowledgments
Gratitude is extended to the Neonatal Intensive Care Unit of Tygerberg Children's Hospital as well as the team that assisted with data collection, and the Division of Human Nutrition, Stellenbosch University, for their consistent support and assistance in the research project. The Centre for Statistical Consultation, Stellenbosch University, is acknowledged for assistance with the statistical analyses. The authors acknowledge and thank Dr Wanda Smith for her efficient and accurate editing work.
Authors' Contributions
K.M., E.v.N., and M.A.D. equally contributed to the design and conceptualization of the research study; D.G.N. performed the statistical analyses; K.M. and E.v.N. reviewed the data. K.M. performed data collection, contributed to the acquisition and analysis of the data, interpreted the data and drafted this article. E.v.N. and M.A.D. helped drafting and critically reviewing the article. All authors critically revised and approved the final version of the article, and agreed to be fully accountable for ensuring the integrity and accuracy of the work.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.