
Abstract
Abstract
Background:
Many women initiate breastfeeding but do not meet their duration goals, and low-income women initiate and continue breastfeeding at lower rates than their counterparts. One-on-one counseling is associated with increased breastfeeding but requires significant resources. In contrast, video education, which requires fewer resources and is effective in other health care settings, such as vaccine uptake, has gone untested for prolonging breastfeeding duration among low-income women.
Objective:
To determine whether use of an educational breastfeeding video shown individually to low-income pregnant women in the prenatal clinic would prolong duration of any and exclusive breastfeeding.
Methods:
A multicenter, randomized, controlled trial was conducted in four prenatal clinics. Low-income pregnant women were randomized to view the intervention (breastfeeding education) or control (prenatal nutrition) video in the third trimester and interviewed by telephone at 1, 3, and 6 months postpartum about infant feeding practices. Kaplan–Meier survival curves with log-rank tests and Cox proportional hazards regression were utilized to compare groups.
Results:
Of the 816 eligible women approached, 64% participated: 263 assigned to the intervention, and 259 assigned to the control. Six-month data were obtained for 211 (80%) and 220 (85%) women, respectively. Rate of breastfeeding cessation did not differ by group (hazard ratios; HR = 1.00, 95% confidence interval [CI]: 0.81–1.24 and HR = 0.93, 95% CI: 0.76–1.14, for any and exclusive breastfeeding, respectively).
Conclusion:
A single viewing of a breastfeeding education video shown in the prenatal clinic did not impact breastfeeding duration or exclusivity among low-income women in this study. Although not sufficient alone, educational videos may be useful as one component of a comprehensive program to promote breastfeeding.
Introduction
I
The World Health Organization (WHO) includes patient education as part of the Ten Steps to Successful Breastfeeding, and both one-on-one lactation consultation and peer counseling have been shown to boost rates of breastfeeding initiation, duration, and exclusivity.11–13 However, the proportion of women receiving prenatal breastfeeding education from a health care provider is small. 14 Potential barriers to providing breastfeeding education in a clinical setting include lack of time, lack of reimbursement, and inadequate provider knowledge and/or training.15–17 Interventions that can not only overcome these barriers to providing education but that also integrate into the clinical workflow are needed to increase initiation and prolong duration of breastfeeding. Video education has been used effectively for vaccine uptake, 18 bowel prep for colonoscopy, 19 and screening for breast and prostate cancer. 20 In a randomized, controlled trial among women in Singapore by Su et al., a breastfeeding education video was shown to increase rates of breastfeeding exclusivity and duration. 21 If effective in other populations, this low-cost, simple intervention could be adopted readily in the clinical setting. Thus, it was hypothesized that use of this educational video in the prenatal clinic would prolong the duration of both any and exclusive breastfeeding for up to 6 months postpartum among low-income women.
Materials and Methods
The Prenatal Video Education Study was a multisite, randomized, controlled intervention trial among low-income, pregnant women conducted at the University of Virginia and the Virginia Commonwealth University Health Systems. The study was reviewed and approved by the Institutional Review Boards at the University of Virginia, Virginia Commonwealth University, and the Virginia Department of Health. The Prenatal Education Video trial is registered at clinicaltrials.gov (NCT01623128).
From 2009 through 2012, research assistants screened the medical records of pregnant women daily for eligibility at four prenatal clinics between the two sites. Inclusion criteria included pregnant women who were 24–41 weeks gestation, WIC-eligible, and English speaking. Women with multiple-gestation pregnancy or any known contraindication to breastfeeding were excluded.
Trained research assistants recruited eligible women in clinic, obtained informed consent, and conducted enrollment interviews. Enrollment data included demographic characteristics, employment status, social support, parity, previous infant feeding experience, and intended feeding method(s). During the enrollment interview, women completed information releases for medical records for themselves and their infants. A computer-generated block randomization sequence using random block sizes of two or four, stratified by prenatal clinic, was generated by an independent statistician. Based on this sequence, consecutively numbered, sealed, opaque envelopes containing group assignment were assembled in advance by a study team member who did not recruit participants or collect data. After collecting baseline data, research assistants opened the next sequential envelope to identify which video to show the participant.
Women randomized to the intervention group viewed a 25-minute, educational breastfeeding video (“Better Breastfeeding,” ©Injoy Productions, 2008), which provided information about breastfeeding (its importance, latch, hunger cues, positioning, sore nipples, engorgement, how breast milk is made, and lifestyle issues). Women randomized to the control group viewed a 20-minute, educational video about prenatal nutrition for women and exercise during pregnancy (“Healthy Pregnancy Nutrition,” ©Injoy Productions, 2007). The video to which the participant was randomized was shown on a laptop with ear buds, either in an alcove in the waiting room and/or in the examination room, to decrease the likelihood of crosscontamination. The goal was to show the video in one continuous session without disrupting normal clinic flow. In cases of interruption, the video was started where left off at the next opportunity. A research assistant recorded whether each participant viewed the video continuously and assigned a subjective score for the level of attention paid by the participant (distracted/inattentive, average, or very focused/attentive).
Following the birth hospital stay, research assistants blinded to group assignment abstracted data from the maternal and infant medical records. These data included information about labor and delivery, hospital stay, feeding methods, and complications. Longitudinal data were then collected during follow-up telephone interviews with participants at 1, 3, and 6 months postpartum. Research assistants blinded to group assignment called each participant up to five times during the period of 1 week before, and up to 1 month following, each follow-up date. Follow-up interviews queried women on self-perceived health status, infant health, work outside the home, smoking, family support related to infant feeding, and detailed information about infant feeding practices, including breastfeeding frequency, duration, and exclusivity; introduction, frequency, and quantity of breast milk substitute; and introduction of complementary foods, including water. The same questions were asked at all three time points, with the exception of some skip patterns based on previous responses to reduce respondent burden.
Statistical analyses
The primary outcome for this analysis was duration of any breastfeeding (direct or expressed feedings) up to 6 months, with a secondary outcome of duration of exclusive breastfeeding (direct or expressed feedings) up to 6 months. The distribution of the duration of any and exclusive breastfeeding in the intervention and control groups was estimated with Kaplan–Meier survival curves, comparing the groups with the log-rank test. Hazard ratios and corresponding 95% confidence intervals (CIs) were estimated using Cox proportional hazards regression. Multivariable models were run to assess the impact of baseline variables that differed between the comparison groups. All observations were censored at 6 months. Subgroup analyses estimated and compared the duration of any and exclusive breastfeeding between the intervention and control groups stratified by the woman's prior experience with breastfeeding or intention to breastfeed. All analyses were conducted on an intention-to-treat basis, using SAS version 9.4 (SAS Institute, Cary, NC) and GAUSS version 16.0 (Aptech Systems, Chandler, AZ).
Sample size for the study was calculated based on a chi-square test of the difference in proportions, assuming 20% of women in the intervention group versus 10% of women in the control continued to breastfeed at 6 months postpartum. Estimates for breastfeeding prevalence were based on differences reported in the study by Su et al. and estimates of breastfeeding rates in the United States. 2 The study was conservatively powered on the difference in proportions to afford flexibility during the analysis. Because this test is less powerful, the calculated sample size provides more than adequate power for time-to-event analyses. A sample of 199 women in each group, or 398 total, yielded 80% power, with a two-sided significance level of 5%.
Results
Among the women whose medical records were screened (n = 2,875), just over half (n = 1,580), were found to be eligible for the study. Research assistants invited 816 of the eligible women to participate; 294 declined and 522 were enrolled, resulting in a participation rate of 64%. Of these, 263 were randomized to view the intervention video and 259 were randomized to view the control video. Outcome data were obtained for 211 (80%) of the women in the intervention group and 220 (85%) of the control group women. Loss to follow-up did not differ by intervention group (p = 0.16).
Study participants were 25 years old, on average, predominantly non-Hispanic black or white, never married, and had a high school education or less (Table 1). Women in the intervention and control groups only differed by other adults living in the home: women in the control group were more likely to live with some “other” adult, whereas women in the intervention group were more likely to live with their parent. There was no significant difference in whether the assigned video was viewed continuously without an interruption between groups (42% versus 53%; p = 0.29); more than 95% of the women in each group were rated by the research assistant as giving average or very focused attention on the video (data not shown).
For columns that do not sum to these totals, data were missing for some participants.
Mean ± SD.
Categories are not mutually exclusive.
There were few differences in maternal, infant, and birth hospitalization characteristics between the two groups (Table 2). Almost two-thirds of women overall delivered vaginally. The mean gestational age in weeks was 38.8 (standard deviation [SD] = 2.0) and 38.7 (SD = 2.0) among infants born to intervention participants and control participants, respectively, with mean birth weights in grams of 3,294 (SD = 603) and 3,289 (SD = 635). The lengths of stay for both women and their infants did not differ significantly (data not shown). Almost two-thirds of infants born to women in the intervention group experienced a complication compared with only half of infants born to women in the control group (p = 0.01). The groups also differed significantly by breastfeeding experience. While the majority of women in both groups (68% in the intervention and 65% in the control) reported no breastfeeding experience, a greater proportion of the experienced women in the control group breastfed a maximum of only 180 or fewer days compared with a maximum of 181 or more days. Neither intention to breastfeed nor initiation of breastfeeding differed by intervention group, as previously reported.22,23
For columns that do not sum to these totals, data were missing for some participants.
Maternal complications included placental abruption, uterine atony, pre-eclampsia, chorioamnionitis, methadone use, and others.
Infant complications included hypoglycemia, transient tachypnea of the newborn, other breathing problems, cardiac problem, hyperbilirubinemia, and others.
Duration of breastfeeding, either any or exclusive, did not differ by intervention group over the first 6 months (Fig. 1). Women in the intervention and control groups stopped breastfeeding at the same rate over time. The unadjusted hazard ratios (HR) and 95% CIs were as follows: HR = 1.00 (CI: 0.81–1.24) for any breastfeeding, and HR = 0.93 (CI: 0.76–1.14) for exclusive breastfeeding. When controlling for baseline variables that differed between the groups despite randomization (other adult living in the home, any infant complication, and prior breastfeeding experience), there was still no difference in the rates of breastfeeding cessation over time: adjusted HR (aHR) = 0.99 (CI: 0.79–1.24), and aHR = 0.96 (CI: 0.77–1.19), for any and exclusive breastfeeding, respectively. These findings remained the same when the analysis was performed using breastfeeding data from medical records rather than interviews.
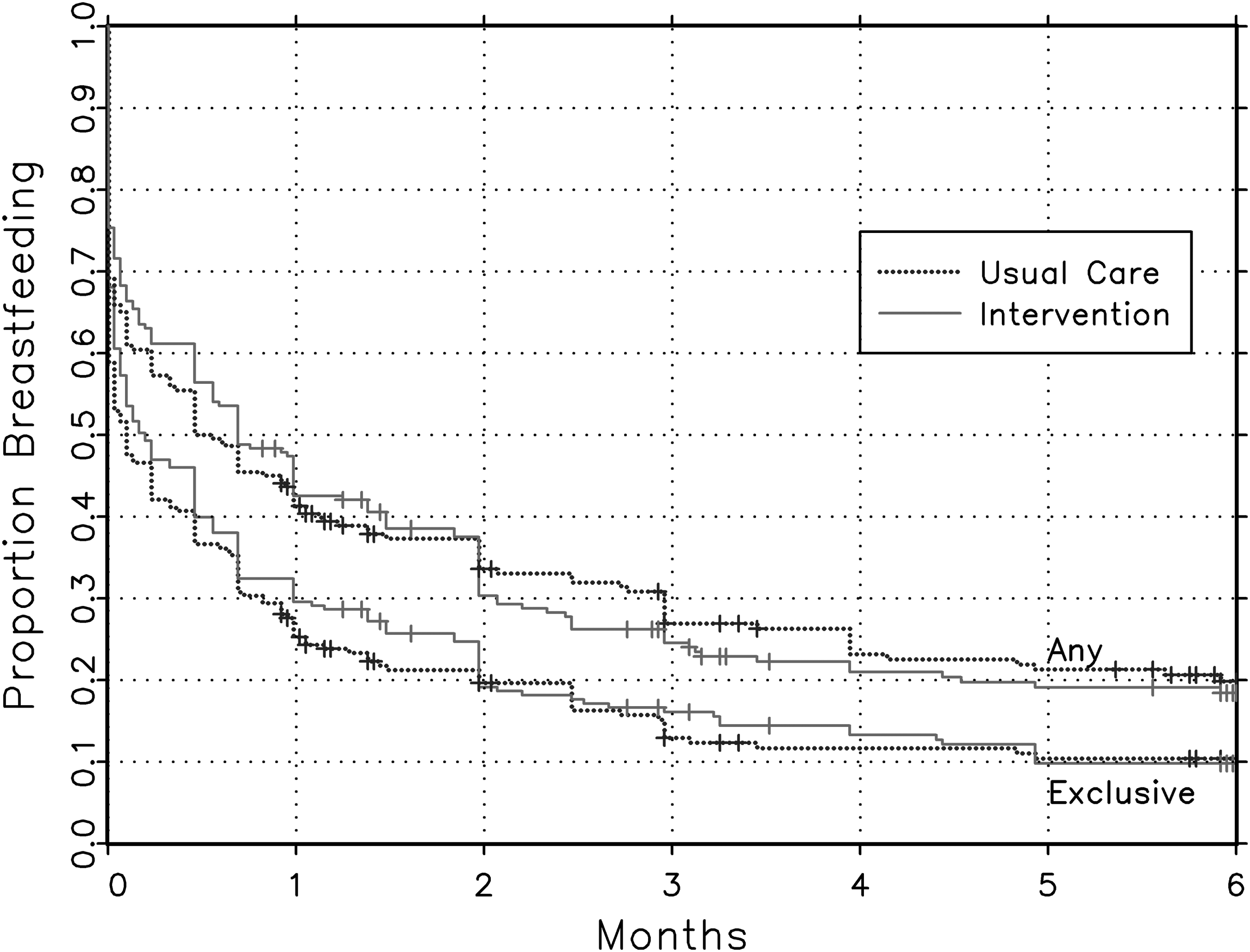
Prenatal education video study duration of exclusive and any breastfeeding by intervention group. Any: p = 0.99, HR (intervention to usual care) = 1.00, 95% CI: 0.81–1.24. Exclusive: p = 0.50, HR = 0.93, 95% CI: 0.76–1.14. CI, confidence interval; HR, hazard ratio.
When stratified by previous breastfeeding experience, there were still no significant differences in duration between the intervention groups (Fig. 2). Over the 6-month follow-up period, women with previous experience breastfeeding for more than 6 months had the highest rates of breastfeeding, followed by women with previous experience breastfeeding less than 6 months, then primiparous women, and finally multiparous women with no previous experience breastfeeding (Fig. 2A–D). Of these subgroups, multiparous women with no previous experience breastfeeding were the only ones among whom a greater proportion of the intervention group breastfed compared with the control group over the 6-month follow-up period; however, the difference was not significant (Fig. 2B).
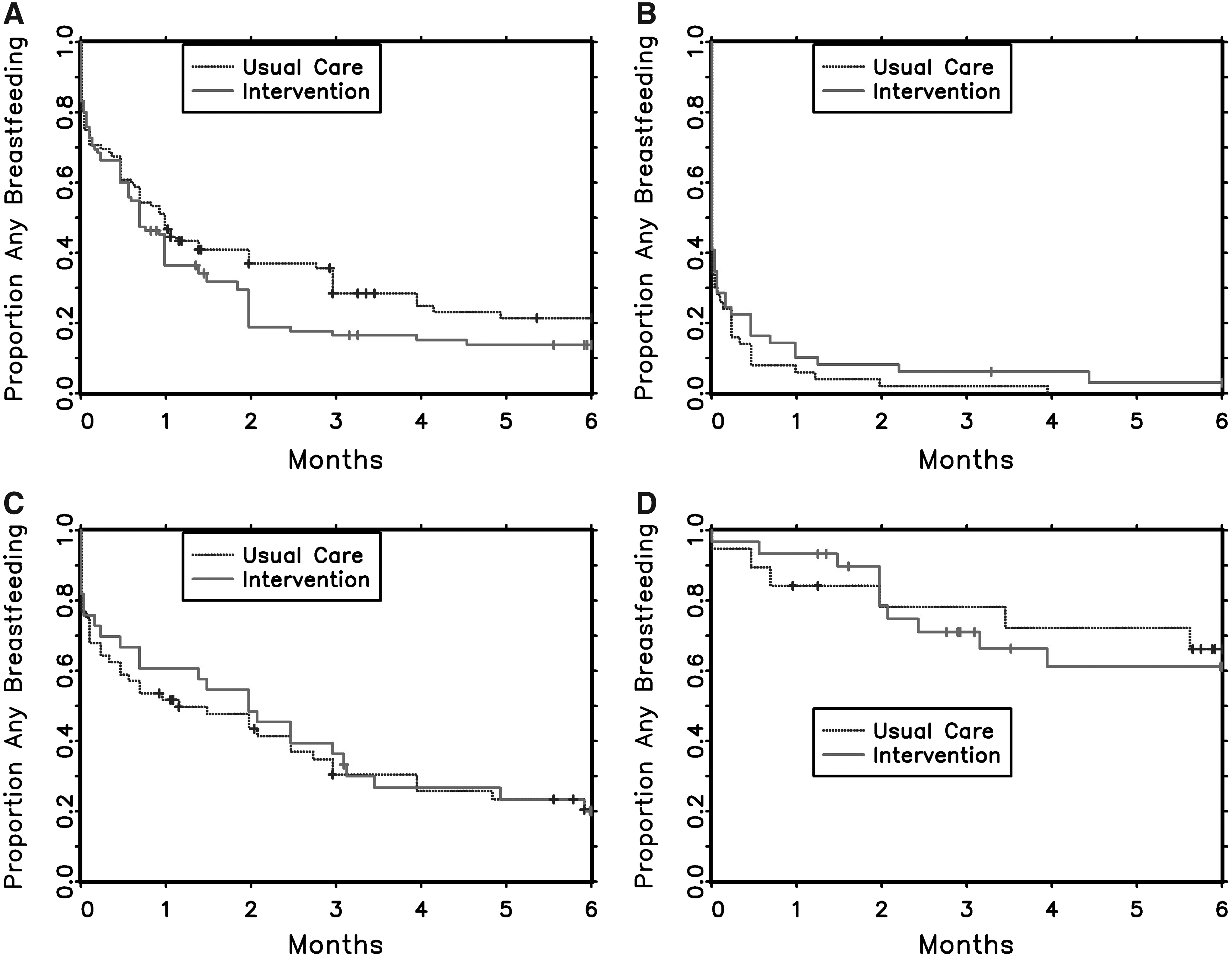
Prenatal Education Video Study Duration of any breastfeeding by previous breastfeeding experience.
Subgroup analyses based on the participants' infant feeding intentions were also performed. Among those who intended to feed breast milk exclusively in the first 6 months versus breast milk in combination with artificial breast milk substitute, neither duration of any nor exclusive breastfeeding differed by intervention group (Fig. 3). Women who planned to feed both breast milk and artificial breast milk substitute had a more precipitous decline in both any and exclusive breastfeeding during the first month compared with women who planned to feed breast milk exclusively (Fig. 3B versus A, D versus C). Women who intended to feed only breast milk had higher rates of breastfeeding at 6 months than those planning also to feed artificial breast milk substitute (Fig. 3A, C). Among women intending to feed only breast milk, those assigned to the intervention had slightly higher breastfeeding rates at most of the time points, although these differences were not significant (Fig. 3A, C).
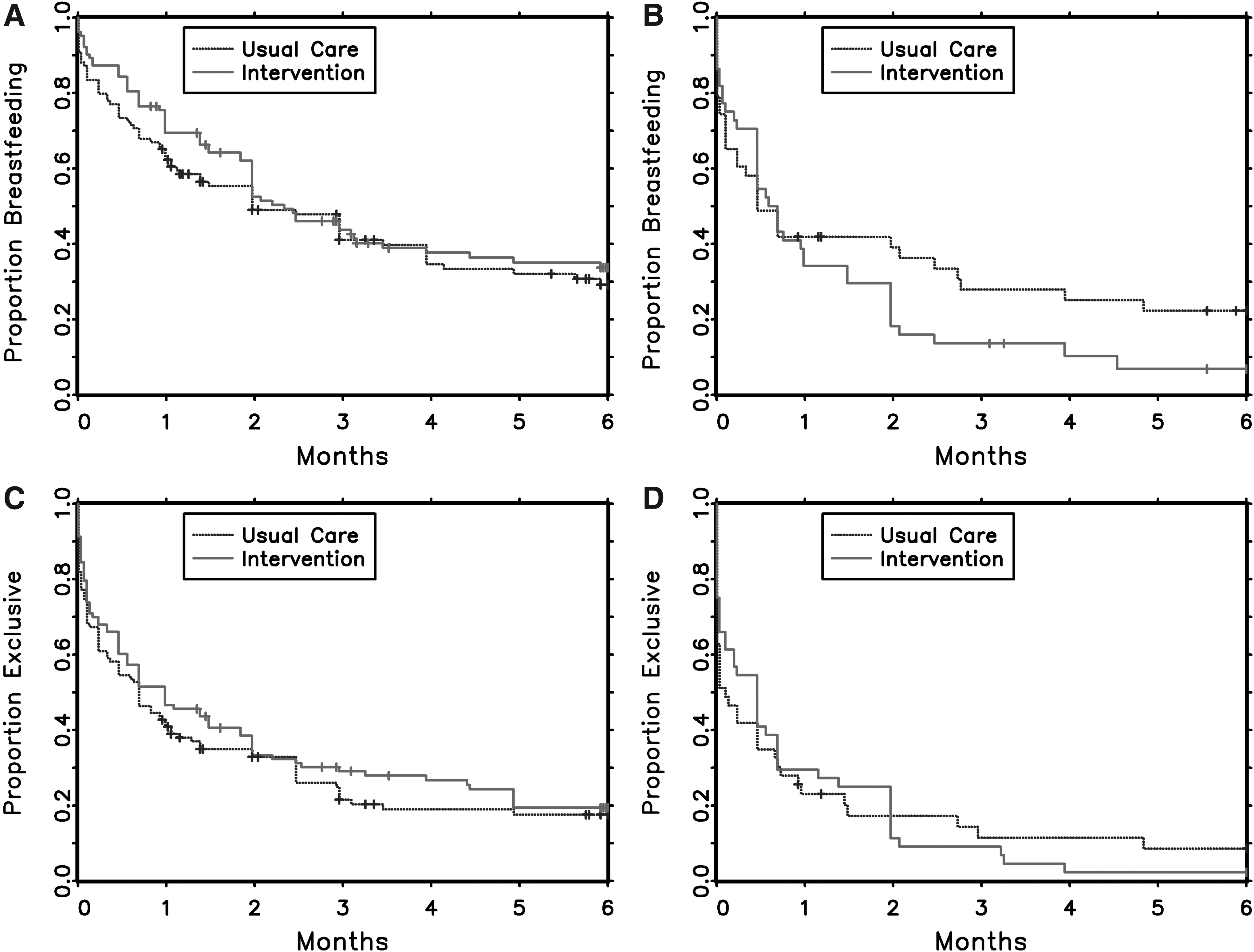
Prenatal Education Video Study Duration of any and exclusive breastfeeding by intended infant feeding method.
Discussion
This study examined the impact of a low-cost, easy-to-implement strategy to increase breastfeeding, but found that use of an educational video alone in the third trimester did not prolong the duration of any or exclusive breastfeeding during the first 6 months postpartum. Not surprisingly, patterns of breastfeeding in subgroups indicated that women with previous successful experience or the intention to exclusively breastfeed were more likely to breastfeed. Viewing the educational video did not significantly impact these associations. Two observations may be of note, however; the intervention group had higher rates of exclusive breastfeeding than the control group at most time points among multiparous women with no prior breastfeeding experience and among women who intended to exclusively breastfeed, although these differences were not significant.
These results differ from those of a previous study that compared breastfeeding among three groups of women: those who viewed the same educational video, those who were given two sessions of postnatal lactation support, and those who received usual care. 21 In the previous study, both intervention groups had higher breastfeeding rates than the control group at multiple time points up to 6 months. However, both printed information on breastfeeding was provided to study participants as well as consultation with a lactation counselor for 15 minutes in this previous study. Counseling by a lactation consultant has been shown to increase breastfeeding exclusivity and duration. 12 Thus, the impact of the video in this previous study could have been enhanced by the additional information and/or counseling. That population also differed in substantial ways from the current study population, including lower initial breastfeeding rates among the previous study population.
Other potential reasons for the lack of impact of the video include that, while information conveyed by video can be effective, it is not individualized or personalized like that of other educational approaches, such as motivational interviewing or face-to-face interaction. In addition, knowledge alone does not predict a woman's ability to meet her own breastfeeding goals; other important factors include perceived cultural norms, availability of maternity leave, and presence of supportive partners or other family members, such as grandmothers. 24 Finally, and perhaps most importantly, multiple interventions are likely to be more effective than a single intervention.25–27 For example, prenatal breastfeeding education may prove more effective when combined with evidence-based hospital best practices. At the time of the study, neither of the birth hospitals were Baby Friendly. 28
Among women intending to feed only breast milk, those assigned to the intervention had slightly higher breastfeeding rates at most of the time points, although these differences were not significant. This finding supports the idea that women enter pregnancy having made a decision about how to feed their infant, and educational interventions may serve to further cement or encourage that decision. Prenatal intent is one of the strongest predictors of exclusive breastfeeding.11,29 Advice from a health care provider to breastfeed has a positive impact on breastfeeding rates, 30 and while the educational video was shown in the prenatal clinic, it did not involve a face-to-face interaction about breastfeeding with a health care provider. In keeping with past studies, these results show that the plan to use any artificial breast milk substitute was related to early cessation,5,31,32 and rates of breastfeeding declined as artificial breast milk substitute was introduced. Perhaps health care providers' advice to breastfeed helps women commit to the intent to breastfeed, which in turn helps them achieve their goal.
Although this study has several strengths, including random assignment of the intervention and longitudinal data collection of feeding data from multiple sources, it also has several important limitations. The participation rate was only 64%, and participants may have differed from nonparticipants. However, loss to follow-up was low and did not differ significantly by intervention group. This study relied on self-reported breastfeeding, which may be overreported due to social desirability. The generalizability of the findings is limited. Due to resource constraints, Spanish-speaking women were excluded from this study, and Latina women have higher rates of breastfeeding, than other racial/ethnic groups. 4 The study population was also restricted to women with low income. Thus, these findings may not be generalizable to women of other socioeconomic groups. Finally, the intervention was delivered during the third trimester of pregnancy. This approach was taken for a number of reasons, including maximizing the likelihood of a viable pregnancy; not systematically excluding women who initiated prenatal care later in pregnancy, eliminating the possible differential effects of early versus late viewing; and decreasing the time from enrollment to delivery to minimize loss to follow-up. However, studies, including the present study, show that women make feeding decisions earlier in pregnancy or even before pregnancy. Thus, the intervention may have had an impact had it been delivered in the first or second trimester.
Although little impact of the educational video on breastfeeding was found, these results underscore two important points. First, a history of previously breastfeeding a child for at least 6 months is associated with future successful breastfeeding. Encouraging women who intend to breastfeed to strive for at least 6 months and helping them to achieve their duration goal will likely impact their breastfeeding duration in future pregnancies. Second, intending to breastfeed exclusively during pregnancy is associated with higher rates of any and exclusive breastfeeding. This highlights the importance of providing each woman with accurate information early, when she makes her feeding decision. Given the important role of both a woman's previous breastfeeding experience and her intended feeding plan, it seems clear that educational and other interventions need to occur as early in the reproductive process as possible. Educating and supporting individual women can then be combined with community and health policy interventions, such as paid maternity leave and improved workplace and community support, to have the greatest impact on increasing breastfeeding duration and exclusivity.
Conclusion
Showing a breastfeeding education video in the prenatal clinic to pregnant women in the third trimester did not impact breastfeeding duration or exclusivity among low-income women in this study. Even among women intending to breastfeed, there are barriers to meeting personal feeding goals that may require multifaceted interventions. Educational videos may be useful as one component of a comprehensive program to promote breastfeeding. Future research should assess use of videos in combination with evidence-based interventions at the hospital, workplace, and community levels; the impact of introducing breastfeeding education early in pregnancy and/or preconceptually; and the development of effective interventions to help those that desire to breastfeed achieve their goals.
Footnotes
Acknowledgments
The authors would like to acknowledge the contributions of Gauri Gulati, MD, and Valerie Coleman, RN, MSN, at Virginia Commonwealth University. This study was funded by the Virginia Department of Health.
Disclosure Statement
No competing financial interests exist.