
Abstract
Abstract
Breastfeeding rates in the United States continue to rise, but still fall short of goals for both initiation and continuation. Many different maternal demographic characteristics have been identified as risk factors for not breastfeeding, but the literature remains inconsistent. National and even state-level data may not reflect patterns seen at the local level. Clinicians and breastfeeding advocates should be aware of the general trends, but should more importantly become familiar with the predominant risk patterns in their local area and populations. This presentation for the Breastfeeding Summit reports on our findings regarding the influence of race and economic status on breastfeeding behavior among women in inner city Philadelphia, and makes a case for advocates and clinicians to explore these trends in their own, local populations.
Introduction
B
Many maternal characteristics seem to be associated with lower rates of breastfeeding.5,6 National-level survey data show that breastfeeding initiation and continuation vary by race; black women are significantly less likely to initiate breastfeeding, and significantly less likely to be exclusively breastfeeding at 6 months. Socioeconomic status (SES) has also been shown, in national data, to associate with lower rates of breastfeeding.7,8 However, the relationships among breastfeeding, race, and SES are far from settled. While the aggregate data captured in such surveys as the National Survey on Children's Health or the National Immunization Survey seem to show clear trends, other smaller and locally focused studies often find conflicting and differing patterns. For example, a recent study from the National Survey of Family Growth showed the income was not a factor in breastfeeding behavior, 9 and a large study among California women found that SES had little impact compared to education level and race. 10 Similar conflicting results have been seen regarding race as well. While African American women are reported to have lower rates of breastfeeding when compared with white or Latina women,8,11,12 some studies have found that specific populations of African American women are more likely to breastfeed than other groups. 13 Breastfeeding rates and behavior by income or race differ between urban and rural settings,14–16 and one study of urban women found that African American women were more likely to intend to breastfeed than non-Hispanic white women. 17
The interaction of race and SES in health behaviors is complex and likely varies in different environments, such as urban, inner city, or rural areas. The United States has a long and persistent history of racial segregation and, in recent decades, a widening economic divide between the upper and lower classes. In addition, we are a large country encompassing a dizzying spectrum of cultures and environments. While it is easy to speak of categories such as “Black Women” and “White Women” and “High Income” or “Low Income” in broad strokes, the lived experience of those wearing such labels is likely very different in different U.S. environments—North, South, urban, and rural. Given this, it is essential to remember that while large data are useful for gaining a big-picture perspective, it frequently does not reflect the experience of any specific population. While smaller studies may lack generalizability and suffer methodologic flaws, they serve an essential function of deeply investigating what is happening in a particular region or population. Understanding the prevalence of breastfeeding and accurately identifying true risk factors for early discontinuation in a particular population may require a focus on that given population. This presentation to the Breastfeeding Summit makes a case for individual researchers and advocates to consider a local focus in breastfeeding research and intervention design. We use the city of Philadelphia as an example of the use of regional statistics to explore local patterns and describe a recent research project to illustrate the usefulness of hyperlocal data in understanding breastfeeding in any specific population.
In considering breastfeeding at the state-level data from Pennsylvania, vital statistics paints a picture of breastfeeding trends that is similar to the national data. In 2016, breastfeeding initiation rates were 91% among Asian/Pacific Islanders; 82% for white women; 80% for Hispanic women, and 75% for black women. 18 However, when broken down by county, striking variation is seen across the state–overall breast feeding rates vary from a low of 54.4% in Green County in the southwest corner of the state to a high of 93.5% in the Sullivan County in the Northeast region. 19 This is a strong indicator that specific areas of the state may not follow the trends that the state-level data suggest.
Pennsylvania is a large and diverse state. There are two large urban areas, one located in the west (Pittsburgh) and one in the east (Philadelphia). The central portion of the state is largely rural, dotted with several smaller urban and suburban centers. Given the diversity encompassed in the state, it is not surprising that breastfeeding practices may be divergent across the region. Patterns and influences may not be the same in the central rural portion of the state as in the coastal urban area. A clinician specifically serving the urban population of Philadelphia, who wants to understand breastfeeding in Philadelphia, should perhaps focus on the city itself.
Being a large city with several academic centers, it is unsurprising to find that several small studies have examined breastfeeding patterns among Philadelphia women. These studies have reported findings that seem to be at odds with the typical patterns that the larger data suggested; a study at a single north Philadelphia academic hospital found that breastfeeding initiation did not differ by race. 20 Studies of patients receiving care through the publicly funded Health District clinic system likewise found that the low-income black women were more likely to intend to breastfeed than white women, 17 and that actual breastfeeding initiation and continuation did not differ by race. 21 This suggests that while clear patterns by race may be seen at the state level, it may not hold as much influence in the local area–other demographic and SES factors may be more significant.
Philadelphia is a densely settled vibrant city. With a population of 1.5 million, it is the fifth largest city in the United States and the second largest city on the eastern coast. It is also designated as the poorest of the 10 largest cities in the United States. The poverty rate is about 26% (third highest in the nation), with 12% of the population living in deep poverty. The median household income is about $41,000, and about 9% of the population is uninsured. 22 While the suburbs surrounding the city are affluent, within the city limits, large areas of the city have a median household income of less than $35,000; only a few focal pockets have median incomes greater than $63,000.
Philadelphia also has the dubious distinction of being a “hyper-segregated” city. This designation is given to a city that meets four of the following five criteria: (1) black residents are “unevenly distributed,” geographically; (2) black residents are isolated—they predominantly live in African American neighborhoods; (3) these neighborhoods are clustered together; (4) the black population is highly concentrated in these small, geographically compact areas; and (5) these residents tend to live in the urban cores of the city. 23 Maps utilizing census data help to visualize these patterns and demonstrate Philadelphia's segregation. Swaths of the eastern portion of the city are 70–80% white, while west and north-central Philadelphia are 60–90% black.
The Pennsylvania Department of Health produces detailed information on breastfeeding initiation, complied from city-wide hospital discharge data. When broken down by census tract, one sees wide variation in breast feeding initiation rates across the city, from a low of 59.2% to a high of 92.2%. This is a striking range for a densely populated city that covers only 141 square miles. Comparison of the breastfeeding maps to the maps of racial and economic distribution suggests some correlates, but no strikingly clear pattern. Conventional wisdom says to expect low rates of breastfeeding in predominantly black and predominantly low-income areas. But while the majority white areas of the city do encompass those areas with the highest breastfeeding rates, they also have some of the lowest, particularly in the north-east. A similar pattern is seen in the majority-black areas–a mix of high and low rates. If we look at income distribution, we see suggestions of a slightly stronger correlation, with lower rates in the lower-income areas–but some of the low-income areas in west Philadelphia are actually doing quite well.
This suggests that to understand which demographic characteristics are associated with nonbreastfeeding among the women of Philadelphia, we should look at both racial and economic factors—both these factors are in play and likely interact. To investigate this, we performed a research study using postpartum clinic data from our hospital, Thomas Jefferson University Hospital in Center City Philadelphia. We wished to examine the relationship between SES and early discontinuation of breastfeeding in our typical urban population, using markers and classifications that are readily available in the clinical care setting. We performed a retrospective cohort study to examine continuation of breastfeeding in women receiving either Medicaid or commercial insurance at 6 to 8 weeks postpartum in a mixed-race, economically diverse urban population.
The full study has been published previously. 24 In brief, this retrospective chart review assessed breastfeeding among women who delivered infants at Thomas Jefferson University hospital between July 1st 2013 and December 15th 2013. Women who delivered live-born, term, singleton infants in the study period were identified from the labor and delivery records, and outpatient records were queried and women who completed an office visit between 6 and 8 weeks postpartum were identified and included in the study.
Outpatient electronic medical records were abstracted to determine breastfeeding status at the time of the outpatient visit. Our primary outcome was defined as a three category description of breastfeeding: no breastfeeding (bottle/formula only), any breastfeeding (breast only or breast and bottle/formula), or exclusive breastfeeding (breast only). Our primary exposure variable was the patient insurance status in the pregnancy. This was defined as a dichotomous categorical variable of Medicaid) or commercial insurance. Race was also examined as an exposure variable.
We found that a total of 656 women delivered term, singleton infants at our hospital in the study timeframe. Of these, 405 (61%) completed a standard postpartum follow-up visit in the typical timeframe of 6 to 8 weeks. All patients had documentation of their feeding method in the medical record. Forty-seven percent of patients were Medicaid-insured, and 53% were African American. Women with Medicaid insurance were younger, more likely to be of African American race, more likely to be primiparous, and less likely to be married or have attended college. Overall, 239 women (59%) were performing any breastfeeding, and 166 (40%) were exclusively breastfeeding at the time of the postpartum visit. While black women were less likely to breastfeed in absolute numbers, after adjusting for confounding, statistical significance in this relationship was lost (Table 1). In considering insurance status, Medicaid-insured patients were significantly less likely to be performing either any breastfeeding or exclusive breastfeeding than commercially insured patients, and this relationship remained significant even after adjusting for confounding (Table 2). Change in effect modeling and partial-F testing showed that of these factors, race was the patient characteristic that most significantly affected the relationship between breastfeeding and insurance status, and that there was significant interaction effect between race and breastfeeding.
Adjusted for age, insurance, parity, education, and marital status.
Adjusted for age, race, parity, education, and marital status.
To explore the effect of interaction between race and insurance status, a stratified analysis was performed to estimate the proportions of breastfeeding women in each race and ethnicity group, in each insurance category. The probability of any or exclusive breastfeeding was highly variable between the insurance categories and race/ethnic groups. The interaction was statistically significant across all categories, even when adjusted for other potential confounders. (p < 0.01) (Figs. 1 and 2). Overall, the highest rates of exclusive breastfeeding were seen among commercially insured white women, and the highest rates of any breastfeeding were seen in commercially insured Asian women. While African American women overall had the lowest rates of breastfeeding (52% any; 33% exclusive), these women had only a moderate difference in either breastfeeding category between the insurance groups. In contrast, white women overall were more likely to breastfeed (64% any; 55% exclusive), but white women on Medicaid had the lowest rates of breastfeeding of all race and ethnicity groups, and the largest differential by insurance was seen among white women. Only 24% and 22% of white women on Medicaid performed any or exclusive breastfeeding, respectively, while 76% and 64% of white women with commercial insurance were performing any or exclusive breastfeeding.

Race, Insurance, and Any Breastfeeding. Proportion of women performing any breastfeeding differs by insurance status across race/ethnic categories. *Statistically significant difference in probability of breastfeeding between insurance categories, across multiple race/ethnic groups.
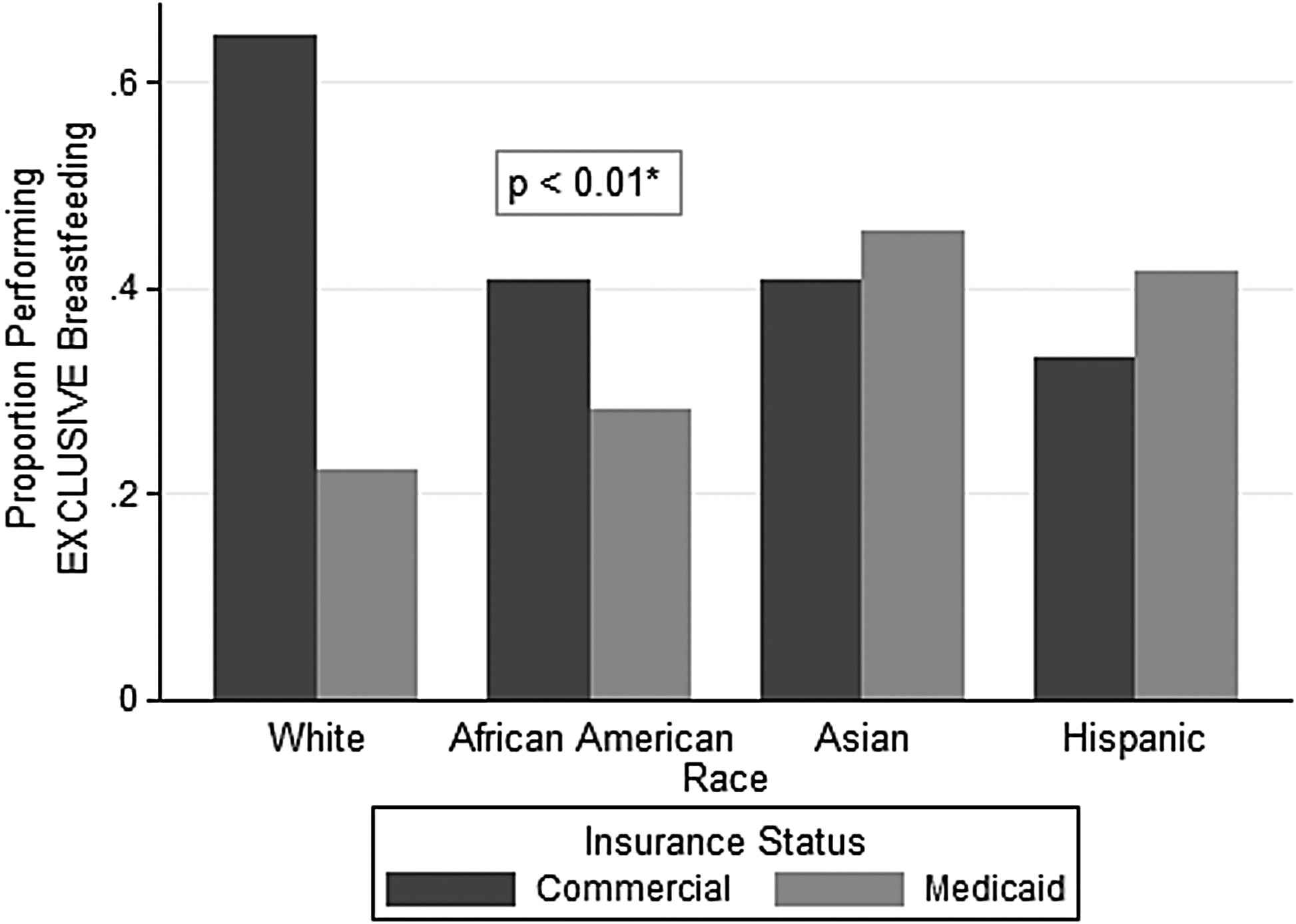
Race, Insurance, and Exclusive Breastfeeding. Proportion of women performing exclusive breastfeeding differs by insurance status across race/ethnic categories. *Statistically significant difference in probability of breastfeeding between insurance categories, across multiple race/ethnic groups.
In sum, we found that in our population, rates of both any and exclusive breastfeeding were significantly lower within the Medicaid population when compared with a commercially insured population, even when controlling for other factors that have been shown to correlate with breastfeeding. This finding is consistent with prior studies showing that women of lower SES are less likely to both initiate and continue breastfeeding, confirming that this pattern is found specifically in the urban setting. Our study expands on this by finding significant difference in breastfeeding in stratified analysis combining insurance status and race. Among Philadelphia women, African American women overall were the least likely to breastfeed, which is consistent with previous literature. However, our stratified analysis demonstrated significant interaction between race and insurance status, finding that white women on Medicaid are actually the least likely of all groups to breastfeed, either at all, or exclusively. Our finding suggests that in this urban population, the strongest risk factor for not breastfeeding is insurance status rather than race and that within the subset of women receiving Medicaid, non-Hispanic white women are the highest risk.
Our study certainly has limitations, and limited generalizability. By including only women who presented for their scheduled postpartum follow-up, we lack data on about 40% of our population,. We also use Medicaid status as a proxy for SES, which may not truly correlated with income. However, this study was undertaken in a time period before the major Medicaid expansion, and anyone on a Medicaid plan would have had an income level not greater than 134% of the Federal Poverty Level, so we can confidently assume that this group is of low SES. In addition, we consider the use of Medicaid status to be a clinically useful predictor. While clinicians do not routinely collect household income information from patients, we do always know their insurance status. The ready availability of this information makes it a feasible tool in assessing a patient's breastfeeding risk.
Regarding generalizability of the findings to other populations–this is a consideration that is central to our effort in this presentation and publication. We were alerted to consider these relationships through exploration of our own local statistics and population. While our findings may be replicable in other similar settings (urban, northeastern, mixed race, but internally segregated cities), we do not expect that these exact patterns to be found in other populations. What we have discovered is that looking carefully at our particular population allowed us to identify patterns in breastfeeding risk factors that differ in subtle but essential ways from what large-scale data suggest. This intimate knowledge of breastfeeding patterns in our specific population helps us understand which are the highest risk groups for noninitiation and early discontinuation of breastfeeding among the women we care for every day.
Much effort is being placed into supporting and encouraging breastfeeding for all women. Several federally funded programs provide support to hospitals to improve maternity care and breastfeeding support; these programs are focused on reducing racial and ethnic disparities in breastfeeding and specifically target low-income and minority populations. Clinical practice should encourage all women in breastfeeding, but effective interventions to improve outcomes need to accurately identify those who are most in need of education and support. Our study demonstrates that in simply considering racial and ethnic characteristics, interventions may miss more complex patterns and women who are at highest risk. In Philadelphia, if one is aware that 65% of white women are breastfeeding, but not that only 22% of white women on Medicaid are, it is easy to overlook this subpopulation and misclassify them as “low risk,” simply based on race. In another environment, there may be different, easily overlooked populations at risk.
In sum, in our work to promote, support, and increase breastfeeding, it is essential to understand the specific population in which one is working. When possible, breastfeeding advocates should consider performing locally focused research to explore these relationships in their specific populations more explicitly. A better understanding of the reasons for these disparities and what influences breastfeeding in local populations groups may allow for more effective interventions to increase breastfeeding rates in each specific high-risk populations.
Footnotes
Disclosure Statement
No competing financial interests exist.