
Abstract
Abstract
Background:
Breastfeeding is known to be the best source of nutrition for infants. The World Health Organization recommends to exclusively breastfeed up to the sixth month of life and to breastfeed with complementary foods until the age of 2. It is reported that maternity leave (ML) is one of the most important interventions for an extended breastfeeding duration. The aim of this review is to synthesize the available data worldwide on the association of ML and breastfeeding duration. We also intend to provide an overview of whether this association is differential by socioeconomic status.
Materials and Methods:
Relevant primary studies relating ML and breastfeeding were included by searching several databases, including PubMed, SCielo, Health Systems Evidence, Health Evidence, Cochrane Reviews, and Epistemonikos. Articles were included up to May 2018.
Results:
A total of 239 relevant articles were identified, of them 21 were included in the review based on exposure, outcome, and study design. These studies reported that an extended ML might be related to breastfeeding duration. In addition, studies reporting data on work type, race, and education showed that black women, women in less privileged position, and women with less education have less breastfeeding duration.
Conclusions:
This review showed a positive relationship between ML length and breastfeeding duration. These results have a homogeneous trend; however, this was different when studies reported results on ML and breastfeeding stratified by socioeconomic status. Public health policies should ensure that all women, especially the most vulnerable, have equal access to the benefits that ML provides.
Introduction
B
To accomplish a successful breastfeeding, governments should promote policies that ensure that all mothers are empowered and supported to follow optimal infant breastfeeding practices. Successful and comprehensive breastfeeding strategies should include high-quality programs that encourage all women who want and can breastfeed, understanding that breastfeeding is always an investment for society and a key part in many of the United Nations' Sustainable Development Goals 2030.8,10,11
According to 2016's Lancet series on breastfeeding,2,8,12 until now, there is no country that has fully implemented these measures in breastfeeding strategies. These recommendations are based on comprehensive strategies at the government, community, and individual levels, targeting pregnant women and new mothers. Examples of these kinds of strategies and interventions are counseling and education, Baby-Friendly Hospital Initiative, cash transfers, maternity leave (ML), national-level pro-breastfeeding campaigns, among others.8,10
ML and maternity protection strategies are among the interventions described as successful in breastfeeding promotion.8,10,13 According to the International Labor Organization (ILO), ML is defined as one part of what is recognized as the legislative provisions of maternity protection, which includes ML, benefits, employment protection, health protection, breastfeeding arrangements at work, and childcare. 14 Nonetheless, only recently the ILO advocated for maternity benefits to be delivered as part of the minimum basic social security guarantees for working women who want to breastfeed their children.
There is inconsistent and scarce information from previous studies regarding the relationship between ML and breastfeeding duration, especially among different socioeconomic levels and developing countries. Some studies are consistent in reporting the association between ML and breastfeeding. For example, Hawkins et al. 15 found that women who had not returned to work by 6 months after birth had a higher prevalence of exclusive breastfeeding, but other studies showed mixed results. 16 In this review of peer-reviewed studies, we aim to summarize and accumulate more evidence relating ML and breastfeeding duration. We intend to provide a narrative overview of the available evidence by clarifying whether there is an association between ML length and breastfeeding duration and whether this association is the same across all socioeconomic strata.
Materials and Methods
Search strategy
Initially, relevant articles relating ML and breastfeeding were identified by searching several databases, including PubMed, SCielo, Health Systems Evidence, Health Evidence, Cochrane Reviews, 17 and the newly created Epistemonikos. 18 Articles were searched up to May 2018. We had no year limit for this review.
Research question
The search looked for already published peer-reviewed articles that answered the research question and included data on exposure and outcome.
We followed the PICO (population, intervention, comparison, outcome) approach to orientate our research question, where:
Population: working women Intervention: ML duration Comparison: no ML Outcome: any breastfeeding duration
And the research question was: Is ML effective in promoting breastfeeding in working women equally according to socioeconomic status?
To address this question, the search strategy included articles with the keywords included in Table 1.
Study selection
This review includes peer-reviewed articles with any of the following study designs: randomized trial, cohort, case–control, cross-sectional studies. Only studies that analyzed individual-level data were included. Articles assessing any type of modeling analysis or ecological study design were excluded.
Articles were included if the outcome was: exclusive breastfeeding duration/exclusive breastfeeding/exclusive “yes or no”, and the exposure was ML (paid and unpaid). We included studies written in English, Portuguese, and Spanish. Articles were also included if the methods section defined clear selection criteria, assessed the effects of ML on breastfeeding duration, and reported exclusive or any breastfeeding duration as the outcome. Studies that reported formula use as an outcome were also excluded.
Articles were first screened for title and abstract. Full text was screened if an article seemed relevant for inclusion.
Data extraction
The extraction of relevant data was performed by the author D.N.R. A summary table was prepared with the following data: first author's last name, year of publication, country where the study was conducted, sample size, sample description, study design, exposure description, outcome description, summary of results, and if the study included information stratified by socioeconomic status. Information on ML length and breastfeeding duration was included for many relevant subgroups. All data on breastfeeding and ML related to socioeconomic status or wealth were extracted, regardless of the type of analysis used.
Results
The search for this study yielded 239 articles, of which 216 were excluded based on title and abstract appraisal because they were written in a language other than English, Spanish, or Portuguese, or because they did not address the research question (Fig. 1). A total of 56 articles were screened for full-text review. Of these, access to full text was unavailable for 7 articles. Twenty-eight articles were excluded because the exposure or outcome was not relevant to the research question. Twenty-one articles were retained in the final review. Twelve of the included studies were located in the United States, Australia, or Europe (United Kingdom, Ireland, Spain), three in Asia (Israel, Jordan, and Turkey), three in South America (Brazil), two in South East Asia (Thailand and Myanmar), and one in Africa (Ghana). Eleven of the included studies had a cohort study design. All studies together counted for a total of 57,804 women.
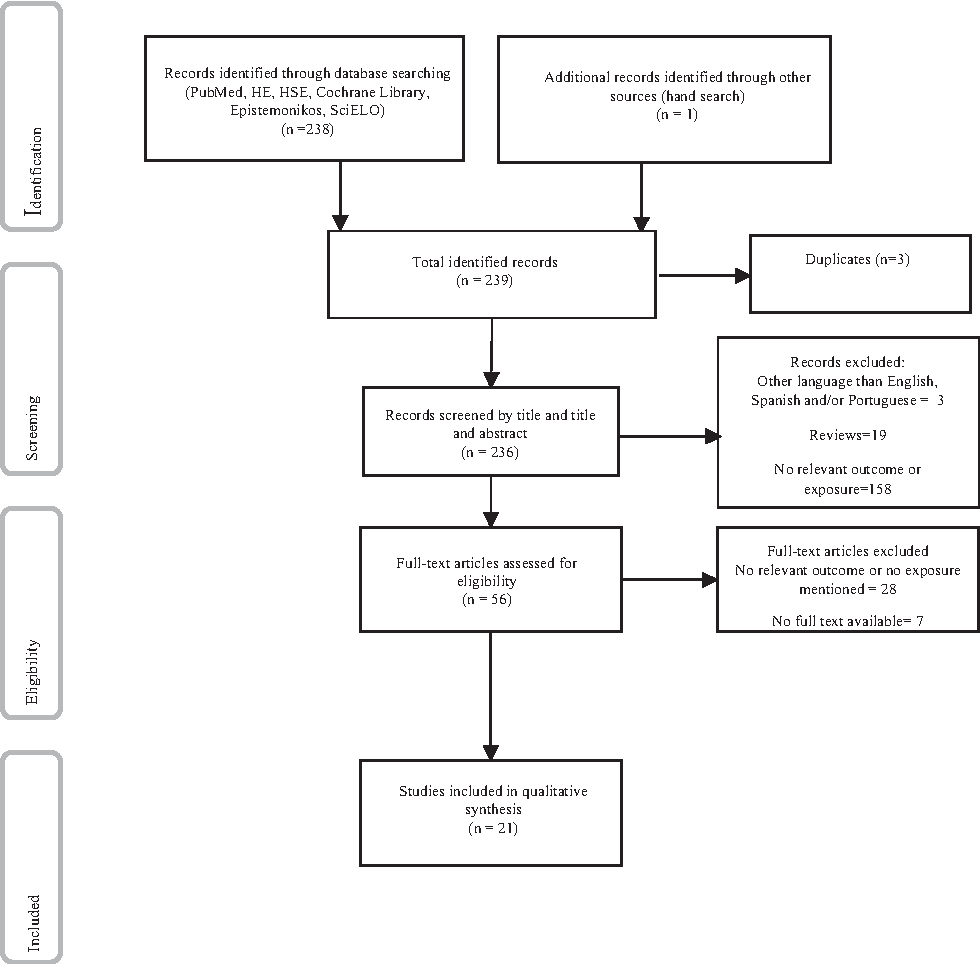
Flowchart of study search and selection.
The 21 studies included in this review referred to ML and breastfeeding duration (Table 2). Camurdan et al. 19 and Khasawneh and Khasawneh 20 describe ML time using days, Hmone et al. 21 and Monteiro et al. 22 provide a description of ML as working women versus not working women, while the rest of the studies that were included reported ML in weeks or months. The majority of studies included in this review outlined a ML of 12 weeks (3 months) or more. Breastfeeding was defined as exclusive in 5 studies, any breastfeeding (5 studies), predominant breastfeeding (2 studies), or total breastfeeding (exclusive) and any breastfeeding (16 studies). All the studies in this review defined the outcome as at least 3 months of breastfeeding.
AOR, adjusted odds ratio; BF, breastfeeding; CI, confidence interval; EBF, exclusively breastfed; HR, hazards ratio; ML, maternity leave; PR, prevalence ratio.
Most of the 21 studies (20 studies) showed that having a longer ML was a protective factor for breastfeeding duration.15,16,19–37 Studies that reported ML of more than 3 months had overall three times the likelihood of maintaining breastfeeding at 3 months after birth compared to returning to work within 3 months after birth. Women who had ML of 6 months were 50% more likely to maintain their breastfeeding until the sixth month after birth. In contrast, women who had to return to work before the third month after delivery showed, on average, between a 20% and 40% more likelihood of discontinuing breastfeeding; however, this did not seem to be significant in all studies.
Qualitative data described in one study carried out in Myanmar 21 reported that work was the main barrier for breastfeeding duration in working women, especially in the private sector where women have a contract. A study from Jordan 20 reported that 65% of working women stopped breastfeeding upon returning to work.
The results in a cohort study of 2,079 women in Scotland found that a ML of 6–10 months did not yield a statistically significant result on breastfeeding duration (hazards ratio, 1.00 [95% confidence interval (CI), 0.75–1.32]). 34
This review found little evidence from studies presenting additional stratified analysis by socioeconomic status15,21,25,28,36 (Table 2). Most studies were stratified by work type, education, and race as socioeconomic status proxies. Only one of these studies was carried out in a developing country 21 ; the rest were performed in the United States and the United Kingdom. These studies showed that, on average, women who had high-profile jobs showed a greater likelihood of maintaining their breastfeeding for more extended periods. In addition, women working in managerial positions, versus other types of jobs, were also more likely to continue their breastfeeding for a longer time, showing that managerial roles might be a protective factor for breastfeeding (odds ratio [OR], 0.63; 95% CI, 0.41–0.96). 28
Another example is the research performed by Visness and Kennedy, 36 which also observed that job status might influence breastfeeding duration. Professional white women had a higher percentage of breastfeeding after returning to work (64%) compared to white women working in technical, administrative, or sales jobs (47%), white women working in services (48%), and white women employed in manufacturing (38%).
Visness and Kennedy 36 also included data on Afro-American women. These results showed that race was also an important factor for early breastfeeding cessation after returning to work (white women 53% vs. Afro-American women 43%). Afro-American women did not show a gradient of association between work position and breastfeeding duration, compared to white women.
Data on education and breastfeeding showed that women with college studies, who returned to work before 6 months after delivery, were more likely to continue breastfeeding (OR, 0.66; 95% CI, 0.47–0.93), compared to women without college education. 36
Discussion
To our knowledge, this review is one of the few pieces of literature that includes data on the impact of ML and breastfeeding duration from six continents. In addition, we also reviewed whether the association differs by socioeconomic status.
Most of the studies selected in this review reported that there is a positive association between ML and breastfeeding duration. This review found that women with a ML of 3 months presented at least 50% more likelihood to extend breastfeeding duration as compared to women who returned to work before this time. Women who had 6 months or more of ML showed at least 30% likelihood of maintaining their breastfeeding for at least the first 6 months.
Other reviews that analyzed the association between ML and breastfeeding duration are consistent with the findings of this study.13,38,39 Returning to work is described as the main reason for an early breastfeeding cessation.25,40,41 Hence, the reasons for a positive link shown between an extended ML and breastfeeding could be related to ML providing more time for women to bond with their babies, and encouraging ad libitum breastfeeding.40–42 Moreover, ML could be associated with having more time at home, away from work, recovering from the physical stress of childbirth, and focusing on the infant.
The few studies that reported data on ML and breastfeeding stratified by job position, education, and race as proxies of socioeconomic status showed that returning to work shortly after birth is related to an early breastfeeding cessation. In addition, in one study, 36 job status results revealed that women in more privileged working roles had higher rates of breastfeeding at 6 months after returning to work. The reasons for this relationship could be that women in low-profile jobs have less flexibility for breastfeeding, get less work support such as nursery and lactation rooms, need to work extra hours, receive less family support, together with having less knowledge of the importance of breastfeeding. These results might also be linked with having shorter commutes and less stress triggered by work.43–45
Although this review includes a large number of cases, the comparability among studies is limited, due to the differences between sample characteristics, study design, analysis, and the metrics of exposure and outcome.
Several limitations of this study are worth considering. This review is limited by the available articles and the included ones, written in English, Spanish, and Portuguese. We found seven articles that were not available in the public domain, mainly data published before the 1990s. In addition, this review did not separate paid versus unpaid leave. These are significant limitations when considering the implications of paid ML, especially when bearing in mind the relationship with breastfeeding duration. As mentioned earlier, the lack of study design consistency limits the comparability among studies. Another limitation of the study design is the causation; as most studies have a cross-sectional design, it is tough to assign a direct relationship between ML and breastfeeding duration.
Despite the methodological limitations mentioned above, this study advances knowledge in many ways. First, it provides enough data to suggest that ML could support a longer breastfeeding duration, especially for women in more vulnerable jobs. Secondly, to our knowledge, this is the first review that includes articles representing the Americas, Asia, Africa, Europe, Oceania, and South East Asia. Additionally, the conceptual outline of this review offers a structure for understanding the situation of ML in more vulnerable women and the implications of this on breastfeeding. Finally, this review also provides relevant data for public health policies, showing that ML legislations do not always offer the same guarantee to all women.
Conclusion
Regardless of the WHO recommendations for EBF for at least 6 months after birth and complemented breastfeeding with other foods until the age of 2, paid ML is still not a compulsory policy worldwide. There is an urgent need to reinforce global policies on breastfeeding that will ensure EBF for at least 6 months, especially to more vulnerable groups and to women from all socioeconomic levels. Public health policies should warrant that ML benefit all working women equally.
Footnotes
Acknowledgments
The submitted work was financially supported by the Chilean National Fund for Scientific and Technological Development (FONDECYT), under the grants 1130277 and 1150878. Deborah Navarro-Rosenblatt holds a Chilean Commission of Science and Technology student fellowship to perform a PhD at the School of Public Health, University of Chile, under the grant 21151097.
Disclosure Statement
No competing financial interests exist.