
Abstract
Abstract
Objectives:
The United States has seen an increasing number of child-bearing women in medical training. We aimed to compare the prevalence of exclusive breastfeeding across varied specialties, whose trainees may face different obstacles to breastfeeding.
Materials and Methods:
An online survey querying the duration and barriers to breastfeeding was sent to Accreditation Council for Graduate Medical Education (ACGME) and American Osteopathic Association (AOA) programs. Female residents with at least one living child born during residency were eligible. We compared the prevalence of exclusive breastfeeding for 6 months between Obstetrics and Gynecology (OBGYN), nonsurgical, and non-OBGYN surgical specialties. A multiple regression model correcting for ethnicity, years lived in the United States, medical degree, year of residency at childbearing, geographical location, and clinical hours was performed.
Results:
There were 708 completed surveys, including 561 nonsurgical, 73 OBGYN, and 74 non-OBGYN surgical residents. More OBGYN residents reported exclusive breastfeeding at 6 months (43/73, 59%) than nonsurgical (217/561, 39%) and non-OBGYN surgical residents (30/74, 41%) (p < 0.01). After adjusting for confounders, OBGYN trainees were twice as likely to breastfeed (adjusted odds ratio [AOR] = 2.18, 95% confidence interval [CI] 1.28–3.72) with no difference between non-OBGYN surgical and nonsurgical residents (AOR = 1.24, 95% CI 0.70–2.19). Less OBGYN residents reported the lack of breastfeeding facilities at work (2.7% versus 17.6%, p < 0.01) and inadequate leave (4.1% versus 17.6%, p = 0.01) than non-OBGYN surgical residents.
Conclusions:
In this national survey of trainees in accredited programs, OBGYN residents were twice as likely to breastfeed and fewer OBGYN residents cited barriers to breastfeeding compared to other residents.
Introduction
Both, the American Academy of Pediatrics (AAP) and the American College of Obstetricians and Gynecologists (ACOG) have long recommended exclusive breastfeeding for 6 months after the birth of the child, with continuation for at least the first year or beyond.1,2 With the Healthy People 2020 deadline fast approaching and breastfeeding goals being an important component of this initiative, headway has been made in breastfeeding overall, but progress lags in exclusive breastfeeding at 6 months (22.3% compared to a target of 25.5%). 3
Female physicians have been identified as a risk group for formula feeding, with several studies reporting that women physicians struggle with exclusive breastfeeding.4–9 This is especially significant in residency training, where long work hours and shorter maternity leave may impact pregnancy outcomes. 10 The number of women graduating from United States medical school training programs has increased from 6.9% in 1966 to 46% in 2016. 11 There has also been an increase of female residents overall, with the largest female trainee increases seen in Obstetrics and Gynecology (OBGYN) and Pediatrics, while specialties such as Orthopedic Surgery and Neurological Surgery remaining male dominated. 12 While surgical training programs have become increasingly supportive of pregnancies during training, female residents still report negative stigma associated with pregnancy during training. 13 A recent survey noted 61% of general surgery residency program directors state that becoming a parent negatively affects the work of female trainees. 14 Trainees in surgical specialties who become pregnant are more likely to experience dissatisfaction with their career choices compared to their nonsurgical counterparts. 15
Breastfeeding can be impacted by work schedules, colleague support, and private places to breastfeed or pump. Thus, this healthy and important practice may be undermined by the divergent work demands and provisions among different residency specialties.5,16 Existing studies on breastfeeding in training physicians have looked at individual hospitals or individual residency specialties,4,6,9,14,16–22 but there is a dearth of literature comparing breastfeeding prevalence among surgical versus nonsurgical residencies.
Our primary objective lay in identifying differences between breastfeeding outcomes in surgical and nonsurgical training programs in the United States by surveying current trainees who had given birth during residency. We hypothesized that women in surgical specialty training would have a lower prevalence of exclusive breastfeeding at 6 months and cite more barriers to this practice than their nonsurgical colleagues.
Materials and Methods
Program coordinators for all Accreditation Council for Graduate Medical Education (ACGME)- and American Osteopathic Association (AOA)-accredited programs across the United States of America were contacted with the link for an anonymous, web-based survey and requested to forward the link to their female residents in this national, cross-sectional study.
This study received expedited approval from the Crozer-Keystone Health System Institutional Review Board due to the anonymous nature of the online surveys and aggregate analysis of responses. Contact information for program coordinators of ACGME-accredited programs was obtained from the ACGME Accreditation Data System. The AOA website was used to collect contact information about AOA-accredited programs and duplicates were eliminated. Almost 4,400 programs were contacted by e-mail and the program coordinators were requested to forward the survey to all female residents. Female residents who had been pregnant or had delivered at least one living child within 6 months of starting residency were eligible to complete the survey. Male residents or female residents who had not given birth to a living child during residency were excluded. The survey was made available to participants in March 2015 with one reminder e-mail sent to all program coordinators 2 weeks later. The survey was closed in April 2015.
We surveyed respondents about their demographics, including age and year of residency at time of childbearing, type of specialty, clinical hours worked, as well as their breastfeeding status, and if they introduced baby formula. Barriers to breastfeeding were assessed, and options that could be selected by the resident (allowed to pick all that applied) included “did not wish to breastfeed, inadequate milk supply, attitude of colleagues, duty hours, inadequate maternity leave, lack of facilities at work (no private space and no access to breast pumps), lack of knowledge regarding WHO guidelines to exclusively breastfeed for 6 months, inadequate prenatal counseling,” and a free text “Other” option. Finally, we surveyed factors that residents wished were present in their professional lives to enhance successful breastfeeding, with options available, including “improved prenatal counseling, increased maternity leave, time at work to breastfeed, a private space at work to breastfeed, access to breast pumps at work, and decreased work hours,” and a free text “Other” option. The full survey can be found in the Appendix A1.
Twenty-six accredited medical specialties were identified through ACGME and AOA. These were divided into surgical and nonsurgical specialty as recommended by the American Board of Medical Specialties 23 and American College of Surgeons (Table 1). The surgical group was further divided into OBGYN and surgical specialties other than OBGYN. Respondents were sorted into these groups according to their declared medical specialty.
Surgical Versus Nonsurgical Specialties
Combined Residencies: Dermatology/Internal Medicine (n = 1), Dermatopathology (n = 2), Emergency/Family Medicine (n = 3), Emergency/Internal Medicine (n = 1), Family/Preventive Medicine (n = 1), Internal Medicine/Pediatrics (n = 12), Pediatrics/Medical Genetics (n = 3), Pediatrics/Psychiatry (n = 1).
Other: Pain Medicine Fellow (n = 1), Internal Medicine Fellow (n = 1), Neuromusculoskeletal Medicine (n = 1).
Data were compared between nonsurgical residents and surgical residents first, and then between the three groups of nonsurgical residents, OBGYN residents, and non-OBGYN surgical residents. Data were exported in to Microsoft Excel 2011 and analyzed using Microsoft Excel and IBM SPSS Statistics 25. Chi-squared and ANOVA tests were used when appropriate to analyze the data, with Fisher's exact tests used for categorical comparisons where n < 5 in any category. A univariate analysis was performed and self-identified resident ethnicity, years the resident had lived in the United States, type of medical degree (allopathic or osteopathic), year of residency at the time of childbirth, and the average number of self-reported clinical hours worked per week were found to be significantly different across the three groups. A multiple regression model was used to correct the relationship between type of specialty (nonsurgical, OBGYN, or non-OBGYN surgical) and the primary outcome (exclusive breastfeeding at 6 months) for the significant suspected confounders noted above. Geographical location was also evaluated as a confounder. The significance level was set at p < 0.05 for all tests. No prior studies have compared this outcome between medical specialties, and no current data exist on the prevalence of residents giving birth during residency years, so sample size to detect a significant difference was not calculated a priori.
Results
We sent the survey to 4,386 programs with over 120,000 residents being trained in the programs at the time of the survey being dispensed. Of these, ∼54,000 residents are female with almost 44,000 residents (82%) in nonsurgical specialties and 10,000 (18%) in surgical specialties. 24 We analyzed 708 completed surveys from female residents who met inclusion criteria, with 561 (79%) nonsurgical residents and 147 (21%) surgical residents, including the field of OBGYN. A response rate could not be calculated since the number of female residents who had children during residency is unknown.
While the majority of both nonsurgical (556/561, 99%) and surgical residents (145/147, 99%) who responded reported an attempt at breastfeeding, surgical residents reported a significantly higher prevalence of exclusive breastfeeding at 6 months (217/561, 39% nonsurgical residents versus 73/147, 50% surgical residents, p = 0.02). Since the OBGYN residents comprised almost 50% (73/147) of the surgical resident respondents in this survey, we then divided our respondents in three separate groups: nonsurgical (n = 561), surgical specialties other than OBGYN (henceforth referred to as “non-OBGYN surgical”) (n = 74), and OBGYN (n = 73).
The demographic data between nonsurgical, OBGYN, and other surgical residents are displayed in Table 2. The average age at first delivery was similar across the three groups (30.0 ± 2.9 years nonsurgical, 29.5 ± 2.5 years OBGYN, 30.3 ± 2.8 years non-OBGYN surgical, p = 0.25). Most nonsurgical (401/558, 72%), OBGYN (61/73, 84%), and non-OBGYN surgical residents (54/74, 73%) self-identified as Caucasian, with more of the non-OBGYN surgical residents identifying as Asian (18%, p = 0.03). Over 90% of residents in all groups were married (p = 0.45) and almost 80% had only one child during residency (p = 0.87). While 95% of respondents in the OBGYN and non-OBGYN surgical groups had lived in the United States for over 10 years, more of the nonsurgical residents (38/552, 6.9%) had lived in the United States for 5–10 years compared to the other cohorts (p = 0.04). Fewer than 10% of the non-OBGYN surgical respondents reported their medical degree as a doctor of osteopathic medicine (DO) compared to 24.2% of non-\surgical and 30.1% of OBGYN residents (p < 0.01).
Respondent Demographics
Bold values are significant results with p < 0.05.
Ethnicity available for 558/561 nonsurgical respondents.
Geographical location available for 560/561 nonsurgical respondents.
Northeast: Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, Vermont.
Midwest: Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, Wisconsin.
South: Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, West Virginia.
West: Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, Wyoming.
Unclassified: Puerto Rico.
Marital status available for 559/561 nonsurgical respondents.
Length of stay in the United States available for 698 respondents (nonsurgical = 552, non-OBGYN surgical = 74, OBGYN = 72).
DO, doctor of osteopathic medicine; OBGYN, Obstetrics and Gynecology.
There was a significant difference in the number of clinical hours worked between the three groups. The majority of nonsurgical residents reported a 40–60 hour work week, while the majority of OBGYN and non-OBGYN residents reported a 60–80 hour work week (p < 0.01). A quarter of other surgical residents reported that their first pregnancy was greater than 4 years in to their residency training compared to third year for both nonsurgical and OBGYN residents (p < 0.01).
More OBGYN residents reported exclusive breastfeeding at 6 months (43/73, 58.9%) than nonsurgical (217/561, 38.7%) and non-OBGYN surgical residents (30/74, 40.5%) (p < 0.01). At 12 months, 208 respondents (29.4%) were still exclusively breastfeeding, but there was no significant difference between the three groups. A univariate analysis revealed that exclusive breastfeeding at 6 months was associated with the years spent living in the United States, with only 21% of residents who have lived in the United States for fewer than 5 years and 42% of those who have lived in the United States for over 10 years reporting exclusive breastfeeding (p < 0.01).
On the multiple logistic regression model, OBGYN residents were twice as likely to exclusively breastfeed when compared to their nonsurgical counterparts (adjusted odds ratio [AOR] = 2.18, 95% confidence interval [CI] 1.28–3.72). There was no significant difference between non-OBGYN surgical residents and nonsurgical residents (AOR = 1.24, 95% CI 0.70–2.19). After correction for other factors (Table 3), the association between years spent living in the United States and exclusive breastfeeding found on the univariate model was no longer significant (AOR = 0.44, 95% CI 0.14–1.40).
Factors Associated with Exclusive Breastfeeding at 6 Months
Bold values are significant results with p < 0.05.
Reference value.
Fisher's exact test.
Geographical location available for 560/561 nonsurgical respondents.
Northeast: Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, Vermont.
Midwest: Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, Wisconsin.
South: Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, West Virginia.
West: Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, Wyoming.
Unclassified: Puerto Rico.
AOR, adjusted odds ratio where appropriate; CI, confidence interval; DO, doctor of osteopathic medicine; OBGYN, Obstetrics and Gynecology.
Subject responses to query about breastfeeding barriers are displayed in Figure 1. Fewer OBGYN residents reported a lack of breastfeeding facilities at work than non-OBGYN surgical subspecialties (2.7% versus 17.6%, p < 0.01). Also, fewer OBGYN residents reported inadequate maternity leave as a barrier compared to their non-OBGYN surgical colleagues (4.1% versus 17.6%, p = 0.01). Almost one-third of all respondents cited inadequate milk supply, making this the most commonly cited barrier among all residents. In contrast, only 6% of residents quoted the attitude of colleagues as a hindrance toward breastfeeding.
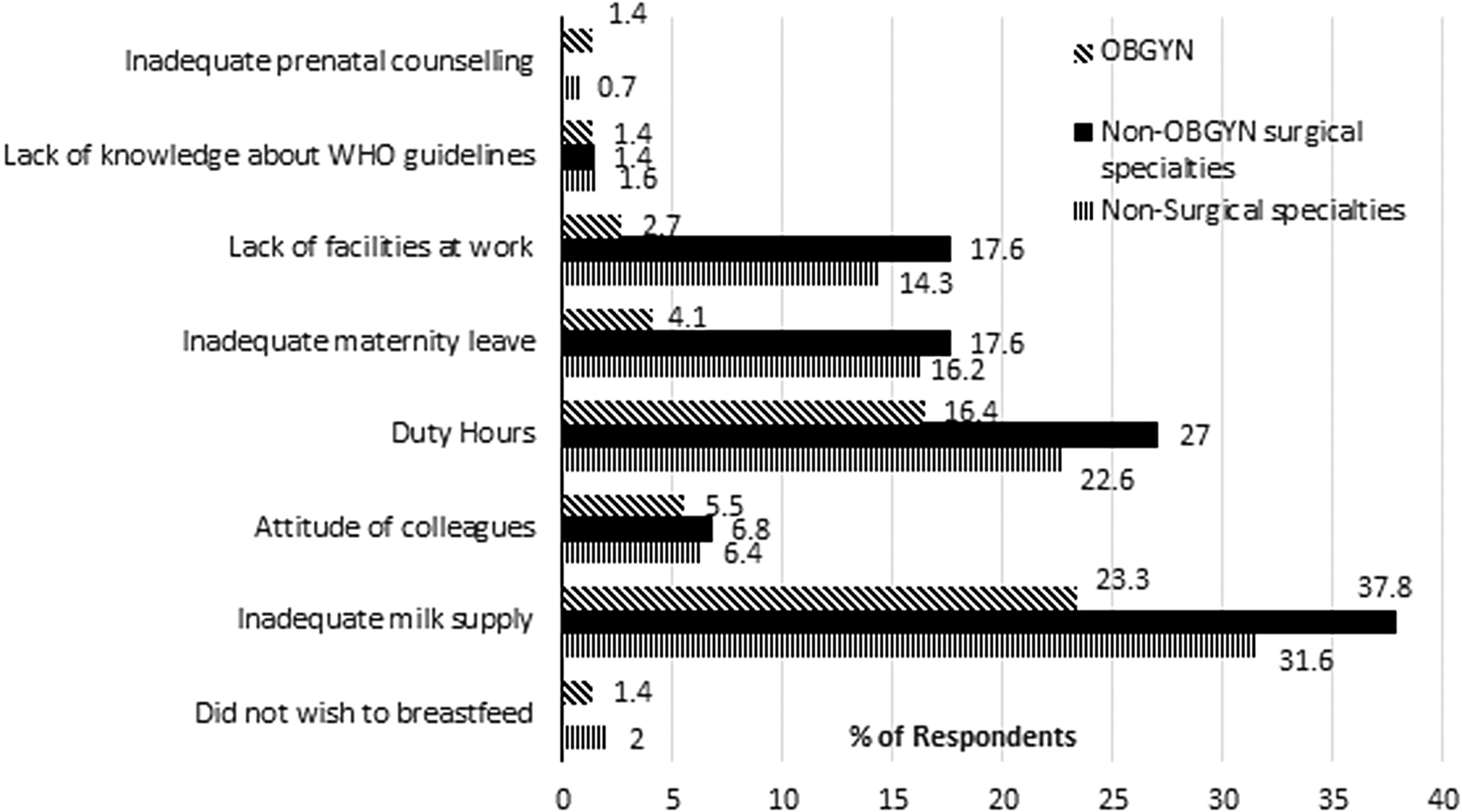
Prevalence of citation of barriers to breastfeeding in the study survey.
Factors residents stated they desired to improve their breastfeeding experience are displayed in Figure 2. Almost half the residents across all specialties wished they had more time at work to breastfeed. Fewer OBGYN residents (15/73, 21%) cited increased maternity leave as a desired factor to help them breastfeed compared to residents in non-OBGYN surgical fields (34/74, 45.9%, p > 0.01). Although one-third of residents cited further decrease in duty hours as a factor they desired to help them breastfeed, this was not significantly different across the three groups (p = 0.22).
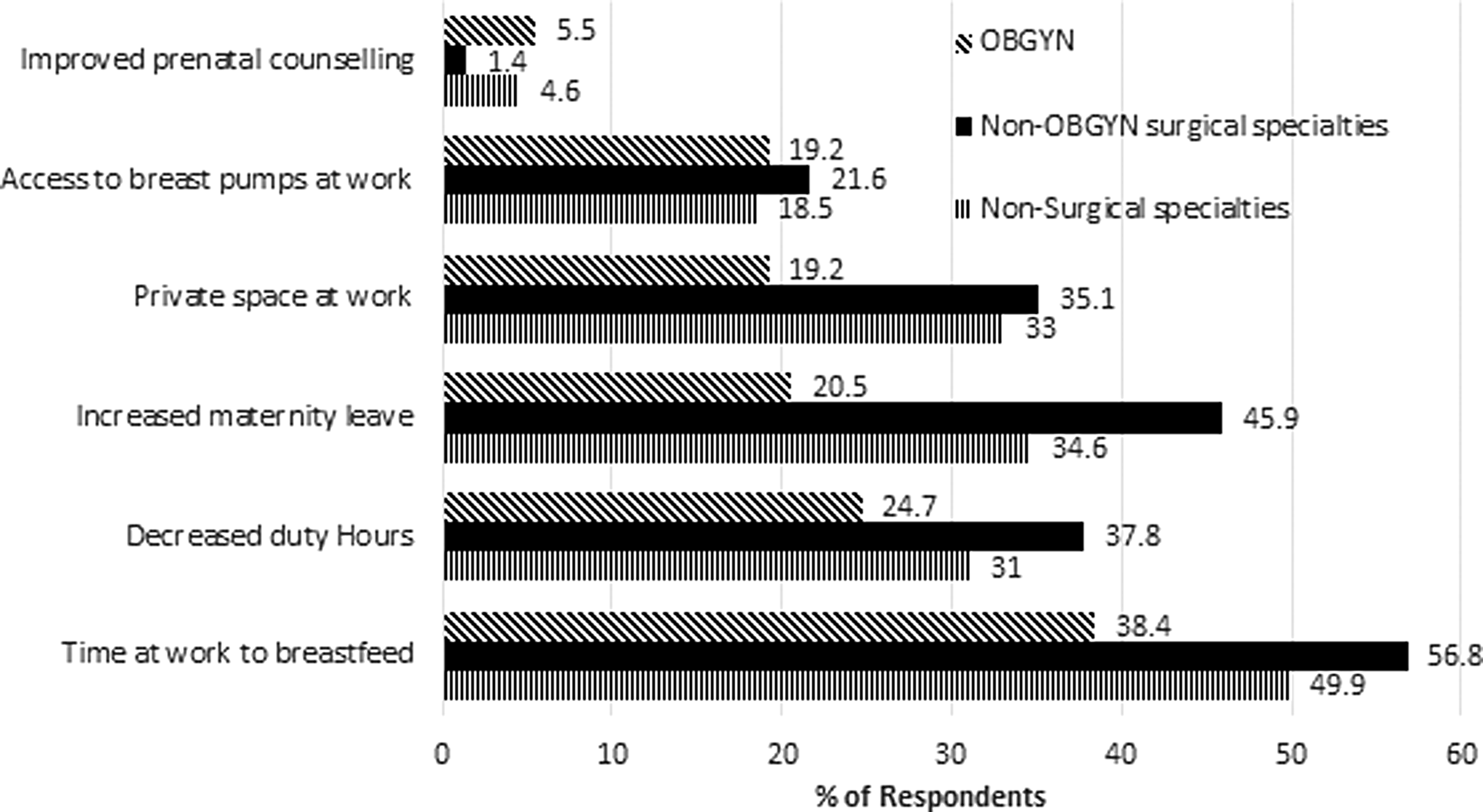
Prevalence of citation of factors desired to improve breastfeeding experience in the study survey.
Discussion
This national survey regarding personal breastfeeding experience in medical residency training among female physicians found a significant difference in the prevalence of 6 months of exclusive breastfeeding between OBGYN and other specialties, with nonsurgical and other surgical residents breastfeeding less commonly for this duration. This difference persisted despite correction for confounders, with OBGYN's more than twice as likely to breastfeed for 6 months despite the majority of all residents reporting an attempt at breastfeeding.
Barriers to breastfeeding varied across training specialties, with fewer OBGYNs reporting inadequate maternity leave and lack of breastfeeding facilities at work. It has been established that family life and lifestyle factors can influence the decision for surgical residency among female medical graduates.19,25 As the number of female medical graduates increases, 10 an increased emphasis on work-home balance may inform the decision for residency training, especially if there are significant differences between the various specialties.
Previous literature has alluded to these differences. OBGYN residents have consistently experienced a positive environment for resident pregnancy, with studies quoting 90% of residents familiar with a breastfeeding colleague.6,13,26 A recent survey reported that residents in anesthesia and internal medicine, and non-OBGYN surgical residencies report a negative stigma associated with pregnancy compared to their OBGYN counterparts. 13 This appears to carry over into breastfeeding practices. While our study supports the high breastfeeding initiation rates among all physician mothers,4,16,17 our OBGYN respondents were significantly more likely to carry this practice on to exclusively breastfeed at 6 months. This result is concerning for women across all of medicine, as no woman should be unsupported in her motivation to be healthy and have a healthy infant due to her choice of specialty or because of negative or uninformed attitudes within her colleagues. It highlights a need for education and action in all areas of medicine.
Access to breastfeeding facilities at work could also explain breastfeeding differences, with eight times as many non-OBGYN surgical residents citing inadequate breastfeeding facilities as a barrier when compared with OBGYN peers. Other studies have reported the need for a private facility to breast pump while at work, and as many as 73% of pediatrics residents report access to a private room to breastfeed. 4 While over 60% of surgical residents report the presence of a lactation facility, they were hampered by limited numbers and proximity to the operating room.19,22 This study found that one-third of non-OBGYN surgical residents felt that a private space at work would have helped their ability to exclusively breastfeed. It is clear from these past results and our survey that “inadequate facilities” may mean a variety of factors, including number, privacy, locations, and use timing of rooms. All these factors must be considered if employers seek to enhance this healthy practice in their residents.
Female mentorship has been identified as a vital component of supportive environments for resident pregnancies, with studies suggesting that the presence of women in leadership roles may foster work–life balance, 13 and mentorship may play a role in breastfeeding as well. This survey found that the attitude of colleagues was cited as a barrier with similar prevalence across groups, but this survey did not query the role of colleagues or mentorship specifically. Surgical trainees have reported a lack of childbearing mentorship in a past study, with two-thirds expressing a desire for mentorship in integrating pregnancy with a surgical career. 22 Obstetrics and Gynecology has seen a dramatic rise in its female membership with over 80% of residents in 2015 identifying as female. 12 ACOG recently reported that almost 60% of OBGYN members in active practice are women, a number that exceeds any group of active surgeons or physicians. 27 One cannot help, but consider that this enhances the supportive environment experienced by OBGYN residents, and more specific questions as to the role of “woman-to-woman” mentorship in specialties may reveal more about this factor.
An additional barrier to breastfeeding cited in this survey was inadequate maternity leave, especially among non-OBGYN surgical and nonsurgical residents. Certain boards, including American Board of Surgery, limit the time away from residency, forcing trainees to extend the duration of their residency. 22 Historically, OBGYN residency programs have reported formal maternity leave policies,19,28 while studies have identified the lack of maternal policies and the dissatisfaction associated with this lack in other surgical residencies.15,19,22 Almost half the surgical residents identified increasing maternity leave as a factor that would help them breastfeed, with only 20% of OBGYN residents reporting a similar need. Predictor models have suggested that even a 1-week increase in maternity leave can significantly impact the duration of breastfeeding. 29 Our study further highlights the importance of policy agreement in a “hospital-wide” manner as well as making sure that residents are aware of these policies, so that all residents can benefit equally from these rights. A formal maternity leave policy could alleviate some of the anxiety surrounding breastfeeding. 22
Duty hours, especially in surgical specialties, have been reported to act as a barrier to breastfeeding among residents.5,6,19 With the implementation of work hour restrictions, programs are required to ensure their residents work fewer than 80 hours per week. 30 Despite this, almost 18% of surgical respondents, including OBGYN, reported working more than 80 hours on this anonymous survey. While we expected this to play a large role in breastfeeding, there was no significant difference among the groups in reporting duty hours as a breastfeeding barrier. This confirms that although OBGYN and non-OBGYN surgical residents state that they work longer hours than their nonsurgical counterparts, an environment promoting childbirth and breastfeeding (such as the adequate maternity leave and access to facilities that many OBGYNs seem to enjoy) may be more important than shortening hours worked. Implementation of fixed breastfeeding policies, including providing time and facilities for pumping breast milk at work, should be considered by residency programs regardless of specialty.
Strengths of this study include size of the cohort and ability to compare between medical specialties. While there have been a handful of studies looking at residents in various specialties, they are limited by their small cohort or single institution.5,7,13,31 This large cross-sectional survey reached over 700 participants in 28 medical specialties. By limiting it to female residents who had given birth to at least one child in residency, we targeted the individuals who were most affected and invested in breastfeeding. Also, we corrected for relevant confounders and considered how barriers and desires residents report around breastfeeding interplay with the outcome of exclusive breastfeeding. This approach can better inform policy or interventions to improve breastfeeding practices than past cohorts that merely describe the frequency of breastfeeding among residents.
Limitations to our study include the inability to verify the size of the eligible population and the number of women needed to study this issue. While the Association of American Medical Colleges tracks the number of women in different specialties, the number of female residents who have had children in residency is not tracked, making it hard to calculate a response rate due to absence of an appropriate denominator. Despite this, the breakdown of 79% nonsurgical and 21% surgical respondents is similar to the ACGME-reported data about female trainees and suggests adequate representation of the specialties. 24 In addition, this survey was sent to program coordinators who were requested to forward this survey to their female residents, thus potentially introducing a selection bias.
Other limitations include biases inherent to a retrospective study. Acceptability bias is particularly concerning in this survey, as breastfeeding is known by medically trained people to be a healthy practice and female physicians, particularly in fields concerned with women and infants like OBGYN and Pediatrics, may be more likely to overreport breastfeeding attempt or success. Although this was an anonymous survey, OBGYN residents may be more tempted to misreport their breastfeeding experiences. Nonresponse bias may have played a role and the residents with the best experience may have responded to the survey. Residents who chose to formula feed, partially breastfeed, or failed to initiate breastfeeding may not have completed the survey, especially given the 99% rate of breastfeeding initiation. Selection bias is suspected due to a large percentage of our respondents belonging to the nonsurgical group. This could possibly be due to a higher proportion of female residents having children in nonsurgical specialties or that surgical residents work significantly more hours and have less time or inclination to complete our survey. Recall bias also may play a role, as some respondents completed the survey up to 2–4 years following their childbirth and breastfeeding practice.
Conclusions
Our national survey of female U.S. residents with personal experience of childbirth during residency found that OBGYN residents were twice as likely to breastfeed compared to their nonsurgical and other surgical specialty peers. Lack of facilities at work and inadequate maternity leave were significant barriers to breastfeeding for non-OBGYN surgical and nonsurgical residents, although these factors seem less problematic in the OBGYN specialty. As the number of women in medical training programs increase, standardized policies for breastfeeding and maternity leave across all residency programs may improve the resident experience with breastfeeding, regardless of specialty.
Footnotes
Acknowledgments
This research was presented at the 20th annual meeting of the Academy of Breastfeeding Medicine held October 15–18, 2015, in Los Angeles, CA. K.M. is a book author and editor for Elsevier.
Disclosure Statement
No competing financial interests exist.