
Abstract
Abstract
Objective:
To compare the effects of different relaxation techniques on physiological outcomes and perceived relaxation in primiparous Chinese mothers breastfeeding their healthy term infant.
Design:
Twenty primiparous mothers who were breastfeeding were enrolled into a within-subject study, and attended six treatment sessions in randomized order (relaxation meditation tape [RM], music tape [M], relaxation lighting [L], combined RM+L, and combined M+L, and control session with no intervention), with a washout period of 1–3 days between sessions. Heart rate, systolic and diastolic blood pressure (SBP, DBP), fingertip temperature, and perceived relaxation were assessed before and after each session.
Results:
Compared with the pretest state, significant changes for all outcomes (p < 0.05) were observed for RM, RM+RL, M+RL treatments, whereas differences for all outcomes apart from SBP were observed for treatment M. Compared with the control, significant changes were found in all outcomes for RM treatment, and in fingertip temperature and perceived relaxation for all treatments.
Conclusion:
Our findings suggest that simple relaxation techniques can reduce both perceived and physiological markers of stress in breastfeeding mothers. Overall, the RM was the most effective technique compared with the control state, considering the number of outcomes affected, effect sizes, and simplicity, suggesting this merits further research in this population.
Introduction
Breastfeeding is of great importance for infant health and development. 1 Increasing evidence shows the effects of human breast milk on optimizing infant growth and development, as well as protecting against infection and developing the immune system.1–4 A recent Lancet review also emphasized the psychological and cognitive benefit of human breast milk for infants. 2 Apart from the health benefits for infants, breastfeeding could provide mothers with a better postpartum recovery,1,2 and is associated with decreased risk of osteoporosis, cardiovascular diseases, diabetes, and ovarian and breast cancer in later life.2,5–8 However, despite a number of health programs designed to promote breastfeeding, it is widely recognized that the exclusive breastfeeding rates in many countries are disappointingly low and resistant to change. 2 Globally, only 39% of mothers exclusively breastfeed their infants up to 6 months (UNICEF 2012). 9 Apart from the socioeconomic and cultural factors, which may influence mother's decision on breastfeeding, lactation performance, such as breastfeeding duration and breast milk volume, is also influenced by maternal physiological and psychological condition. 10
Stress can influence the hypothalamic–pituitary–adrenal (HPA) axis thereby affecting lactation. 11 A number of studies reported the effectiveness of relaxation techniques on reducing stress and anxiety and increasing milk yield in mothers with preterm infants.12,13 In a previous study, maternal psychological state was manipulated using relaxation meditation (RM) in 64 Malaysian mothers breastfeeding their full-term infant. 14 The therapy showed significant effects in reducing maternal stress during lactation, favorably affecting breast milk composition (higher fat/energy and higher total carbohydrate) and positively influencing infant sleeping behavior and growth.
Apart from RM, there are many well-documented relaxation methods for the reduction of stress and anxiety, including relaxation training, 15 guided imagery, 12 music therapy, 16 yoga, and progressive muscle relaxation (PMR). 17 Moreover, light therapy is another technique, which may be used to promote relaxation. Evidence shows that light can stimulate the suprachiasmatic nucleus (SCN) in the hypothalamus and influence the secretion of cortisol and adrenocorticotrophic hormone by mediating the HPA axis. 18 Research also indicates that light may induce gene expression (circadian clock-related or sleep-related genes in depression) in the adrenal gland through the SCN-sympathetic nervous system. 19 An increasing number of studies have reported the application of light therapy for the treatment of a range of mental diseases, namely seasonal affective disorder, 20 nonseasonal depression, 21 total sleep deprivation, 22 and antepartum depression.23–25
Most existing studies evaluating the effectiveness of relaxation therapies only look at one intervention rather than comparing different ones. Moreover, there is a lack of research investigating the effects of relaxation therapy specifically in breastfeeding mothers. A recent systematic review evaluated six studies (three observational, three experimental) investigating the effect of relaxation techniques on breastfeeding outcomes. 26 While the results showed that relaxation therapy might significantly improve milk yield, methodological issues were identified, such as high variability in the milk collection protocol and assessment time points among six studies. Hence, the aim of the present study was to compare the effects of different relaxation techniques on reducing stress in mothers breastfeeding their healthy term infant. We evaluated the effects of five different relaxation techniques on physical and psychological changes using a within-subject study design. Our aim was to identify the most effective relaxation technique for use in future research to test the hypothesis that reducing maternal stress could result in enhanced milk ejection and improved breastfeeding outcomes.
Materials and Methods
Study design
The study was conducted at a local community clinic attached to Beijing Children Hospital in China. A within-subject design was used to evaluate the effectiveness of the five tested interventions compared with a control situation. Recruitment was performed using flyers in the local community, and advertisements posted in the hospital and community clinic. The study information sheet was given to interested women. Eligibility criteria were: (1) primiparous mothers who were currently breastfeeding their infants within 2 years after delivery; (2) 23 to 45 years of age; (3) generally healthy (without any diseases that could influence blood pressure (BP), heart rate (HR), energy expenditure, or breastfeeding practice); (4) not currently participating in other studies; and (5) nonsmoker.
After obtaining written informed consent, participants were invited to attend the clinic every 1–3 days on six occasions (five relaxation sessions and one control session). The six sessions were coded as: 0 = control, 1 = RM, 2 = M, 3 = L, 4 = RM+L, and 5 = M+L. The order of the six sessions was randomly assigned for each participant using a computerized random number generator. This was performed by an independent person who had no contact with the subjects. To control for circadian rhythm, all sessions were performed in the afternoon between 2:00 PM and 4:00 PM. The duration of each treatment was 10 minutes, with additional 10-minute pre- and posttest measurements. Each treatment was conducted in a breastfeeding room at the clinic, where participants were comfortably seated and guided by the researcher. The participants were encouraged to report any comments about their experience to the researcher after each session; such issues were noted in the demographic questionnaire of the participants. The infants of participants were not present during the session. Ethical permission for the study was obtained from the Research Ethics Committee of University College London (ID: 12681/001) and the leaders of Center for Child Health, Beijing Children Hospital. The trial was registered at clinicaltrials.gov (NCT03593551).
Interventions
The RM used in this study was a modified version of a guided imagery meditation tape, which was originally developed by Sheri Menelli in 2004 for breastfeeding mothers. The researcher translated it into Chinese (Mandarin) and shortened the content to focus on the relaxation part with the assistance of a psychologist. The Mandarin version of the tape was recorded by a certified yoga therapist with prior experience of recording meditation tapes. Two types of music were used in this study; New-age music and traditional Chinese music played on a classical instrument. Participants could choose their preferred music to enhance relaxation and stress reduction. The light therapy used in the L, RM+L, and M + L treatments was generated using the Philips Hue system, whereas the lighting during the nonlight treatments (RM, M) was a standard light. Participants could choose either the orange light (“Relax” setting) or the blue light (“Energize” setting) to meet their preference and the intensity of the light could also be altered.
Outcomes and measures
The primary outcomes of this study were changes in HR, BP, fingertip temperature, and perceived relaxation for each treatment compared with the control. Systolic BP (SPB), diastolic BP (DBP), and HR were measured in the seated position using an automatic BP machine (Yuyue, China) by trained nurses with at least 10-minute rest period before the pretreatment measurement. The posttreatment measurement of BP will be conducted immediately after the treatment considering the participants were rested during the treatment. A digital body thermometer (Care1st, China) was used for measuring the fingertip temperature. These assessments were carried out three times and the mean of the closest two readings was used. Perceived relaxation was assessed by a visual analog scale (VAS), which consists of a horizontal 10 cm line with one end representing the maximum and the other end the minimum of the variable to be measured. The right anchor of the scale was identified as “completely relaxed” and the left anchor was labeled “completely unrelaxed.” Participants indicated their state of relaxation by marking a point along the line before each session and again at the end of each session. The distance from the left anchor to the mark made by participants was measured in millimeters and pre- and posttest differences were compared.
Sample size calculation
Sample size for paired comparisons (between each treatment and the control situation) was calculated using the formula
21
:
A previous study, 22 which evaluated the effect of audiovisual imagery on patient anxiety and physiological parameters reported a significant reduction in HR with a mean of 0.75 and standard deviation (SD) of 1. Accordingly, the estimated sample size was 14. To allow for dropouts, we aimed to recruit 20 subjects.
Statistical analysis
Data were analyzed using SPSS 23.0. Mean and SD were used to summarize the characteristics of the entire sample. Paired t test was used to analyze changes in each of the outcomes before and after the different treatment sessions. Paired t test was also computed to compare the mean difference of each treatment to the control state. Differences were considered statistically significant at p < 0.05.
Results
The study was carried out from 3rd June to 28th June 2018. All participants attended the full six sessions. Descriptive characteristics of the participants are presented in Table 1. The mean age of the participating mothers was 32.2 (±3.29), and the mean age of their infants was 7.55 months (±6.18). Sixteen participants were exclusively breastfeeding their infants, whereas four participants were using mixed feeding. No participants were unwell during the study period.
Demographic Characteristics of the Sample (Mean and Standard Deviation)
BMI, body mass index; SD, standard deviation.
Changes in BP, HR, fingertip temperature, and perceived relaxation during each session
Table 2 shows the mean differences in the primary outcomes pre- and posttest for each treatment. Overall, except for the control session, all relaxation sessions showed reduced BP and HR and increased fingertip temperature and perceived relaxation after the session (Fig. 1). The RM, RM+RL, and M+RL treatments showed significant differences before and after the test for all primary outcomes (p < 0.05). For treatment M, significant differences between pre- and posttest were found for all outcomes, except SBP.
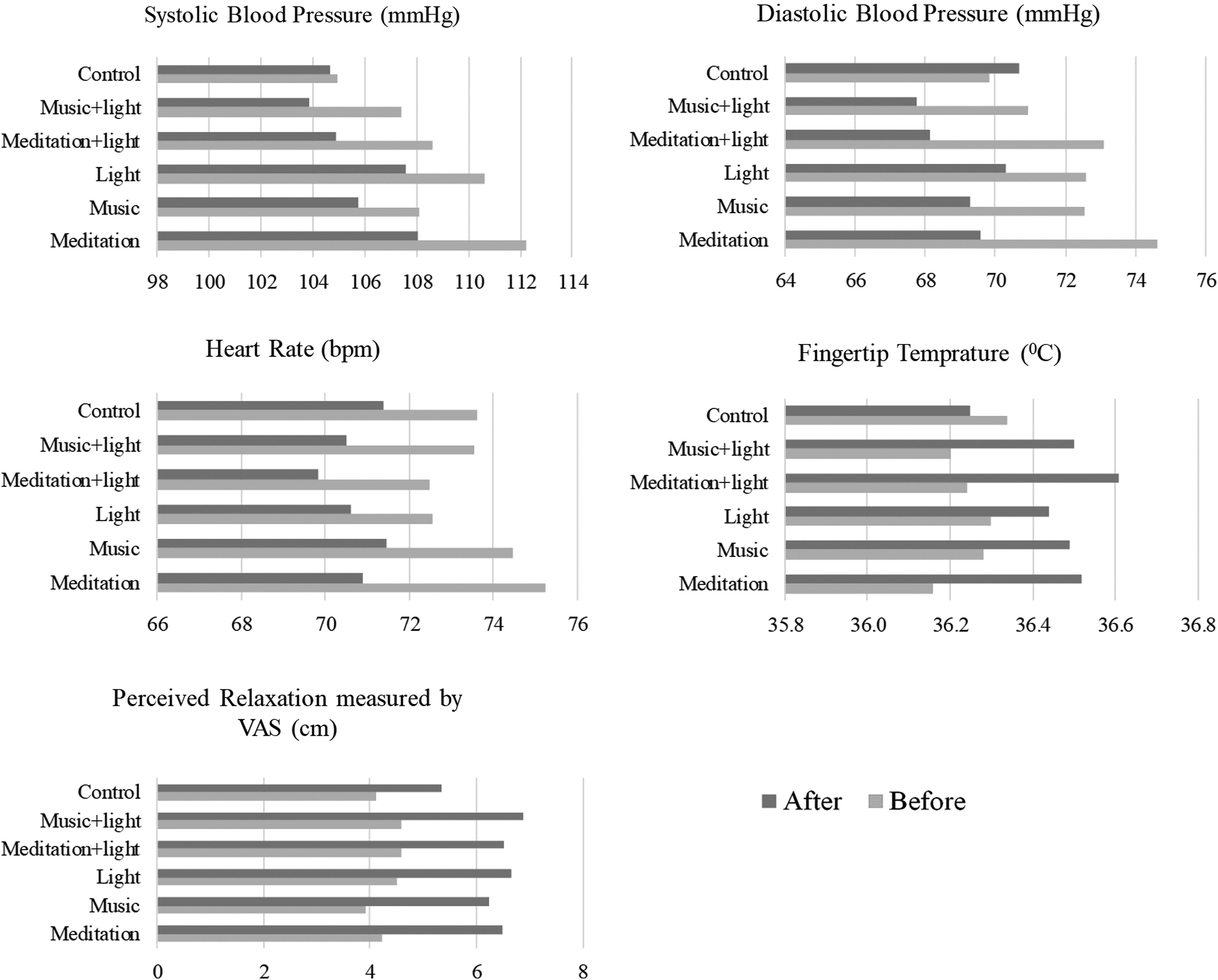
Pre–Post changes among six sessions.
Mean and Standard Deviations of the Outcomes of Six Sessions
p < 0.05; **p < 0.01.
DBP, diastolic blood pressure; FT, fingertip temperature; HR, heart rate; M, music; M+RL, music plus lighting; Relax-VAS, perceived relaxation measured by visual analog scale; RL, relaxation lighting; RM, relaxation meditation; RM+RL, relaxation meditation plus lighting; SBP, systolic blood pressure.
Comparisons of mean changes in each outcome between relaxation sessions and the control
Paired t tests were conducted to compare the changes in primary outcomes for each treatment with the control state. As shown in Table 3, significant changes were found in all primary outcomes in RM compared with the control. For fingertip temperature and perceived relaxation, significant differences were found for all treatments when compared with the control state (p < 0.01). Additionally, the SBP and DBP were reduced in all treatments compared with the control state, although some of the changes were not significant (Table 3).
Mean Differences of the Primary Outcomes in Five Interventions Compared with the Control State
p < 0.05; **p < 0.01.
CI, confidence interval.
Four participants, with infants 1–3 months of age, experienced milk let-down (ejection) during the session using the RM treatment. This was not reported for the remaining four treatments or control session.
Discussion
This study showed that, compared with the control state, all five relaxation interventions tested had significant effects with increased fingertip temperature and perceived relaxation in Chinese mothers who are currently breastfeeding their infants. A significant reduction in BP and HR was also observed following the RM, RM+RL, and M+RL treatments. When compared with the control state, the RM produced significant changes in all measured outcomes and resulted in the greatest change in SBP, DBP, and HR, whereas the M+RL showed the greatest mean change in fingertip temperature and perceived relaxation.
A previous randomized controlled trial (RCT) compared the effects of music, PMR, music-assisted PMR, and silence on measures of anxiety and perceived relaxation in 60 university students (15 randomly assigned to each treatment; mean age = 22.2 years). 27 Anxiety and perceived relaxation were measured by the State Trait Anxiety Inventory and VAS, respectively, and all participants achieved significant relaxation responses regardless of the treatment type. However, physiological responses were not examined in this study and the relaxation status was measured using a self-rating scale. This may result in reporting bias, where the participant may either expect to feel more relaxed after treatment, or believe that they are expected to report this by the researcher. The same criticism applies to the VAS used in our study but, to address this issue, we also measured three physiological outcomes—BP, HR, and fingertip temperature—to objectively evaluate the relaxation response. Previous research suggested that positive emotion could affect the endothelium vasoreactivity, 28 which was associated with reduced BP and HR. We found that, compared with the pretest state, the VAS was significantly increased after all interventions, but also after the control session (Table 2), whereas the physiological outcomes did not show significant changes during the control session. This could suggest that the VAS is indeed subject to reporting bias, or alternatively that the subjective feeling of relaxation measured using the VAS reflects a different process from the relaxation measured by physiological responses.
A previous RCT evaluated the effects of listening to different types of music versus no music on perceived and physiological indicators of stress in 56 undergraduate students (mean age = 21 years). 29 Both physiological indicators (skin temperature, frontalis muscle tension, HR) and a perceived indicator (ratings of relaxation, measured by self-rating scale) were assessed. No significant differences in physiological indicators were found between different types of music, whereas significant increases were found in perceived relaxation (p = 0.004) in the classical, self-selected relaxation music and no music groups. The author concluded that people who reported that listening to certain types of music helped them to relax may not be classified as relaxed using physiological indicators. As suggested by Gay Peterson, 30 the stress response can be defined as a complex reaction, which often includes physiological, cognitive, and behavioral components. Hence, certain relaxation technique could influence different components of an individual's stress response. Physiological and perceived indicators may detect a reduction in physiological and cognitive stress, respectively. Thus, a significant cognitive relaxation effect may be detected by an indicator of perceived relaxation without changes in physiological indicators. However, more experimental studies in this area are needed to further investigate this interpretation.
Regardless of the perceived relaxation, comparisons of changes in physiological outcome measures from pre- to postintervention showed that the RM resulted in the greatest mean difference for SBP, DBP, and HR, whereas the greatest mean difference for fingertip temperature was found using RM+RL, followed by RM. Moreover, four participants were recorded to experience the let-down reflex during the RM session but not in other sessions. The let-down reflex is affected by maternal psychological state, and milk ejection could be stimulated by reducing maternal psychological distress or increasing relaxation.26,31 Although this was reported in only four mothers, it is interesting that their infants were only 1–3 months of age (the youngest among the study participants) and thus feeding more frequently. This observation, combined with the observed effects on the outcome measures, suggests that the RM treatment may be particularly effective in promoting relaxation and milk ejection in breastfeeding mothers.
The strengths of the study include the use of a within-subject design, allowing several relaxation interventions to be tested and compared in a single study. All 20 participants attended their six sessions during the study period, reflecting a high level of engagement and sustained involvement. The study also has some limitations. First, only 20 participants from one community in Beijing were enrolled, so the population may not be representative. However, since the ultimate aim of this research was to select the most appropriate relaxation technique for breastfeeding mothers to be used in a subsequent trial, which will be conducted in Beijing, the current study participants were recruited from the area where the main study will take place. A potential disadvantage of the within-subjects design is that there might be “carryover effects” of one intervention on the next. However, the order of the six sessions was randomly assigned for each participant, there was a 1- to 3-day period between sessions and the expected effects of each intervention were expected to be short lived. Finally, it is important to note that we evaluated short-term responses to the relaxation interventions after a single session; it is possible that responses to more prolonged, repeated use of the interventions would differ and this should be considered when designing future studies. Such studies should include a larger sample and, importantly, investigate the effects of the intervention on outcomes related to lactation performance such as the breast milk volume, energy content, and breastfeeding duration.
Conclusion
Our findings suggest that simple relaxation techniques can reduce both perceived and physiological markers of stress in breastfeeding mothers. Overall, the RM was the most effective technique compared with the control state, considering the number of outcomes affected, effect sizes, and simplicity, suggesting this merits further research in this population.
Footnotes
Acknowledgments
The authors would like to thank the Sanlihe community clinic, Beijing, China, for providing advice and instruments for this pilot study. Moreover, the authors would like to thank Ms. Cheng Yulan for contributing to the relaxation tape recording work.
Disclosure Statement
No competing financial interests exist.