
Abstract
Abstract
Objective:
To explore the relationship of early breastfeeding behaviors after Cesarean section (CS) to long-term breastfeeding outcome.
Materials and Methods:
A total of 648 healthy breastfeeding primiparas (333 delivered by CS, and 315 by vaginal birth) were recruited from three teaching hospitals using probability proportional to size sampling method. Data of the first 3 days breastfeeding behaviors, including breastfeeding initiation, frequency and duration, formula supplement, and infant sucking performance, were gathered. Ordinal cumulative odds logistic regression model were conducted to explore the effect of CS on breastfeeding outcome at fifth day, and first, fourth, and sixth month before and after adjusting for the variants of early breastfeeding behaviors.
Results:
The unadjusted odds ratios (ORs) for lower breastfeeding rates associated with CS were 2.11 (95% confidence interval [CI]: 1.58–2.81), 2.67 (95% CI: 1.96–3.63), 1.60 (95% CI: 1.19–2.15), and 1.36 (95% CI: 1.01–1.83) at the fifth day, and first, fourth, and sixth month. After adjusting for the early breastfeeding behaviors, the negative effect of CS on long-term breastfeeding was attenuated, and no longer significant at fifth day (OR: 1.01, 95% CI: 0.70–1.47) and fourth month (OR: 1.13, 95% CI: 0.79–1.62) and sixth month (OR: 0.81, 95% CI: 0.56–1.17).
Conclusions:
CS had a detrimental effect on early breastfeeding behaviors and long-term breastfeeding outcomes. CS per se is not a negative factor, but rather those infants who have feeding difficulties in the immediate postpartum period have long-term problems.
Introduction
Increasing the duration and exclusivity of breastfeeding is a recognized public health priority, due to its unparalleled advantages in optimal infant development and maternal health. World Health Organization (WHO) recommends a 6-month exclusive breastfeeding and breastfeeding up to 2 years of age. However, the exclusive breastfeeding rate at the sixth month is no >30% globally. 1 Cesarean section (CS) has been proved to be an independent risk factor for breastfeeding. 2 Mothers who experienced CS encounter more problems in breastfeeding. Compared with mothers after a normal vaginal delivery, those women who underwent CS tend to cease breastfeeding or exclusive breastfeeding at an early stage. 3
Previous studies have reported that the special problems of breastfeeding related to CS include exposure to anesthesia 4 or antibiotic, 5 unsatisfied infant sucking activity, delayed breastfeeding initiation, and postpartum maternal fatigue and depression. Lai et al. 6 observed that women after CS experienced heavier postpartum fatigue during the first 3 days, and in turn, the fatigue led to difficulties in baby-care activities. CS newborns suffer a delayed breastfeeding initiation because of possible drug residue exposure. Health care providers have reported the potential harm of delayed first suction to long-term breastfeeding and infant survival. 7 CS infants display poorly coordinated tongue movements and delayed onset of lactation. 8 Our previous study detected a weaker suction pressure in CS infant. 9 Suction problems impede milk transfer and lactation. Therefore, mothers after CS are more likely to use formula in the early postpartum period. 10
However, the role of specific early breastfeeding behaviors in infants born after CS and long-term breastfeeding rates remains unclear. This research thus compared breastfeeding behaviors in the first 3 days postpartum, including breastfeeding initiation, frequency, and duration, formula supplement, and infant sucking performance in the relationship to 6-month breastfeeding rates in infants born either by the vaginal route or by CS.
Materials and Methods
Study design and sampling
This research was a multicenter, prospective cohort study. A two-stage sampling method was conducted.
In the first stage, three hospitals were randomly selected using the probability proportional to size sampling method. Initially, we got the birth data (2011–2013) of all registered hospitals of Nantong city from the government agency of Maternal and Child Health Institution. Then, constituent ratios based on their amount of births were calculated. The hospitals were ordered in sequence by letters of the name and encoded with a segment of numbers by their constituent ratios. Our target hospitals were those that contained the corresponding computer-generated random numbers.
Second, all mother-infant dyads in the three hospitals were enrolled from September to December in 2014. The number of newborns delivered in the three hospitals (Affiliated Hospital of Nantong University, Maternal and Children Health Care Service Hospital, and the First People's Hospital of Nantong City) accounts for over 70% of the total births in Nantong city.
The protocol was approved by the Ethics Committee of Nantong University (2014-069) and registered on Clinical Trial Registry. Verbal and written information regarding the aims, procedures, and potential risks and benefits were introduced to all participants. They were informed the freedom to withdraw unconditionally from our research. Written informed consent was obtained from each participant before the protocol.
Participants
We recruited healthy single-birth primiparas from 20 years of age to younger than 35. The parturient delivered a healthy full-term newborn with an Apgar score of >8. The infant was fed from the breast directly. The exclusion criteria were: (1) breastfeeding contraindication; (2) any other condition which may impede successful breastfeeding or lactation, such as inverted nipple, breast surgery/injury, hypothyroidism, hypopituitarism, polycystic ovarian syndrome, ovarian theca-lutein cyst, placenta implantation, amniotic fluid embolism, diabetes, hypertension, or postpartum hemorrhage; (3) mother-infant separation during the first day after birth, for example, newborn was transferred to the Neonatal Intensive Care Unit; (4) maternal smoking; (5) prepregnant body mass index ≥27 kg/m2; or (6) assisted vaginal delivery by forceps or vacuum extraction.
Data collection
Early breastfeeding behaviors
Early breastfeeding behaviors included breastfeeding initiation, frequency and duration, formula supplement, and infant sucking performance.
(1) Breastfeeding initiation, including data of the time from birth to first breastfeeding and the duration of first breastfeeding. Our trained staff nurse recorded the data immediately after the newborns' deliveries. Usually, newborns after vaginal delivery had their first breastfeeding after the umbilical care, physical assessment, wipe dry, and dressing, while the Cesarean babies were not available to the first suck until their mothers were sent back from operation room to obstetric ward.
(2) Duration and frequency of breastfeeding, volume and frequency of formula supplement. Mothers were required to keep a record of the duration and frequency of each breastfeeding and formula supply. Our staff nurse interviewed mothers and recorded the data every 4–6 hours. If the sucking was off and on, we only recorded the sucking duration and took it as one sucking episode, although the newborn's mouth may leave the breast temporarily.
(3) Infant sucking performance. It was evaluated by the Chinese Version of Infant Breastfeeding Assessment Tool (IBAT). 11 It is a 4-item scale that measured the breastfeed from arousability, rooting, fixing, and suckling efficacy. Each item ranged from 0 to 3. Scores correlated positively with infant sucking competence. The inter-rater reliability of this tool is 0.90, test–retest reliability correlation is 0.88, and content validity index is 0.94. Our staff nurse evaluated infant sucking performance once a day.
Breastfeeding outcomes
Breastfeeding outcomes included the breastfeeding methods and maternal perceived milk supply.
(1) Breastfeeding methods were evaluated on the fifth day, and at the first, fourth, and sixth month postpartum. Mothers were required to keep a record of the breastfeeding and formula frequency. Data were collected by our research nurse through telephone interviews. It was evaluated based on a previous 24-hour feeding method in consideration of memory bias. Feeding methods are categorized into seven levels according to WHO definition, 12 including exclusive breastfeeding, predominant breastfeeding, high-level breastfeeding, middle-level breastfeeding, low-level breastfeeding, token breastfeeding, and artificial feeding. Infant feeding methods were evaluated by the frequency of breastfeeds and formula within a 24-hour period (breastfeeding frequency/[breastfeeding frequency + formula frequency] × 100%). Exclusive breastfeeding is defined as a 100% breastfeed. High-level breastfeeding means that >80% feeds are breastfeeds. Middle-level breastfeeding means that 20–80% feeds are breastfeeds. Low-level breastfeeding refers to that <20% feeds are breastfeeds. Token breastfeeding is quantified as <15 minutes of breastfeeding per day, or less than two to three short breastfeeds in a 24-hour period. Artificial feeding means a 100% formula feeding without any breast milk.
(2) Maternal perceived milk supply was assessed by using the Chinese Version of the H&H Lactation Scale. 11 Item was responded to on a 7-point Likert scale with a total score of 140. This scale was designed to evaluate mother's satisfaction with her milk supply from three dimensions, including confidence in breastfeeding, perceived infant breastfeeding satiety, and maternal-infant breastfeeding satisfaction. The overall alpha coefficient ranged from 0.91 to 0.92, and test–retest reliability ranged from 0.68 to 0.90, from 0.67 to 0.89, and from 0.73 to 0.83 for each subscale. Predictive validity achieved 0.42 by assessing the correlations of H&H Lactation Scale to breastfeeding outcomes. This scale was self-evaluated by breastfeeding mothers on the fifth day, and at the first, fourth, and sixth postpartum.
In addition, demographic information was collected through a face to face interview. Prenatal, delivery, and postnatal data were gathered from medical records. Maternal pain was evaluated once a day for the first 3 days by Visual Analogue Scale that ranged from 0 to 10. Maternal fatigue was measured by using the Chinese version of fatigue scale (Fatigue Scale-14, FS-14) 13 on the third day after delivery. FS-14 is a 14-item self-evaluated tool to measure physical and mental fatigue. A higher score indicates a more severe fatigue condition. The Cronbach's α coefficient ranged from 0.88 to 0.90. Its split-half reliability is 0.86. The sensitivity and specificity of this tool are 75.5% and 74.5%. Postnatal depression was screened by the self-report scale, Edinburgh Postnatal Depression Scale (EPDS).
Sample size and statistical analysis
Based on Prior et al., 14 the breastfeeding rate at hospital discharge for vaginal delivery is 73.87%. The odds ratio (OR) for breastfeeding rate associated with CS is 0.57. Two-sided level of significance of 0.05 and power of 0.8 were set. Factoring in a 30% increase in sample size to account for any dropout in the 6-month follow-up, 600 subjects were estimated to be needed.
Two persons were engaged in data entry separately. The input errors were checked by Epidata 3.1. The statistical analysis was made by Stata 20.0. Normal distribution data were expressed as means and standard deviations and analyzed by t test. Nonparametric tests were carried out for non-normally distributed data expressing with median and interquartile range. Multivariate analysis of variance of repeated measuring was adopted for repeated measurements of H&H Lactation Scale and breastfeeding methods. Ordinal cumulative odds logistic regression model was applied to explore the adjusted and unadjusted ORs for breastfeeding rates associated with CS. Early breastfeeding behaviors, including breastfeeding initiation, frequency, and duration, IBAT score, and formula frequency and volume, were adjusted at both the individual and group level.
Results
Mother and infant characteristics
Of the 1,861 evaluated mother-infant dyads, 703 were eligible. Fifty-five mothers (7.82%) refused to take part in this study. No difference was found in baseline information between the recipients and those who declined: age (t = −0.38, p = 0.706), nationality (χ2 = 1.04, p = 0.309), education (χ2 =1.48, p = 0.830), and employment (χ2 = 0.12, p = 0.729).
Among the 648 enrolled, 315 mothers delivered vaginally and 333 of them gave birth by CS. There were 27 mothers (4.17%) who dropped out at the first month postpartum, 33 mothers (5.09%) at the fourth month, and 39 mothers (6.02%) at the sixth month (Fig. 1). No difference (first month χ2 = 2.63, p = 0.11; fourth month χ2 = 0.10, p = 0.75; and sixth month χ2 = 0.06, p = 0.81) existed in the missing numbers between vaginal delivery and CS.
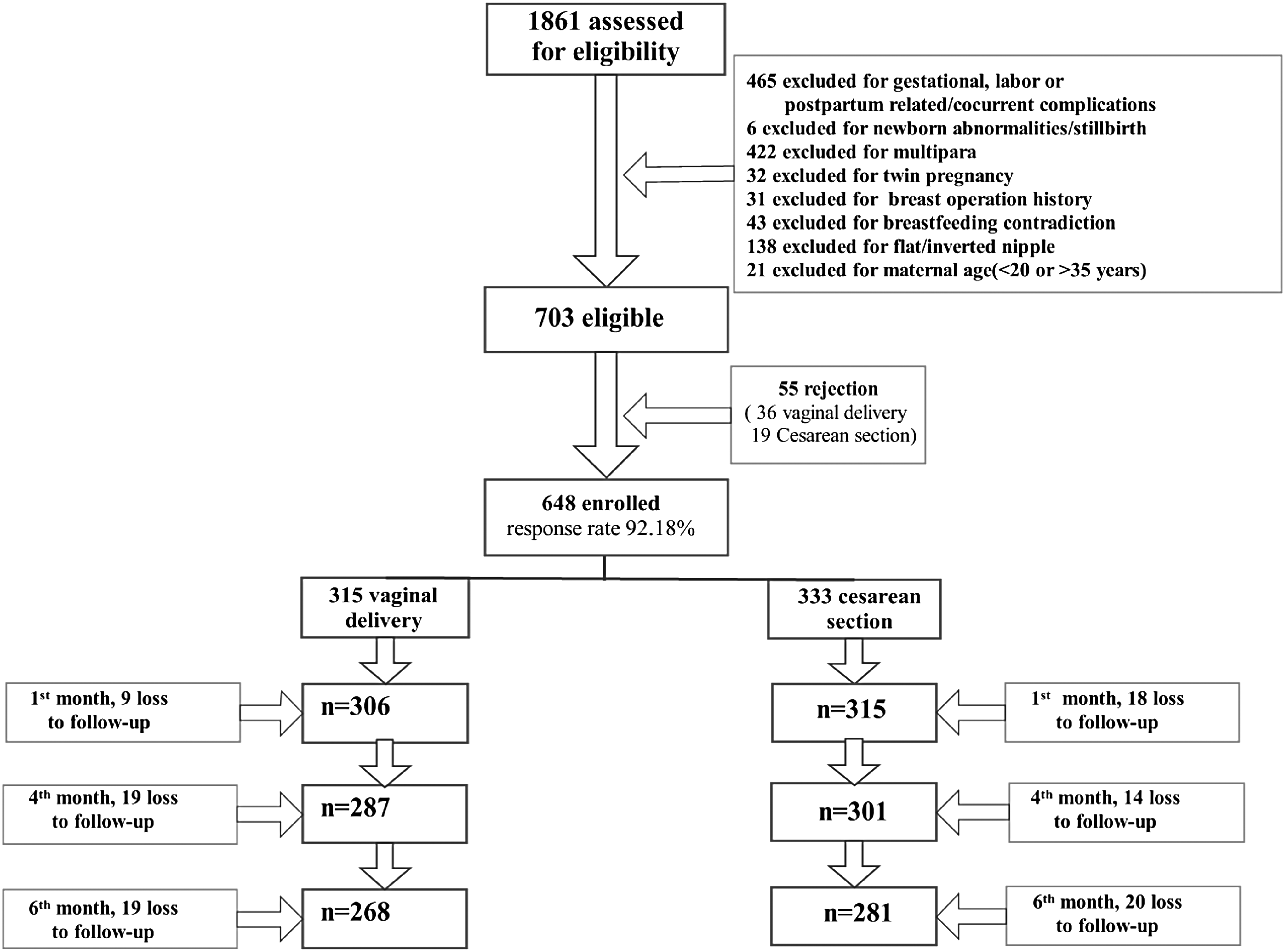
Flowchart of participants from eligibility to data analysis.
Women who experienced Cesarean birth were older (p = 0.02), in a higher economic status (p = 0.04), with more antenatal care interviews (p = 0.00), more overweight (p =0.00), and with heavier newborn birth weight (p = 0.00) (Table 1). In addition, mothers after CS experienced more severe pain (p = 0.00) and fatigue (p = 0.00), longer postpartum hospital stay (p = 0.00), and higher EPDS score (p = 0.00) (Table 2).
Demographic Characteristics for Mother-Infant Dyads
Note: Underweight, BMI <18.5 kg/m2; normal weight, BMI 18.5–23.9 kg/m2; and overweight, BMI 24–26.9 kg/m2. Women with obese BMI ≥27 kg/m2 were exclusion criteria because they may fail in lactation.
BMI, body mass index; CS, Cesarean section; CNY, Chinese Yuan; SD, standard deviation.
Intrapartum Factors That Influence Early Feeding Behavior
Note: Maternal pain score was data of repeated measurement data. Others refer to oral medication or muscular injection of analgesics.
CSE, combined spinal-epidural analgesia; EPDS, Edinburgh Postnatal Depression Scale; M, median; PCEA, Patient Controlled Epidural Analgesia; PCIA, Patient Controlled Intravenous Analgesia; Q, interquartile range.
Early breastfeeding behaviors
For infant after vaginal delivery, the average time from birth to first breastfeeding is 40.91 minutes, while the first suck was delayed to 74.54 minutes for Cesarean newborn. The duration of the first breastfeeding was maintained for 18.33 minutes for babies after vaginal delivery and 14.98 minutes for those after CS (p = 0.00). Although the difference in breastfeeding frequency did not achieve statistical significance (p = 0.11), newborns after vaginal delivery maintained a longer sucking duration for the first (p = 0.000) and second (p = 0.008) day postpartum. Correspondingly, Cesarean newborns were more frequently (p = 0.000) supplied with formula, and they consumed more volumes (p = 0.000) of formula within the first 72 hours after birth. Although infant sucking performance (IBAT scores) improved as time goes by, the Cesarean newborn gained a relatively lower IBAT score compared with that after normal birth (Table 3).
Outcomes of Early Feeding Behaviors
Note: Sucking frequency, sucking duration, formula frequency, formula volume, and IBAT score were repeated measurement data.
BF, breastfeeding; IBAT, Infant Breastfeeding Assessment Tool.
Long-term breastfeeding outcomes
The exclusive breastfeeding rate was 54.92% at discharge (fifth day after birth), and reached its peak point at the first month (65.03%), and then decreased to 47.39% and 25.37% at fourth and sixth month for mothers delivered vaginally. Without exception, the rates were much lower in the Cesarean group (35.74%, 40.32%, 32.22%, and 17.79%, respectively) at all measuring points. Correspondingly, a similar result was achieved in maternal perceived milk supply (H&H Lactation Scale) (Fig. 2).

Exclusive breastfeeding rate and scores of H&H Lactation Scale for mothers after vaginal delivery or CS. Note: Numbers of mothers in analysis: onset of lactation (vaginal delivery n = 315, CS n = 333); first month postpartum (vaginal delivery n = 306, CS n = 315); fourth month postpartum (vaginal delivery n = 287, CS n = 301); sixth month postpartum (vaginal delivery n = 268, CS n = 281). CS, Cesarean section.
Effect of early feeding behaviors on long-term breastfeeding outcomes
The unadjusted ORs for lower breastfeeding rates associated with CS were 2.11 (95% CI: 1.58–2.81), 2.67 (95% CI: 1.96–3.63), 1.60 (95% CI: 1.19–2.15), and 1.36 (95% CI: 1.01–1.83) on the fifth day, and at the first, fourth, and sixth month. The most predominant difference existed at the first month.
To further explore the role of specific early feeding behaviors in long-term breastfeeding rates, we controlled the variant of time from birth to first breastfeeding in model 1, duration of first breastfeeding in model 2, breastfeeding frequency in model 3, breastfeeding duration in model 4, IBAT score in model 5, formula frequency in model 6, formula volume in model 7, and all the 7 variables (time from birth to first breastfeeding, duration of first breastfeeding, breastfeeding frequency, breastfeeding duration, IBAT score, formula frequency, and formula volume) in model 8.
Interestingly, after adjusting for the early breastfeeding behaviors, the negative effect of CS on long-term breastfeeding was attenuated (model 1–7), and was no longer significant on the fifth day (OR: 1.01, 95% CI: 0.70–1.47), and at fourth (OR: 1.13, 95% CI: 0.79–1.62) and sixth month (OR: 0.81, 95% CI: 0.56–1.17) (model 8). Instead, breastfeeding frequency, breastfeeding duration, IBAT score, formula frequency, and formula volume were contributed to 6-month breastfeeding outcomes by multivariate regression (Table 4).
Odds Ratios for Breastfeeding Outcomes Associated with Cesarean Section in 6-Month Follow-Up
Note: Ordinal cumulative odds logistic regression method was applied for ranked data of breastfeeding methods.
CI, confidence interval; model 1, adjusted for time from birth to first BF; model 2, adjusted for duration of first BF; model 3, adjusted for BF frequency; model 4, adjusted for BF duration; model 5, adjusted for IBAT score; model 6, adjusted for formula frequency; model 7, adjusted for formula volume; model 8, adjusted for time from birth to first BF, duration of first BF, BF frequency, BF duration, IBAT score, formula frequency, and formula volume; OR, odds ratio.
Discussion
In this research, we determined the effect size of CS on long-term breastfeeding outcomes, and the role of specific early breastfeeding behaviors in infants born after CS and long-term breastfeeding rates. A major finding is that CS per se is not a negative factor, but rather those infants who have feeding difficulties in the immediate postpartum period have long-term problems.
CS is an acknowledged risk factor for breastfeeding. This point has been widely reported.3,15 Differently, we found that the effect of CS on long-term breastfeeding was attenuated and no longer statistically after adjusting for early breastfeeding behaviors. CS infants are at 1.67 times greater risk for nonexclusive breastfeeding at 1 month by bivariate analysis. The risk decreased from 2.65 times to 1.83 times when the variables of breastfeeding initiation, IBAT scores, breastfeeding duration, frequency, and formula supplement were adjusted. A similar decrease revealed in the adjusted ORs for lower breastfeeding rates associated with CS from data of the fifth day, and fourth and sixth month follow-up, and thus, the CS was no longer a risk factor to breastfeeding.
To our knowledge, few articles have reported this point. Although no direct evidence has proven the effectiveness of optimal breastfeeding behaviors at early stage for CS newborn to improve long-term breastfeeding outcome, numerous articles have mentioned the importance of early breastfeeding.16,17 Early and frequent suck is recommended as guideline worldwide. Restriction on early formula supplement promotes breastfeeding effectively. 18
Plenty of articles have reported the phenomenon that CS shortened the breastfeeding duration 15 or decreased the exclusivity. 19 Our results implied that the unsatisfied early breastfeeding behaviors may mediate the effect of CS on long-term breastfeeding. That is, CS adversely affects long-term breastfeeding primarily by jeopardizing the early breastfeeding behavior.
CS impairs early breastfeeding activity. A wide range of routine care after CS has become an impediment to breastfeeding. 20 The first breastfeeding of infants whose mother experienced CS was delayed to 74.54 minutes in this research. Evidence has supported the necessity of breastfeeding initiation within 1 hour after birth. 21 CS infants often miss the optimal opportunity of sucking reflex. 22
In addition, drug residues damage the coordination of infant sucking movement, 23 and in turn, lead to a delayed onset of lactation. 24 In our research, 55.45% CS mothers received epidural anesthesia, and 45.65% used patient-controlled epidural analgesia. Newborns under the exposure of anesthesia residues were not able to maintain sufficient sucking stimulation (p = 0.00). Instead, they consumed more time in arousing, rooting, and fixing. The whole suckling was on and off. Maternal pain and fatigue status may be another reason leading to mothers' decreased breastfeeding activity. 25 However, sufficient sucking stimulation on breasts is essential for prolactin secretion and lactation.
Another explanation is that women who chose CS tend to use more formula, and then prematurely abandon exclusive breastfeeding. The formula supplement is a significant factor affecting lactation, which accounts for 23.1% of the decrease of milk production. 26 Human's nipples have greater extensibility and deformability than silicone teats under ultrasound imaging. 27 Infants reveal abnormal tongue movements when silicone nipple is given to them in formula supplement. Therefore, it is the suboptimal early feeding behavior after CS that leads to adverse breastfeeding outcomes.
These findings implicated that early breastfeeding behavior can be an attractive candidate providing an opportunity to develop strategies to boost long-term breastfeeding. Supports aimed at early feeding behaviors are necessary and may be effective for Cesarean mothers to improve long-term breastfeeding. Especially during the key points of the first several days in the hospital, nursing care, including early initiation of breastfeeding, sufficient sucking stimulation, correct sucking technique and restriction of formula supplement, is recommended as routines for CS populations.
Our research provided new information about the risks of breastfeeding that connected to CS and the role of early breastfeeding behavior in CS population. Previous researchers have demonstrated the disadvantages of CS in breastfeeding from short and long terms. Experts claimed to prohibit unnecessary CS without medical indications. Our findings gave insight for interventions to those after inevitable CS. More attention should focus on those infants who have problems in early feeding behaviors. This should serve as an incentive to appropriately modify the health practices and policies for mother-infant dyads after CS so as to minimize the anticipated problems in breastfeeding.
Limitation
However, this observational study design limited the ability to determine the directionality between the early sucking behaviors and long-term breastfeeding outcomes. Future randomized controlled studies deserve to explore their causal effect. In addition, 69.44% of the enrolled infants were fed with formula at least once during the first 3 days in our research. Formula supplement may disturb infant sucking pattern and breastfeeding outcomes. Therefore, our results may not apply to infants without formula supplement during the early stage of breastfeeding.
Conclusions
CS exerted an adverse effect on early breastfeeding behaviors and long-term breastfeeding. The effect of CS on long-term breastfeeding was attenuated and no longer significant after controlling the early breastfeeding behaviors. It is implicated that the early feeding behavior may mediate the negative effect of CS on long-term breastfeeding. This finding suggested that clinicians should pay more attention to newborns' early feeding behaviors after CS and provide early breastfeeding support to promote long-term breastfeeding.
Footnotes
Acknowledgments
We thank the midwives, babies, and nurses in the Affiliated Hospital of Nantong University, the People's Hospital of Nantong City, and Maternal and Children Health Care Service Hospital for their contributions, National Natural Science Foundation of China (NSFC, No.81701425), and Natural Science Foundation of the Jiangsu Higher Education Institutions of China (No. 17KJB320009).
Authors' Contributions
F.Z. conceptualized the research questions, conducted data collection and statistical analyses, drafted the initial and revised articles, and approved the final article as submitted. J.C., S.Y., H.W., and T.B., helped the research design, collected and input the data, conducted statistical analyses, helped draft the initial article, and approved the final article as submitted.
Disclosure Statement
The authors declare that they have no conflicts of interest.