
Abstract
Abstract
Objective:
Few clinical reports have addressed the use of the antihypertensive drug amlodipine during breastfeeding. The objective of this study is to characterize concentration-time profiles of amlodipine in maternal and infant plasma, and milk.
Materials and Methods:
Plasma and breast milk samples were obtained from eight nursing mothers and their nine newborn nursing infants (median postnatal age: 6.5 days, range 5–7 days). Participants were recruited from February 2009 to June 2009. Multiple blood and milk samples were obtained from the mothers over a 24 hours dosing interval. The blood of infants was also obtained at before and 8 hours after nursing. Amlodipine concentrations were determined by high-performance liquid chromatography. Relative infant dose (RID) was calculated by dividing the infant's dose via milk in mg/kg/day by the maternal dose in mg/kg/day, assuming that a daily intake of milk is 150 mL/kg/day in the infants.
Results:
Maximal amlodipine concentrations in mothers ranged from 4.4 to 14.7 ng/mL in plasma, and 6.5 to 19.7 ng/mL in milk (Average milk/plasma ratio: 1.4). RID was 3.4% of the maternal weight-adjusted dose. All plasma concentrations in infants were under the quantitation limit (0.4 ng/mL).
Conclusion:
Infant exposure to amlodipine in breast milk appears very small, suggesting that amlodipine can be used with little influence on infants during breastfeeding.
Introduction
P
Methyldopa and hydralazine have been commonly used in nursing women, due to the availability of clinical data about their concentrations in breast milk,4–7 long experience of clinical use, and recommendations from various authoritative bodies. 8 Both medications are used only rarely as antihypertension drugs in nonpregnant adults because they confer insufficient antihypertensive effect, require relatively frequent dosing, and result in multiple side effects.9,10 Moreover, methyldopa is problematic to use in the postpartum period because it has side effects such as sleepiness and depression.10,11 Long-acting antihypertensive drugs, which cause little fluctuation in blood pressure and few side effects, are commonly used in general practice. Amlodipine, one of the commonest antihypertensive drugs in Japan, has fewer side effects and a longer half-life (31–37 hours) than most antihypertensives,12,13 enabling once-daily dosing. However, little information is available regarding its secretion into breast milk.14–17 In this study, we characterized concentration-time profiles of amlodipine in maternal plasma and milk over a 24 hours dosing interval. In parallel, we assessed infant plasma levels of the drug.
Materials and Methods
Subjects of research
The Ethics Committees of the National Center for Child Health and Development and the National Institute of Health Sciences approved this study. Participants were recruited from February 2009 to June 2009. Written informed consent was obtained from all parents. Subjects included mothers, who took amlodipine during breastfeeding and had no complications other than hypertensive disorders, and their nursing infants. There were no restrictions on breastfeeding to infants during this study. Infants were examined by a neonatologist at day 1 and 5 of life. Neuromotor developments of all infants were followed by a neonatologist on a regular schedule until the age of 18 months.
Sample collection schedule
Five milliliters of heparinized blood samples and 5–10 mL of foremilk were collected from mothers at 5–7 days postpartum. Sampling schedules were defined based on the time to maximum concentration in healthy adults (8 hours) and mother's schedules as follows: 0, 2, 4, 8, 12, and 24 hours postdose (n = 3); 0, 4, 8, and 24 hours postdose (n = 2); or 0 and 8 hours postdose (n = 3). Two mL of heparinized whole blood samples were obtained at before and 8 hours after nursing from infants, who received breast milk obtained from their mother 8 hours after oral amlodipine administration. Separated plasma and milk were stored at −80°C until analysis.
Materials
Amlodipine besylate and diphenhydramine were obtained from LKT Laboratory (St. Paul, MN) and Sigma-Aldrich (St. Louis, MO), respectively. Acetonitrile for liquid chromatography-mass spectrometry (Wako Pure Chemical Industries, Osaka, Japan) and ultrapure water produced on a Milli-Q Integral 3 (Merck Millipore, Billerica) were used as the mobile phase of high-performance liquid chromatography. All other chemicals were of the highest grade available.
Analysis of amlodipine in plasma and milk
Concentrations of amlodipine in plasma and milk were determined as reported by Okabe and Sataka and Massarotti et al. with slight modifications.18,19 In brief, 300 μL of plasma or milk was dispensed in tubes, to which 50 μL of water and 20 ng/mL diphenhydramine solution were added, followed by vortex mixing. To the mixture, 200 μL of 1 M sodium hydroxide and 100 μL of saturated sodium hydrochloride solution were added, and the mixture was again vortex-mixed. Then, 5 mL of ethyl acetate/hexane mixture (4:1, v/v) was added to tubes, and amlodipine and diphenhydramine were extracted to the organic phase by shaking at 150/minutes for 15 minutes. After centrifugation at 1,400 g for 20 min at 4°C, the upper phase was transferred to new tubes, and then evaporated to dryness under a nitrogen stream at 40°C. The residue was dissolved in 0.1 mL of mobile phase, and the solution was filtered through Durapore PVDF 0.1 μm (Merck Millipore). Twenty microliters were loaded onto an HPLC system (HP 1100 model) with ESI-MS (G1946D) detection. The chromatographic conditions were as follows: column, PC HILIC (4.6 × 100 mm; Shiseido, Tokyo, Japan) with a CAPCELL C18MG S-5 guard cartridge (4.0 mm i.d. × 20 mm) (Shiseido); column temperature, 40°C; mobile phase, 1 mM ammonium acetate (pH 5.0); acetonitrile (10:90); flow rate, 0.5 mL/min; ESI-MS; and m/z, 238 for amlodipine and 256 for diphenhydramine. The lower limit of quantitation (LLOQ) of this method was 0.4 ng/mL, and its intermediate precisions at 2, 5.5, and 20 ng/mL were 9.9%, 12.9%, and 7.7%, respectively, both in milk and plasma.
Calculation of milk plasma ratio and relative infant dose
We calculated the milk to plasma (MP) ratio of amlodipine based on area under the concentration-time curve in five cases, for whom milk and blood samples were obtained at more than four time points. Relative infant dose (RID) of amlodipine was calculated by dividing the infant's dose via milk in mg/kg/day by the maternal dose in mg/kg/day, using the maximum amlodipine concentration in milk and assuming a daily milk intake in infants 150 mL/kg/day.
Results
Patient characteristics
The eight nursing mothers (mean age: 33.9 years; range: 23–43 years), who received amlodipine (5 mg/day: n = 7; 2.5 mg/day: n = 1) during breastfeeding, and their nine newborn infants (median postnatal age: 6.5 days, range 5–7 days), including a pair of twins, were included in this study. Six mothers received amlodipine from 1 or 2 days postpartum and two mothers from first trimester in their pregnancy (Table 1). One mother had preeclampsia and two had gestational hypertension. Remaining five mothers had chronic hypertension (essential hypertension) before pregnancy, and two had proteinuria with superimposed preeclampsia. Mean systolic and diastolic blood pressures at the beginning of amlodipine treatment were 156 mmHg (range: 144–177 mmHg) and 89 mmHg (range: 80–100 mmHg), respectively. Two subjects started amlodipine therapy during pregnancy, and six started 1–2 days postpartum. Blood pressure was normalized by 3–4 days postpartum in all eight mothers, and there were no significant adverse effects.
M/P ratio: milk/plasma concentration ratio calculated from area under the curve in cases for which samples were obtained at more than four time points.
Cases 2 and 5 are monochorionic diamniotic twins; case 7 is a dichorionic diamniotic twin.
RID, relative infant dose.
Mean weights and gestational ages of the babies were 2,251 g (range: 1,692–3,041 g) and 36.1 weeks (range: 32–40 weeks), respectively. All infants were exclusively breastfeeding at the time of sample collection. All babies had stable vital signs and developed normally until the age of 18 months.
Plasma and milk concentrations of amlodipine in nursing mothers
The concentration-time curves of amlodipine in plasma and milk of five mothers with four or more data points are shown in Figure 1. Amlodipine concentrations reached a peak at about 4–8 hours postdose in plasma and 8 hour in milk. Maximal amlodipine concentrations ranged from 4.4 to 14.7 ng/mL and 6.5 to 19.7 ng/mL in plasma and milk, respectively. Average MP ratio was 1.38 (range, 0.89–2.29) (Table 1).
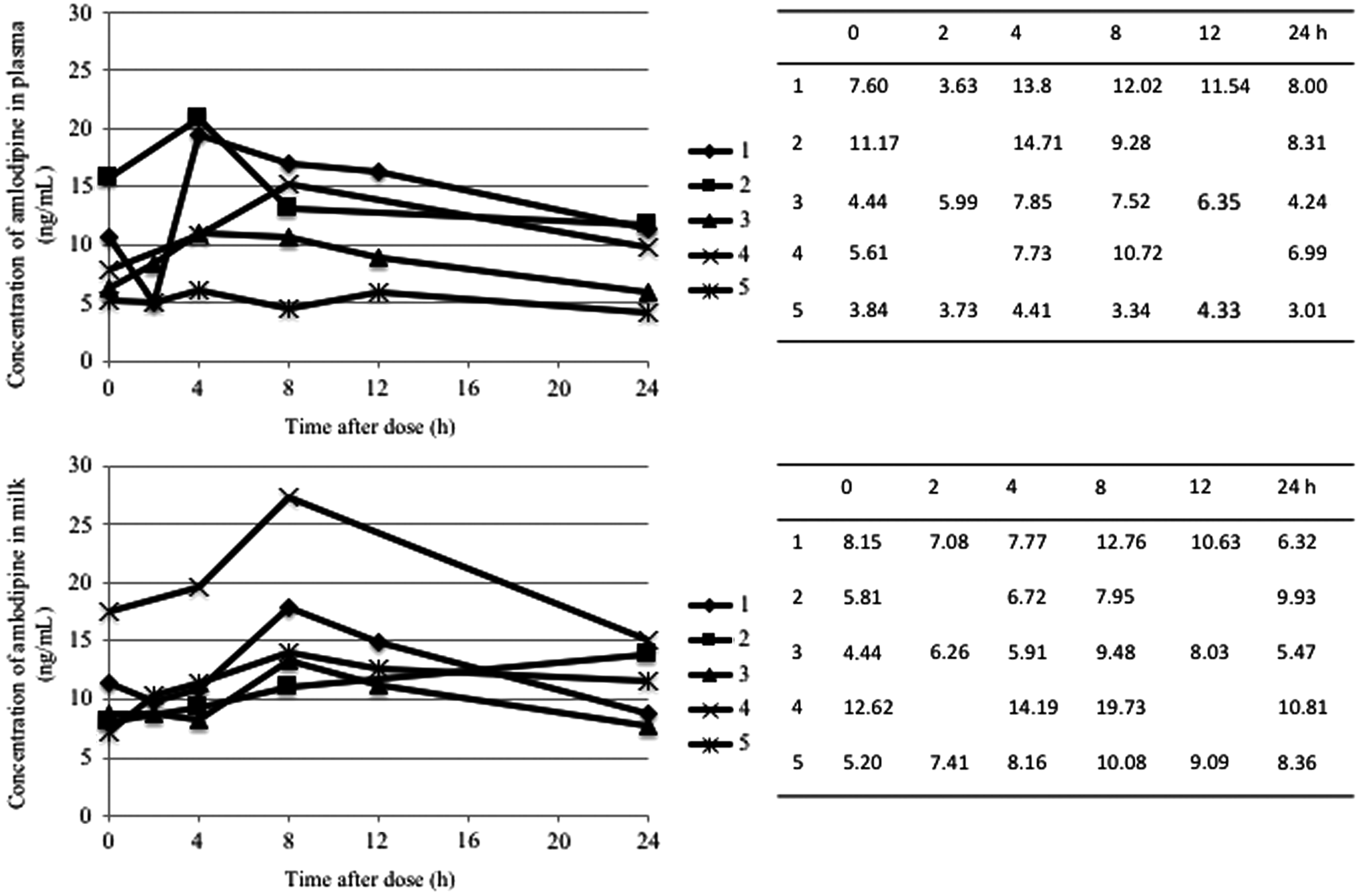
Plasma and milk concentration-time profiles of amlodipine in nursing mothers (n = 5). Note. Plasma and milk concentration-time curve of amlodipine in cases 1–5, which had samples at more than four time points. Cases 1, 2, 4, and 5 received 5 mg/day of amlodipine and case 3 received 2.5 mg/day of amlodipine.
Plasma amlodipine concentrations in infants and RID
All plasma concentrations in babies were under the LLOQ (0.4 ng/mL), which was lower than 10% of the concentrations in the mothers (Table 2). Average RID calculated using maximum amlodipine concentrations in mothers was 3.4% (range, 1.56 to 4.32%) (Table 1).
ND, lower than lower limit of quantitation (0.4 ng/mL). Case 2 is a twin pregnancy; cases 5 and 7 are each one baby from a set of twins.
Discussion
The RID of amlodipine was less than 10% in this study. Medications with low molecular weight, high pKa, low serum protein binding, and high lipid solubility tend to be excreted easily into breast milk. Calcium channel blockers, including amlodipine, have high lipid solubility. The MP ratio of amlodipine observed in this study was only slightly higher than 1.0, despite the high lipid solubility, which may be due to its very high plasma protein binding. 20 However, it is important to recognize that MP ratio is only an index of drug concentrations in milk relative to maternal plasma (not the maternal dose), and that it does not necessarily reflect the actual amount of drug taken up by infants. By contrast, RID provides estimation of the actual amount of drug received by the baby relative to the maternal dose. In general, a drug exposure through breast milk is considered relatively inconsequential for dose-dependent effects, if the RID is less than 10%. 21 The average RID of amlodipine observed in this study was 3.4% (range, 1.56–4.32%), and no mother showed the higher RID than 10%.
Although RID is a useful indicator of breastfeeding safety, drug may accumulate in the infant despite a low RID because drug clearance in infants, especially in premature infants, is low compared to that in adults. As a concept, the exposure index addresses this crucial point, incorporating the child's clearance, and highlights clinical importance of low drug clearance in infants. 22 For this reason, medicines with high clearance or a short half-life (as a surrogate for high clearance) are usually preferred because they are less prone to accumulation. In this study, the plasma concentrations of amlodipine in nursing infants, including low-birth-weight infants and premature infants, were less than the LLOQ (0.4 ng/mL) in all cases, which were far below its concentrations in their mothers. This result shows that there was no significant accumulation of amlodipine in the plasma of nursing infants. Although amlodipine has a long half-life (31–37 hours), it is due to a large distribution volume but not due to low clearance. 12
There are some limitations in this study. First, we measured the breast milk concentration of amlodipine using foremilk. The concentration of amlodipine is lower in foremilk than in hindmilk because of its lipophilicity. Consequently, it is possible that we underestimated the concentration of amlodipine in breast milk. However, we measured plasma concentration in infants who took breast milk produced at the time to maximum concentration, and it was less than the LLOQ in all cases. Second, our subjects include preterm infants. Although preterm infants potentially have lower drug clearance than full term infants, our results showed that plasma concentration in infants were less than the LLOQ in all cases.
Conclusion
The RID of amlodipine was about 3%, and the blood concentration of amlodipine in infants was under the LLOQ, suggesting that amlodipine can be used with little influence on infants during breastfeeding. Thus, amlodipine has several advantages, including a sufficient antihypertensive effect, long duration of action, and fewer side effects, and probable safety during breastfeeding.
Footnotes
Acknowledgment
This work was supported, in part, by a grant from the Japan Ministry of Health, Labor and Welfare (MHLW) (#H22-Jisedai-Ippan-007). We appreciate Mr. Jun Nishikawa at the National Institute of Health Sciences for his excellent analytical technique.
Disclosure Statement
The authors have no conflicts of interest associated with this manuscript.