
Abstract
Abstract
Background:
Olfactory maturation is essential for successful oral feeding. Previous studies have suggested that olfactory stimulation with maternal breast milk may expedite oral feeding skills in the premature infant; however, the optimal developmental window to utilize this intervention and sex-specific responses to stimuli are largely unknown.
Objectives:
To determine individual responses to olfactory stimulation with mother's own milk (MOM) on feeding outcomes in premature newborns.
Materials and Methods:
Infants born between 28 0/7 and 33 6/7 weeks' gestation (n = 36) were randomized to receive either MOM or water (sham) stimulus during the learning process of oral feeding. Clinical and feeding outcomes were recorded. Statistical analyses examined the effect of stimulation with MOM on feeding outcomes stratified for age and sex.
Results:
Overall, there was no significant difference between sham infants compared with MOM infants in mean postmenstrual age of full oral feeds (sham: 35 5/7 versus MOM 36 0/7; p = 0.37). However, when stratified by gestational age (GA), infants born <31 weeks' gestation who received MOM stimulation learned to feed sooner than controls (p = 0.06), whereas infants born ≥31 weeks' gestation learned to feed later than controls (p = 0.20) with a significant interaction (p = 0.02) between the stimulus (MOM versus sham) and dichotomized GA (<31 versus ≥31 weeks). There were no sex differences in response to olfactory stimulus.
Conclusions:
Infants born <31 weeks' GA who received MOM stimulation learned to feed sooner than control infants and the impact of MOM is significantly different between infants born before or after 31 weeks GA. These data suggest there may be an optimal time in development to utilize maternal breast milk to expedite oral feeding maturation in the premature newborn.
Introduction
The ability to orally feed is a complex developmental milestone requiring integration of the neuromuscular, oral motor, gastrointestinal, and sensory systems.1–4 One of the more studied developmental sensory pathways involved in successful oral feeding is olfaction.5–8 Olfactory genes represent the largest superfamily of genes in humans9,10 and play an essential role in memory, taste, defense, and sensory integration. Human studies have shown that during 28 and 35 weeks' postmenstrual age (PMA), the olfactory system is rapidly maturing, 11 and olfactory stimulation with human milk has been shown to improve a preterm infant's appetitive responses,12–14 that is, sucking and rooting. Furthermore, odorants unique to breast milk allow a premature infant to not only prefer the odor of their own mother's breast milk from that of other mothers, but to also prefer other women's breast milk over formula.15–17 These data suggest that olfaction is essential for feeding maturity, and that timely interventions with olfactory stimulation may improve feeding outcomes in the preterm neonate. However, optimal timing in development to utilize this intervention, as well as potential sex-specific responses to the stimulation, is largely unknown. Obtaining developmental milestones, as well as sex disparities in preterm neonatal outcomes, is well described in the literature.18–22 O'Driscoll et al. recently reported that “gender is an important variable in preterm outcomes and should be considered when designing clinical and experimental research.” 22 The aim of this study was to perform a prospective, randomized trial to further explore developmental time frames and sex-specific responses to olfactory stimulation with maternal breast milk to improve oral feeding outcomes in this at-risk population.
Methods
This is a prospective, placebo-controlled, partially blinded, single-center, randomized pilot study. Institutional Review Board approval was obtained; parents signed informed consent before enrollment. Infants born between 28 0/7 and 33 6/7 weeks' PMA to mothers who planned on breastfeeding in the Tufts Medical Center (Boston, MA) Level IV Newborn Intensive Care Unit (NICU) were approached. Infants were excluded if their mothers were HIV or hepatitis C positive or if an infant had a condition that may impact oral feeding skills (i.e., cleft lip or palate). Once informed consent was obtained, an infant was randomized to receive either olfactory stimulation with mother's own milk (MOM) or a sham intervention with sterile water. Breast milk was obtained from all mothers in the study (≤30 mL), regardless of intervention group, to maintain parental blindness to treatment arm. Mothers provided breast milk through pumping in the first week of an infant's life, after transitioning to milk from colostrum (i.e., transitory or mature milk). Breast milk of mothers' infants who were randomized to the sham intervention was discarded. Approximately 30 mL of breast milk received from mothers whose infants were randomized to receive olfactory stimulation with MOM was immediately placed at 4°C for up to 24 hours before being aliquoted and frozen at −80°C pending use at the bedside.23–27 Breast milk was only obtained at this single time point and used throughout the study. Milk was stored at −80°C for days up to several weeks depending upon duration of stimulus. The volume of milk aliquoted into each 2 mL container ranged from 30 to 50 μL to ensure that there was enough breast milk available for olfactory stimulation for the duration of the trial.
Olfactory stimulation
Olfactory stimulation commenced once enteral feeds had been initiated by the care team. When enteral feeds were initiated, three drops (∼30 μL) of freshly thawed MOM or water (sham) were placed on cotton tipped applicator (Cardinal Health, Sterile Cotton Tipped Applicators, 6′′) by a study coordinator who was unblinded to randomization. The coordinator would soak the tip in the NICU, but away from the bedside, to ensure that parents, nurses, and NICU staff were blinded to the intervention to maintain the integrity of the trial. Maternal breast milk underwent only one freeze–thaw cycle to maintain the odor properties of the milk.23–27 Presoaked cotton tipped applicator was held 1–2 cm from the infant's nose during gavage or oral feeding for one feed per day, 4–6 times per week, for the duration of the feed or the first 15 minutes, whichever occurred first. Infants on noninvasive respiratory support by a mask or nasal cannula had the device removed for the length of the stimulus. If the infant was intolerant to removal of support, the stimulus was forfeited for the day. The stimulus was held at the nares of orally intubated infants; no patient was nasally intubated. This intervention continued until either the infant reached full oral feeds or was transferred to a Level II NICU in the metropolitan area of Boston, MA for convalescent care. Once transferred to an outlying hospital, all olfactory stimuli ceased. Data regarding day of life that full oral feeds was reached and days spent learning to feed were obtained from our Level II nurseries for all transferred infants. A schematic of our methods is given in Figure 1.
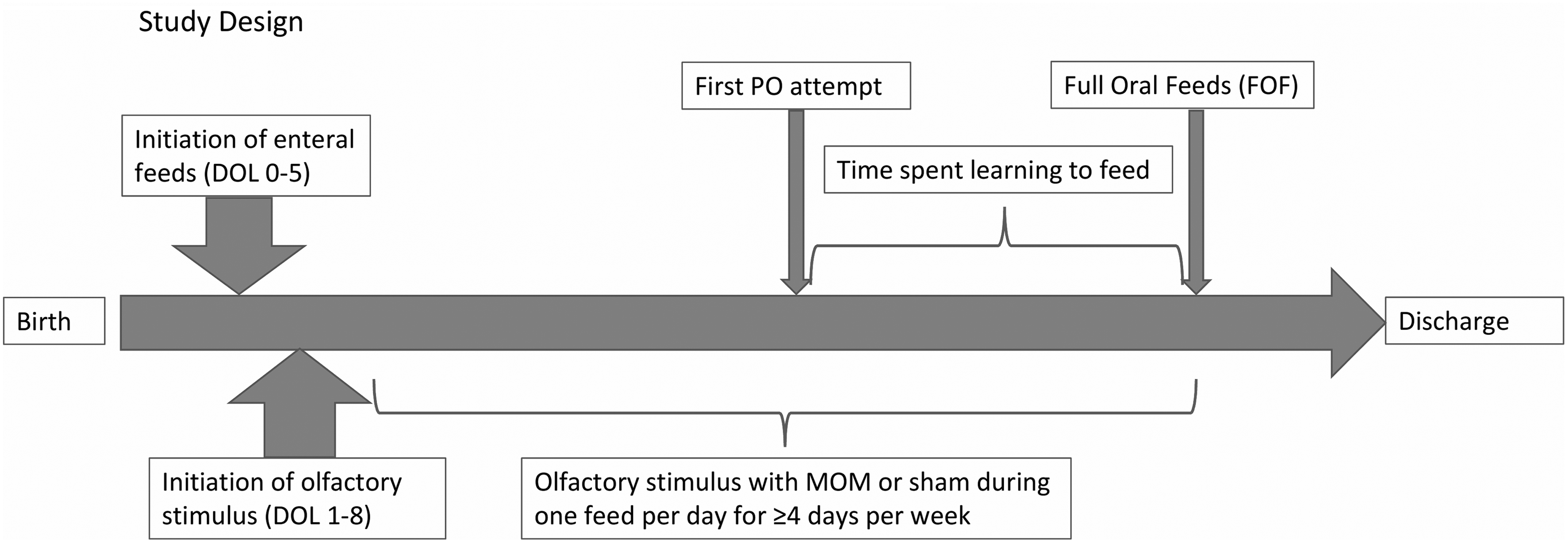
Schematic of study methods. DOL, day of life; MOM, mother's own milk.
Clinical assessment
Pertinent information regarding feeding outcomes including the PMA at initiation of oral feeding trials, PMA at achievement of full oral feeds, and PMA at discharge were recorded for all enrolled subjects (Table 1). Tufts Medical Center NICU and its affiliates used the infant-driven feeding protocol described by Ludwig and Watizman. 28 Nurses are required to begin assessing and recording infant feeding cues at 33 weeks' PMA in a standardized manner to best determine when an infant may begin oral feeding trials. All scores are recorded as part of daily vital statistics. Infants who demonstrated feeding scores of 1 or 2 consistently for a 24-hour period were allowed to begin oral feeding trials. The day of life for oral feeding success was defined as either the day the nasogastric tube was removed or the day the infant sustained full oral feeds for 24 hours, whichever occurred first.
Pertinent Feeding Information for All Subjects (n = 33)
GA, gestational age; MOM, mother's own milk; PO, per os; DOL, day of life.
Statistical analysis
Two-sample t tests and chi-square tests were performed between mean values for the primary outcomes between MOM and sham infants. A two-factor analysis of variance (ANOVA) was used to test the interaction of the intervention and GA dichotomized as less than versus at least 31 weeks. Statistical significance was set at p ≤ 0.05. Kaplan–Meier plots were used to display the pattern of oral feeding over time.
Results
Clinical outcomes
Thirty-six babies were enrolled. One infant was withdrawn because of parental request and another was withdrawn because the mother was unable to provide the requisite MOM sample. One additional baby was removed from the clinical analysis because of a significant patent ductus arteriosus that prohibited oral feeding trials owing to a dependence upon continuous positive airway pressure until surgical repair at 38 weeks' PMA. Of the 33 babies evaluated for clinical outcomes, 17 (52%) were female infants and 17 (52%) received MOM olfactory stimulation (Table 1). Fifteen (45%) infants were <31 0/7 weeks' GA (Table 2). Eighteen (55%) infants were ≥31 weeks' GA (Table 3). There were no differences in illness profiles between groups (Supplementary Table S1). Enteral feeds commenced in study patients between day of life 0–5; stimulus was initiated between day of life 1 and 8. The number of stimulations in all subjects ranged from 2 to 40 (mean = 13.8). Variation in stimulation was directly related to time spent in the Tufts Medical Center NICU. Only 9 of 36 infants originally enrolled in the study reached full oral feeds at Tufts Medical Center. The remaining infants were transferred out to nine community Level II NICUs in the metropolitan Boston, MA area before attainment of full oral feeds.
Pertinent Feeding Information for Infants <31 Weeks' Gestation (n = 15)
Pertinent Feeding Information for all Infants ≥31 Weeks' Gestation (n = 18)
Clinical outcomes
Overall, the mean PMA for achievement of full oral feeds was 35 5/7 weeks in the sham group and 36 0/7 weeks in the MOM group (p = 0.36). There was no difference in the number of days required to learn to orally feed between groups (13 sham versus 13.3 MOM; p = 0.88). Female and male infants acquired full oral feeds at similar average PMAs (female infants: 35 5/7 sham versus 35 6/7 MOM; p = 0.99; male infants: 35 4/7 sham versus 36 2/7 MOM; p = 0.24). Comparisons of sexes within each treatment group showed similar results (sham: female versus male infants; p = 0.75; MOM: female versus male infants, p = 0.33).
The group was evaluated in two cohorts divided based upon their gestational age: GA, 28 0/7–30 6/7 (younger) versus 31 0/7–33 6/7 (older). In the older cohort, the average PMA of full oral feeds in the subjects exposed to MOM was 36 2/7; the average PMA of full oral feeds in subjects exposed to sham was 35 1/7 (p = 0.01). In the younger cohort, the average PMA of full oral feeds was earlier in the MOM group, 35 5/7 versus 36 4/7 in the sham group, although it failed to reach significance. (p = 0.19). However, there was a significant reduction in day of life at attainment of full oral feeds in the younger age group compared with the older age group for those subjects given MOM olfactory stimulation (p = 0.08, two-pair comparison p = 0.0002) (Fig. 2). Among the younger infants, there was a reduction in day of life of attainment of full oral feeds in MOM versus sham infants (mean = 41 versus 49 days, p = 0.06). In the older infants the mean day of life of attainment of full oral feeds was longer in the MOM versus sham infants (mean = 31 versus 25, p = 0.19 days). The impact of MOM versus sham was significantly different in the younger versus older infants (two-way ANOVA interaction p = 0.02).

Kaplan–Meier analysis exploring DOL, at attainment of full oral feeds, FOF, based upon GA and stimulation group. GA, gestational age.
Days of learning, as defined as number of days from initiation of oral feeds to achievement of full oral feeds, were compared within each cohort. In the younger babies, the average days of learning in the MOM group was 12.5 versus 16.4 in the sham group (p = 0.22). In the older babies, the average days of learning in the MOM group was 14.1 versus 11.1 in the sham group (p = 0.33). Finally, PMA of discharge was considered. In the older babies, the average PMA of discharge for the MOM exposed babies was 38 1/7, whereas the sham exposed babies were discharged at average PMA 36 6/7 (p = 0.11). In the younger babies, the MOM versus sham average PMA was 38 0/7 versus 38 1/7 (p = 0.89).
Discussion
Despite significant advances in neonatal care, our ability to improve and/or expedite oral feeding maturation in premature neonates remains largely limited. Because achievement of oral feeding maturation is a major determinant of length of stay in the NICU, there is an important opportunity to develop and utilize safe and effective techniques to improve oral feeding skills. Sensory stimulation offers an inexpensive, noninvasive intervention to minimize time spent learning to orally feed. Specific interventions that incorporate parents, such as with the use of maternal breast milk, have the added and important benefit of allowing mothers to have an active and important role in providing care to their premature infants.
Our study is not the first to examine the association between olfactory stimulation with MOM and clinical feeding outcomes in the premature infant.5,6 Previous research has demonstrated that olfactory stimulation with maternal breast milk shortens time to achieve full oral feeds in this population.5,6 However, our study not only validates previous research, but also further advances the field by elucidating key developmental windows where this intervention may prove most beneficial. Our data suggest that infants born <31 weeks' gestation are more receptive to olfactory stimulation than older infants. There is a growing body of literature that supports this finding. Sensory development is an integrated and timed process that impacts alertness, feeding progression, and discharge readiness in the NICU population.29–32 Ontogenetic studies have shown a progression of sensory emergence, with tactile and vestibular senses developing first, olfaction soon after, and auditory and vision later in gestation. 33 Olfactory neuron maturation is believed to occur at ∼29 weeks GA. 34 During gestation, amniotic fluid serves as a powerful chemostimulant of olfactory receptors. 35 Furthermore, recent studies have shown that both amniotic fluid and breast milk share similar molecular and odorous properties, suggesting that in gestation, amniotic fluid serves as primer for successful oral feeding after birth.36–38 Thus, olfactory stimulation with MOM may provide a continuous environment for sensory development in those infants born more prematurely.
Although there is an emerging field of literature identifying sex differences in response to treatment and interventions in newborns,2,39 our study did not identify sex-specific responses to olfactory stimulation. Rather, our study showed a trend toward significance in female infants who received olfactory stimulus with MOM. Prospective studies may be able detect sex-specific differences and further serve as a guide to inform caregivers not only when to use olfactory stimulation but in which patients.
Interestingly, infants born ≥31 weeks gestation learned to feed sooner when exposed to sham stimulus compared with MOM olfactory stimulation. This finding may further support the hypothesis that olfactory stimulation with MOM is only beneficial during certain time frames in development. However, our study is limited by a small sample size that may have directly impacted our findings.
This proof of principle, pilot study is limited by the fact that enrolled subjects were frequently transferred to convalescent care Level II NICUs before the attainment of full oral feeds. As younger infants would have received more interventions before transfer, it is possible the effects we are seeing are not because of a specific developmental window where the intervention is most beneficial, but rather are reflective of total number of interventions received. Future studies will need to be designed to limit this potential confounder. Nevertheless, this study adds to the emerging literature that supports the use of safe, noninvasive, and family-friendly interventions to improve feeding outcomes in the premature neonatal population.
Conclusions
Olfactory stimulation with maternal breast milk is a cost-effective and noninvasive intervention that may expedite oral feeding and improve feeding outcomes, specifically in infants born at <31 weeks' gestation. Male and female infants have similar responses to stimuli. Future studies are warranted to further explore the beneficial effects of olfactory stimulation with MOM and better delineate optimal timeframes in development to utilize this intervention.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.