
Abstract
Abstract
Background:
Breastfeeding is the best source of food for the newborn. In a situation wherein it is not possible to breastfeed a baby, it may be necessary to express milk from the mother's breast using a breast pump. To achieve lactation success before a baby's suckling can ensure the effective extraction of milk, breast pumps must meet specific biomechanical requirements. However, the parameters of the vacuum stimuli by which milk is expressed remain nonoptimized.
Subjects and Methods:
Forty-nine lactating women of 21–30 years of age who volunteered to be included in this study were examined. Women had been lactating and breastfeeding normally for 6–7 days. A new method was developed to compare the amount of milk ejected by vacuum pulses of different amplitudes or duration.
Results:
It was found that for most nursing women, the vacuum stimuli with amplitude of about 190 mm Hg, duration of 0.7 second, and frequency of 1 impulse/s are optimal for removing milk from the breast of a woman.
Conclusions:
Optimization of the amplitude and duration of the vacuum stimuli increased the efficacy of the breast pump.
Introduction
Breastfeeding, owing to its nutritional and immunological aspects, is the best source of food for the newborn. 1 In a situation wherein it is not possible to breastfeed a baby, for example, where the mother has returned to work or is otherwise temporarily separated from her baby, it is necessary for her to express breast milk for storage and use during the period of separation using a breast pump. 2 Breast pumps must meet specific biomechanical requirements. They should (1) effectively mechanically stimulate mechanoreceptors in the areola of the mammary gland for the formation of the milk ejection reflexes and milk secretion in lactating women (2) not damage the mammary gland not to cause pain in women during milk expression, (3) and effectively empty the breasts.
The vacuum breast pumps extract milk from the breast by applying vacuum stimuli on the mammary gland. Vacuum stimuli are also used in breast pumps with compression stimuli. 3 The key to effective milk removal is, therefore, to optimize the parameters of vacuum stimuli. Yet, we may encounter a number of difficulties when interpreting the results of the studies on assessing how the amplitude and duration of vacuum stimuli influence milk removal. In particular, as studies show, physiological and psychological state of the woman can dramatically influence milk ejection in a 24-hour period. 4 Evidently, to assess the difference in the amount of the ejected breast milk, it is necessary to express milk by applying vacuum stimuli of different amplitude or duration during the same session.
Nevertheless, there are some obstacles that are related to the intermittent nature of milk ejection. Mechanical stimulation of the mechanoreceptors of the areola by applying vacuum periodically releases oxytocin from the central nervous system into the bloodstream, which produces periodic increases in intraductal mammary pressure. 5 During breast pumping, as our previous experiments have shown, when the duration of the peaks is equal to 1.5–2 minutes, the internal mammary gland pressure is subject to intermittent changes, so is the amplitude of the peaks and their sequences. Importantly, these parameters are significantly different between women.6,7 Therefore, when expressing milk by applying vacuum stimuli of the same duration or amplitude at the peak intraductal pressure in the mammary gland, the amount of expressed milk tends to be higher than the amount of expressed milk when applying vacuum stimuli of different duration or amplitude when the intraductal pressure reaches its minimum value in the mammary gland. Thus, to minimize the effect of difference in intraductal mammary pressure on the amount of expressed milk, the breast needs to be exposed equally to different vacuum stimuli at all stages of the changes in intraductal pressure.
The primary aim of the article is to develop and apply the method that allows us to reveal the difference in volume of milk expressed by applying vacuum stimuli of different amplitude and duration in relation to changes in intraductal pressure and to determine optimal vacuum strength, and duration of application of vacuum on milk removal during breast expression using a breast pump.
Subjects and Methods
Participants
The study was conducted at the postnatal unit of the D.O. Ott Institute of Obstetrics, Gynecology and Reproductology in St. Petersburg, Russian Federation. Forty-nine lactating women of 21–30 years of age who volunteered to be included in this study were examined. Women had been lactating and breastfeeding normally for 5–6 days. Forty of them were primiparous breastfeeding mothers and nine were multiparous mothers. All infants were born in term. The informed consent of the women was obtained according to the Declaration of Helsinki. The study was approved by the Ethics Committee of the D.O. Ott Institute of Obstetrics, Gynecology and Reproductology, RAN, Russia.
Experimental setup and procedures
Figure 1 shows the experimental system that has a removable cup and a controller.
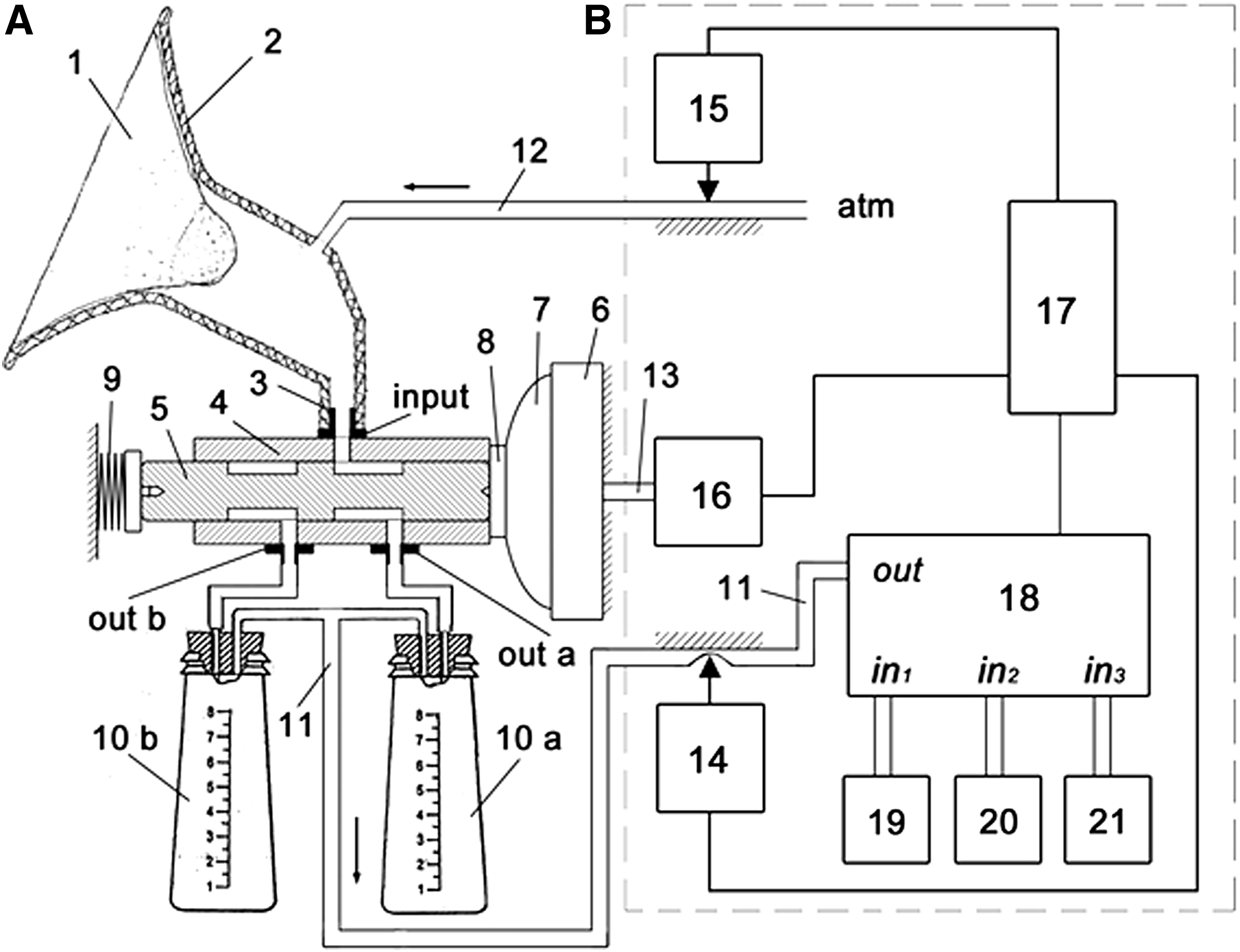
Experimental setup.
The removable cup (Fig. 1A) has a plastic cone-shaped cup (2), a silicone milk collection tube (3), a switch module of the milk collection containers (4), and milk collection containers 10
The switch module of the milk collection containers has a plunger (5) with two grooves that have one side contacted through a rigid disk (8) with a moving membrane (7) that is fixed in the chamber (6) and the other side (5) contacted with a spring (9). The controller (Fig. 1B) includes a generator of electrical control pulses (17), a source of controlled vacuum (19, 20) and noncontrolled vacuum (21), a switch module of the sources of vacuum (18), a positive pressure pulse generator (16), and pinch valves (14, 15). The pneumatic connections between the elements of the controller have a marking of a double line, whereas the electrical connections have a marking of a single line.
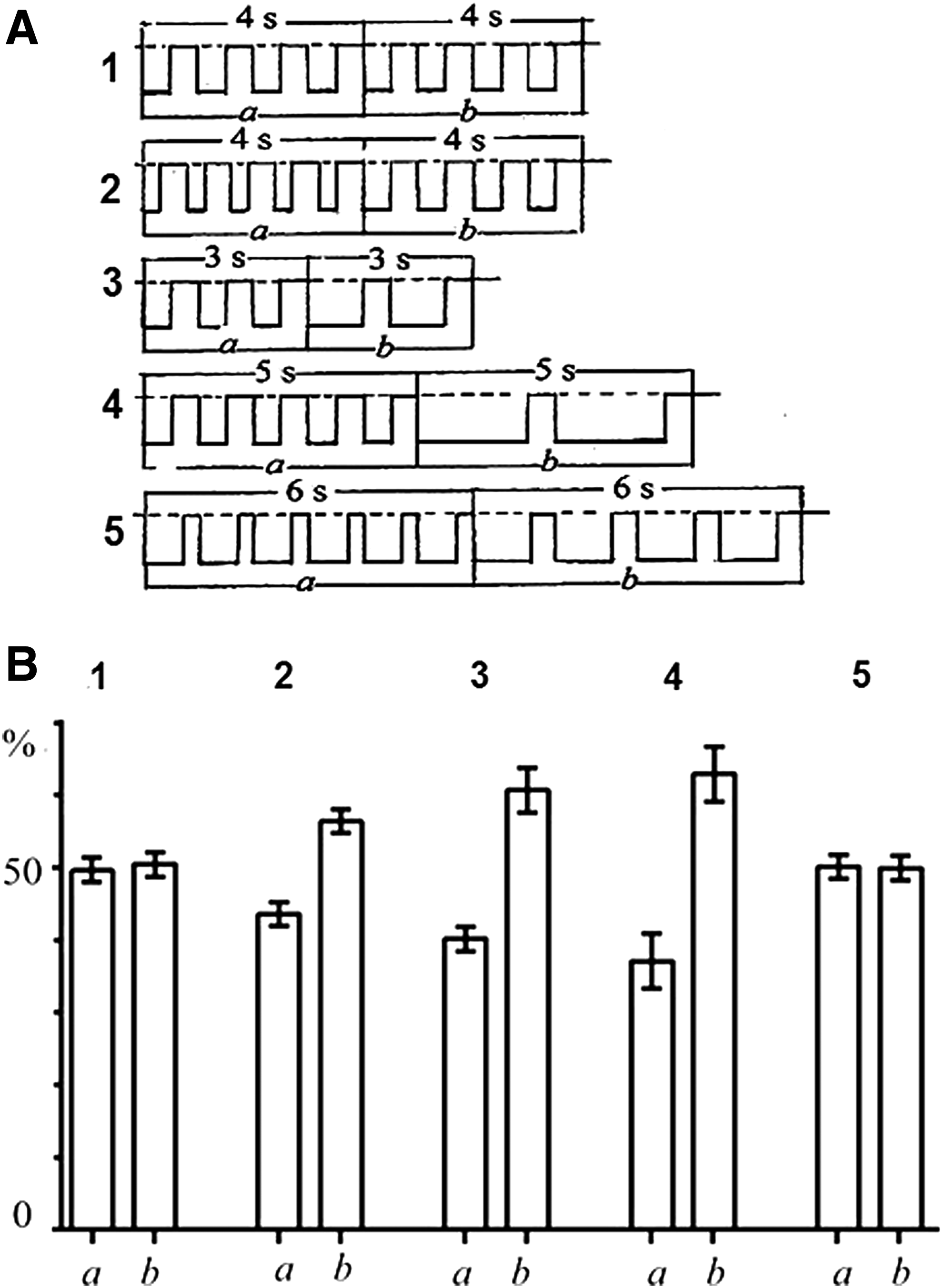
The system works as follows: before the experiment, it is necessary to set an appropriate mode of operation for the generator unit of the electrical pulses (Fig. 1B—17) and define the appropriate values of amplitude and duration of vacuum for the sources of controlled vacuum (Fig. 1B—19, 20). The plastic cone-shaped cup (2) (Fig. 1A) is placed on the mammary gland (1) (Fig.1A). Figure 2A and B shows the cyclograms of the controller. The cyclogram 1 (Fig. 2A) shows the time (numbered cross-hatched rectangles) when the sources of vacuum (19, 20, 21) are connected to the switch module of the sources of vacuum (18) (Fig. 1B). At T1, the pneumatic pulse is transmitted through the hose (13) from the positive pressure pulse generator (16) to the chamber (6) that involves the moving membrane (7) (Fig. 1B) (cyclogram 5, Fig. 2A).

Cyclograms of formation of impulses of vacuum of different amplitude
The duration of the pulse is T1–T3. As a result, the membrane (7) moves the plunger (5) of the switch module of the milk collection containers to the far left position (Fig. 1A) and simultaneously presses the spring (9). When the plunger (5) is in the far left position, the plunger groove (Fig. 1A—on the right) connects the milk collection containers 10
At t2, the hose (11) is punched (marked as a single line), yet the vacuum is still in the closed space: the plastic cone-shaped cup with the nipple and areola (2), silicone milk collection tube (3), plunger grooves and milk collection containers (10
For more accurate collection of milk in the containers, the system, at the end of each session of impulses of vacuum, generates an additional impulse of vacuum. At T2 during T2–T3, we connect an additional source of vacuum (21) to the output of the switch module of the sources of vacuum (18) (Fig. 1B) (cyclogram 1, Fig. 2A). At t15, during t15–t16 (cyclogram 2, Fig. 2A), the hose (11) is opened, as is the hose (12) during T2–t17. The additional impulse of vacuum can slightly increase (up to 20 mm Hg) the vacuum pressure inside the plastic cone-shaped cup (2) (Fig. 1A). It is marked as a crosshatched low-amplitude stimulus in the cyclogram (4) (Fig. 2A). The additional stimulus of vacuum initiates airflow toward the milk collection containers that effectively “pushes” forward the drops of milk from the silicone milk collection tube (3) and plunger groove (Fig. 1A) into the milk collection container 10
At T3, the system stops generating the impulse of excess pressure in the hose (13) (Fig. 1A). The spring (9) (Fig. 1A) of the switch module of the milk collection containers moves the plunger (5) (Fig. 1A) into the far right position for T3–T5 that is equal to T1–T3 and connects the plastic cone-shaped cup (2) and milk collection container (10
During the experiments on assessing how the impulses of vacuum of different duration influence milk collection, the generator of electrical control pulses (Fig. 1B—17) is set for a selected mode of operation. How the system operates in this mode (Fig. 4B) does not differ from how it operates when assessing the role of amplitude of vacuum on milk collection (Fig. 4A). As the amplitude remains the same in a session of vacuum stimuli, we do not use the source of the controlled vacuum (20) at T3–T4 (cyclogram 1, Fig. 4B).
When comparing the parameters of the vacuum stimuli, it is essential to take into consideration the duration of the series of the compared impulses. Ideally, the number of the compared vacuum stimuli should have ratio 1:1. However, after the milk removal by vacuum stimuli is completed, for example, in the milk collection container
The volume of milk per one switch is insignificant, but a large number of vacuum stimuli pass through the entire session and the volume of milk in the milk collection containers may introduce a noticeable error in the results of the experiment. However, if the number of pulses is more than 1 – n stimuli, the volume of milk removed by n – 1 vacuum impulses will remain in the same milk collection container and only the residual milk will switch to another milk collection container when the n-th stimulus is switched. The measurement errors will decrease by about n times. It was decided to set the number of the pulses in the series 4–5. The measurement error, due to the reflex pressure changes in the duct system in the mammary gland, will increase slightly.
If a woman had enough milk, we compared the basic value of the amplitude or duration of the vacuum (the milk collection container
Once the milk collection container has no less than 7–10 mL of milk, the milk removal was stopped. It took 3–5 minutes. In the milk collection containers
Statistical analysis
The study compares the amount of milk ejected by applying basic vacuum and by experimental vacuum. The reliability of differences in the means is tested by the Student's t-test. Statistical significance was set as p < 0.05.
Results and Discussion
Optimizing the amplitude of the impulses of vacuum
The first part of the study examines how the vacuum stimuli of different amplitude influence the amount of expressed milk. The basic stimuli are vacuum stimuli with duration of 0.5 second, frequency of 1 impulse/s, and amplitude of 152 mm Hg. In our experiments, the duration of the rising and declining phases of basic vacuum and experimental stimuli is ∼0.05 second.
To check that the systems are symmetrical, at the beginning of the examination, we collected milk from five women in containers 10
The effect of the vacuum stimuli of different strength on milk expression is shown in Table 1. We compared the amount of milk (Va) expressed by applying the basic vacuum stimuli of amplitude 152 mm Hg to the amount of milk (Vb) expressed by applying experimental vacuum stimuli of amplitude 76 mm Hg. The ratio Va/Vb was 1.9 ± 0.2 (p < 0.05) (Fig. 3A).

The amount of milk in the milk collection containers extracted by vacuum stimuli of different amplitude. The ratio between the amount of milk ejected by the basic vacuum 152 and 76 mm Hg
Effect of Vacuum Stimuli of Different Amplitudes on Milk Expression
Va, milk volume in mL in collection container
The significance of bold values is p < 0.05.
When the vacuum stimuli were equal to 152 and 114 mm Hg, the ratio Va/Vb was 1.3 ± 0.1 (p < 0.05) (Fig. 3B). Consequently, when the vacuum stimuli were equal to 152 and 190 mm Hg (Fig. 3C), the ratio Va/Vb was 0.8 ± 0.04 (p < 0.05). As we can see, the higher the amplitude of the vacuum stimuli is, the more the milk is expressed from the breast (Fig. 3). Nevertheless, the standard deviations were comparatively more in the ratios of the amounts of milk expressed by applying the vacuum stimuli of 152 and 76 mm Hg, yet they were considerably different from those in the ratios of the amount of milk expressed by the vacuum stimuli of 152/114 and 152/190 mm Hg (Fig. 3). These differences can be explained by an increase in intraductal pressure in formation of milk-ejection reflex in response to stimulation of the mechanoreceptors of the areola and nipple of the mammary gland. 5
In particular, when we apply vacuum stimuli of 152 and 76 mm Hg and the intraductal pressure increases, for example, 5 by 15.2 mm Hg, the difference between the pressure in the alveoli and ducts and atmospheric pressure increases as follows: 152 + 15.2 = 167.2 mm Hg or 76 + 15.2 = 91.2 mm Hg. Consequently, the ratio that is equal to 2 between 152 mm Hg and 76 mm Hg decreases to 1.83, which implies the differences in how the expressed milk amounts are related to each other. Importantly, this increase is more likely to affect how the low-amplitude stimuli facilitate milk removal.
However, as our examinations show, an increase in the amplitude up to 228 mm Hg sometimes can cause pain, and consequently pain stress can decrease milk release. 8 Our examinations have shown that the optimal amplitude for most women is 190 mm Hg, which also proves previous studies. 9
Optimization of duration of the stimuli
The second part of our study focuses on how vacuum stimuli of different duration influence milk removal. Effect of the vacuum stimuli of different duration on milk expression is given in Table 2. The vacuum strength for the second part of the study was 152 mm Hg. In our first examination, we collected milk in the container
Effect of vacuum stimuli of different duration on milk ejection.
Effect of Vacuum Stimuli of Different Duration on Milk Expression
Duration of vacuum stimuli in the series: A, 0.5 second; B, 0.3 second; C, 1 second; D, 2 seconds; E, 0.7 second; F, 1.05 seconds. Va, milk volume in mL in collection container
The significance of bold values is p < 0.05.
If the duration of vacuum stimulus was 0.3 second, the ratio between the sum of vacuum stimuli of 0.3 second that was equal to 1.5 seconds and the total duration of a series that was equal to 4 seconds was 0.37 (E = 0.37). The ratio between the sum of forces of vacuum stimuli of 0.5 second that was equal to 2 seconds and the total duration of a series that was equal to 4 seconds was 0.5 (E = 0.5). The amount of milk expressed during one series of vacuum stimuli of 0.5 second (Fig. 4B—2b) was 13% higher than amount of milk expressed during one series of vacuum stimuli of 0.3 second (Fig. 4B—2a) (p < 0.05) (Fig. 4B—2).
Comparing the series of duration of 3 seconds of vacuum stimuli of 0.5 second (Fig. 4A—3a) and the series of duration of 3 seconds of vacuum stimuli of 1 second (Fig. 4A—3b) revealed that the amount of milk expressed by vacuum stimuli of 1 second was ∼20% higher than the amount of milk expressed by vacuum stimuli of 0.5 second (p < 0.05) (Fig. 4B—3), and the total duration of vacuum stimuli of 1 second was 0.5 second higher than the total duration of vacuum stimuli of 0.5 second (Fig. 4A—3). For the duration of stimulus of 0.5 second, E = 0.5, whereas for the stimulus of 1 second, E = 0.67.
Comparing the 5-second series of vacuum stimuli of 0.5 second (Fig. 4A—4a) and the 5-second series of vacuum stimuli of 2 seconds (Fig. 4A—4b) revealed that the amount of milk ejected by applying vacuum of 2 seconds was 25.8% higher than the amount of milk ejected by vacuum of 0.5 second (p < 0.05) (Fig. 4B—4), and the total duration of vacuum stimuli of 2 seconds was 1.5 seconds higher than the total duration of vacuum of 0.5 second (Fig. 4A—4). For vacuum of 0.5 second, E = 0.5, whereas for vacuum of 2 seconds, E = 0.8.
Thus, our study has shown that if E is increasing, the amount of milk removal is also increasing. It can be explained by an increase in the ratio between the duration of vacuum stimuli and the interval between them. The maximum value of E is 1. In other words, E is equal to 1, if the interval between the stimuli is equal to 0 and is exposed to continuous vacuum. We should mention here that the first models of breast pumps were based on permanent vacuum. It could cause pain and lead to a swollen areola and nipple. 2
In our study, when we removed milk by applying vacuum stimuli of 2 seconds, some women experienced pain and swelling in the nipple–areola complex. Although there was no difference in the duration when the vacuum stimuli of 0.3–0.5 and 0.5–1 seconds were applied, the amount of milk removal was considerably different in the latter case (Fig. 4B—3). Yet, if the time difference between the session of vacuum stimuli of 0.5 and 2 seconds was 1.5 seconds, we did not witness an increase in the amount of milk removal when applying the vacuum stimuli of 1 second (Fig. 4B.3). Therefore, we can assume that the ducts, due to their biomechanical properties, are “set” to express milk by the vacuum stimuli of a certain duration.
Presumably, a decrease in efficiency of milk removal by increasing the duration of the vacuum stimuli up to 2 seconds is associated with discomfort and pain in the nipple–areola complex. It can have a negative effect on the central mechanisms of formation of the milk removal reflex and, therefore, decrease the efficiency of milk removal. Our data prove the results of the studies on how the form of vacuum stimuli influences the milk removal. 10 If we apply the vacuum stimuli of different forms and duration and assess them in terms of whether they are comfortable or uncomfortable, the vacuum stimuli of 2–3 seconds in the experimental breast pumps are associated with discomfort. 10 Presumably, if we increase an interval between the stimuli up to 1 second, it could reduce discomfort that is associated with the vacuum stimuli of long duration. Yet, if we apply the vacuum stimuli of 2 seconds with an interval of 0.5 second, E decreases from 0.8 to 0.67, which is the value for the vacuum stimuli of 1 second.
Reducing the duration of vacuum stimuli and increasing their frequency do not seem effective. To sum up, the optimal duration of vacuum is within 1 second. To prove our supposition, we chose the vacuum stimuli of 0.7 second with an interstimulus interval of 0.3 second and the frequency was 1 impulse/s (Fig. 4A—5a). Then we compared the efficiency of the vacuum stimuli of 0.7 second with the vacuum stimuli of 1.05 seconds with an interstimulus interval of 0.45 second and the frequency 0.67 impulse/s (Fig. 4A—5b). The number of the vacuum stimuli of 0.7 second in series was 6, whereas the number of the vacuum stimuli of 1.05 seconds in series was 4. The total duration of the vacuum stimuli of 0.7 second and the total duration of the vacuum stimuli of 1.05 seconds were 4.2 seconds (Fig. 4A.5). The total duration of the series of stimuli was 6 seconds. For the vacuum stimuli of 0.7 second, E = 0.7, whereas for the vacuum stimuli 1.05 seconds, E = 0.66.
The amount of milk expressed by applying the vacuum stimuli of 0.7 second was 50.1% ± 1.8%, whereas the amount of milk expressed by applying the vacuum stimuli of 1.05 seconds was 49.9% ± 1.8% (Fig. 4B.5). No statistically significant evidence was found (p ≥ 0.05). However, the vacuum stimuli of 1.05 seconds were associated with discomfort and swelling in the areola–nipple complex. Thus, our study shows that the optimal duration of the vacuum stimuli is 0.7 second with an interstimulus interval of 0.3 second and frequency of 1 impulse/s.
Conclusions
The research findings show that the vacuum stimuli with amplitude of about 190 mm Hg, duration of 0.7 second, and frequency of 1 impulse/s are optimal for removing milk from the breast of a woman. The method described may be extrapolated to assess the efficacy of the breast pumps of various designs.
Footnotes
Acknowledgments
This research was supported by grant No. 28-12-19-56 Medthechnika, Thula, Russian Federation. We express our thanks to Dr. Irina Lekomtseva for translating this article into English.
Disclosure Statement
No competing financial interests exist.