
Abstract
Abstract
Background:
Although national breastfeeding rates have improved across recent decades, women continue to face barriers to achieving recommended breastfeeding targets. Returning to work presents a unique set of challenges for breastfeeding continuation, even in health care settings tasked with promoting breastfeeding among patients. This study examined the association between key workplace breastfeeding support characteristics, job satisfaction, and breastfeeding outcomes among health care employees.
Materials and Methods:
We used data from a cross-sectional survey of employees in a large integrated health care system. The study sample included female employees who had breastfed in the past 3 years (n = 165). The Employee Perceptions of Breastfeeding Support Questionnaire (EPBS-Q) measured organization, manager, and coworker support for breastfeeding. Regression analyses tested the association between workplace support factors and breastfeeding duration, breastfeeding exclusivity, and job satisfaction.
Results:
Managerial support increased median job satisfaction by 0.39 standard deviations (p < 0.001), and increased the odds of prolonging exclusive breastfeeding (odds ratio [OR] 1.47; confidence interval [CI] 1.03–2.09). Organizational support increased median job satisfaction by 0.27 standard deviations (p < 0.001), and increased the odds of exclusive breastfeeding by nearly twofold (OR 1.80; CI 1.05–3.09). No significant associations were found between workplace support factors (organizational, managerial, and co-worker support) and overall breastfeeding duration.
Conclusions:
Organizational and managerial support are key aspects of workplace lactation support, which may positively impact job satisfaction, rates of exclusive breastfeeding, and duration of exclusive breastfeeding among female health care employees. This intersection of outcomes salient for the business community and public health practitioners highlights opportunities for collaborations to improve workplace and breastfeeding outcomes.
Introduction
Breastfeeding rates in the United States have improved across recent decades. However, women continue to face significant barriers to achieving their breastfeeding goals. Nationally, only 81% of infants are ever breastfed, only 52% of women meet the American Association of Pediatrics' (AAP) recommendations for exclusive breastfeeding for the first 6 months, and less than one-third (31%) of women meet targets for breastfeeding for up to a year. 1 Among women who stop breastfeeding before 1 year, ∼60% of women fail to reach their personal breastfeeding goals for reasons that include problems with lactation and with pumping milk. 2
Returning to work postpartum negatively impacts breastfeeding duration3,4 and intensity. 5 To maintain their milk supply, women working outside of the home need to express milk at regular intervals, while away from their child or have the opportunity to breastfeed during the workday. The lack of a private, comfortable lactation space at work, insufficient break time for milk expression, and absence of a lactation support policy have all been shown to decrease breastfeeding duration among postpartum women.4,6–8 While the 2010 Affordable Care Act provided guidelines to ensure adequate break time for lactating employees, policies within many U.S. organizations do not accommodate the needs of a workforce that is increasingly young and female.
Efforts to engage businesses as partners in support of breastfeeding have benefited from research linking workplace breastfeeding support to better outcomes for employers and employees. Workplace breastfeeding support (e.g., lactation facilities, lactation programs, and break time) is associated with lower absenteeism, 9 lower turnover, 10 higher job satisfaction, improved morale, and a more positive company reputation.11–13 The absence of workplace lactation support is related to perceived negative work interference with personal life, 14 increased stress, and early discontinuation of breastfeeding. 15 In health care settings where women comprise more than 80% of the workforce, studies have reported both low and high levels of support and few studies have examined the impact of different types of workplace breastfeeding supports on outcomes that matter for employers and employees.4,16–18 Understanding the nuances of these relationships has important practical implications for how resource-limited workplaces best provide breastfeeding support, and for strengthening the business case for breastfeeding.
Workplace breastfeeding support can be examined across five major domains: organizational support, managerial support, co-worker support, time, and physical environment.19,20 Waite and Christakis 13 examined the differential impact of the five domains on breastfeeding duration and job satisfaction in two large corporations and found that increased total workplace support score was associated with increased job satisfaction, but not with breastfeeding duration. Increased support scores within each domain were independently associated with increased job satisfaction. When all domains were considered together, different domains were significant between the two companies. The study illuminated the need for additional research on how different types of workplace breastfeeding support impact breastfeeding duration and job satisfaction.
This study replicates three study aims from Waite and Christakis to examine whether their findings hold in a different sample
13
:
To determine if overall perceptions of workplace breastfeeding support are associated with job satisfaction. To examine which domains of breastfeeding support are associated with job satisfaction. To determine if perceptions of workplace breastfeeding support are associated with increased breastfeeding duration.
In addition, our fourth aim was to examine the association between workplace support and exclusive breastfeeding, an area of further inquiry identified by Waite and Christakis. 13 We hypothesized that workplace support would be positively associated with exclusive breastfeeding and exclusive breastfeeding duration.
Materials and Methods
Design
We used data from a cross-sectional survey conducted to assess perceptions of workplace support for breastfeeding among health care employees. The online survey included the 41-item Employee Perceptions of Breastfeeding Support Questionnaire (EPBS-Q) 19 questions exploring breastfeeding practices, participant demographics, job satisfaction, and an open-ended box for participant comments. The Chesapeake Institutional Review Board reviewed this study and classified it as exempt research because it presented minimal risk to participants.
Data collection
The survey was conducted from March to July 2017 at a large integrated health care system, which serves patients at over 900 outpatient and inpatient care locations in North and South Carolina. Survey data were collected anonymously online using Qualtrics. The research team recruited employees through e-mail, intranet postings, and in person at a table set up in two hospital cafeterias. Consent was implied by completion of the survey. Participants received no financial incentive. All survey questions were in English.
Sample
The target population for the survey included adult employees (age ≥18 years) of the health care system, who had been employed for ≥6 months. The study sample included survey respondents who were female and had breastfed in the past 3 years.
Measurement
Outcomes
We examined four outcomes: job satisfaction, overall breastfeeding duration, exclusive breastfeeding, and exclusive breastfeeding duration. Job satisfaction was measured using the following validated, one-item measure of job satisfaction 21 : “Taking everything into consideration, how do you feel about your job as a whole?” Consistent with the Waite and Christakis study, this item was measured using a 7-point Likert scale (1 = extremely dissatisfied and 7 = extremely satisfied). 13 Reliability for the one-item measure of job satisfaction has been reported to be between 0.73 and 0.90 with good concurrent and discriminant validity. 21
The one-item measure also performed as a multiple-item measure of job satisfaction in predicting turnover intention. 21 Overall breastfeeding duration was measured using a single item that asked, “Approximately how long did you actually breastfeed your youngest child? (If you are still breastfeeding, indicate how long you have been breastfeeding.).” Responses were categorized as follows: <6 months, 6–12 months, or >1 year. Exclusive breastfeeding was assessed using the following item: “Did you practice exclusive breastfeeding (i.e., gave baby breast milk only; no use of infant formula)?” Two response choices were provided (yes; no). Exclusive breastfeeding duration was measured by the following question: “Approximately how long did you (or have you) exclusively breastfed?” Responses were categorized as: <4, 4–5, and 6 months.
Workplace breastfeeding support
Workplace breastfeeding support was the independent variable. The 41-item EPBS-Q measures breastfeeding support across 5 domains: organizational support (11 items), managerial support (12 items), co-worker support (6 items), time, and physical environment (12 items). 19 Organizational support captures system-level attributes (e.g., organizational structure, culture, and operations) that shape both availability and access to resources and opportunities for workplace lactation.” Sample questions for the organizational support domain include, “I would be able to get information about combining work and breastfeeding from my company” and “I'm certain there is a place I could go to breastfeed or pump breast milk at work.” Managerial support and co-worker support assess individual-level support (e.g., instrumental, psychological, and social) provided by direct supervisors and workplace associates, respectively. (Sample Question: “My manager would support me breastfeeding or pumping breast milk at work.” and “My co-workers would cover my job duties if I needed time for breastfeeding or pumping breast milk.”). Time refers to the availability of time during an occupational work shift for lactation. (Sample Question: “My breaks are long enough for breastfeeding or pumping breast milk.”). Physical environment measures the availability and adequacy of space and equipment for lactation. (Sample Question: “The designated place for breastfeeding or pumping breast milk at work would be available when I needed it.”). All items are on a 4-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = agree, and 4 = strongly agree), except for four items under the physical environment domain which are on a “1 = no, 2 = not sure, and 3 = yes” scale). Domain-specific scores were obtained by summing Likert responses within each domain. The overall workplace breastfeeding support score was obtained by totaling the domain-specific scores. Content validity of the EPBS-Q was assessed by 10 experts in the field of lactation, as well as, one-on-one interviews with 14 women who had recent experience with breastfeeding while working. 19 The EPBS-Q subscales were correlated at 0.68 and the questionnaire had good internal consistency with an alpha of 0.87 in the original validation study. 20
Data analysis
Linear and quantile regression models were used to examine the association between workplace support and job satisfaction. The relationships between workplace support and both breastfeeding duration and exclusive breastfeeding duration were assessed by fitting an ordinal probit regression model. The association between workplace breastfeeding support and the likelihood of exclusive breastfeeding was examined using a binary logistic regression. All models were adjusted for the following potential confounders: age, race, marital status, education, income, and pay type (salaried or hourly). Workplace breastfeeding support scores were standardized for each domain to allow for comparisons across domains. Analyses were conducted in SPSS 25.0 and Stata 15.
Missing values and imputation
The percentage of missing data ranged from 0% to 44% with most variables missing around 13% of the observations. To maximize the use of information in the data and minimize bias due to missing data, multiple imputations were conducted. A full conditional specification (Markov chain Monte Carlo method) was used to perform 50 imputations of the sample. All subsequent analyses were conducted using the imputed data and pooled estimates are reported.
Of the five dimensions of workplace support, we retained organizational support, managerial support, and co-worker support for further analysis. Physical environment, while used in the imputation process, was removed from the model due to its uniquely high proportion of missing values. Time was also dropped from modeling due to multicollinearity with other workplace support variables. Elimination of these two workplace factors (physical environment and time) precluded analysis associated with study objective 1.
Results
Table 1 summarizes the demographic characteristics of the 165 female employees. The majority of participants were 35 years of age or younger (72.7%), white (76.8%), married (88.8%), and had a college degree or greater (73.5%). Nearly one-third (30.9%) of participants were in clinical roles, 23.0% self-identified as business/administrative staff, and 18.1% were in allied health or leadership positions. The remaining participants (27.8%) had roles in the “Other” category (e.g., research staff, laboratory technicians, food/environmental services, and nonspecified roles).
Demographics of Female Health Care Employees Who Breastfed in the Past 3 Years (N = 165)
N may not add up to 165 because of missing data.
Percentages reflect percent of nonmissing data.
For example, physician, physician assistant, resident, and nurse.
For example, psychologists, social worker, exercise physiologist, music therapist, and pharmacist.
For example, financial services, accountant, patient account representative, and marketing communication.
For example, executive, director, and manager (as primary role).
For example, research staff, laboratory technician, food and environmental services, and nonspecified roles.
Approximately one-third of employees (34.0%) breastfed for <6 months, 40.1% breastfed for 6–12 months, and 25.9% breastfed for >1 year. The majority of the total sample of employees (67.3%) exclusively breastfeed for the AAP recommended duration of 6 months.
Table 2 shows summary statistics of workplace support variables. The total possible score range for workplace support was 41–160, and the observed range was 63–158. For further analyses, these variables were standardized. On a 7-point scale, average job satisfaction of the sample was 5.85 and median job satisfaction was 6.00 (data not shown in a table).
Descriptive Statistics (Workplace Breastfeeding Support)
SD, standard deviation.
Workplace support and job satisfaction
Given the skewness of the scale, a quantile regression model of job satisfaction was estimated. The effect of managerial support on job satisfaction varied by job satisfaction quantile, with higher effects at lower quantiles of job satisfaction and lower effects at higher quantiles. One standard deviation increase in managerial support increased the median job satisfaction by 0.39. For the 0.1 quantile, or the bottom 10% of the job satisfaction distribution, one standard deviation change in managerial support increased job satisfaction by 0.80. Figure 1 shows the change in this coefficient and its 95% confidence interval (CI) at various quantiles.
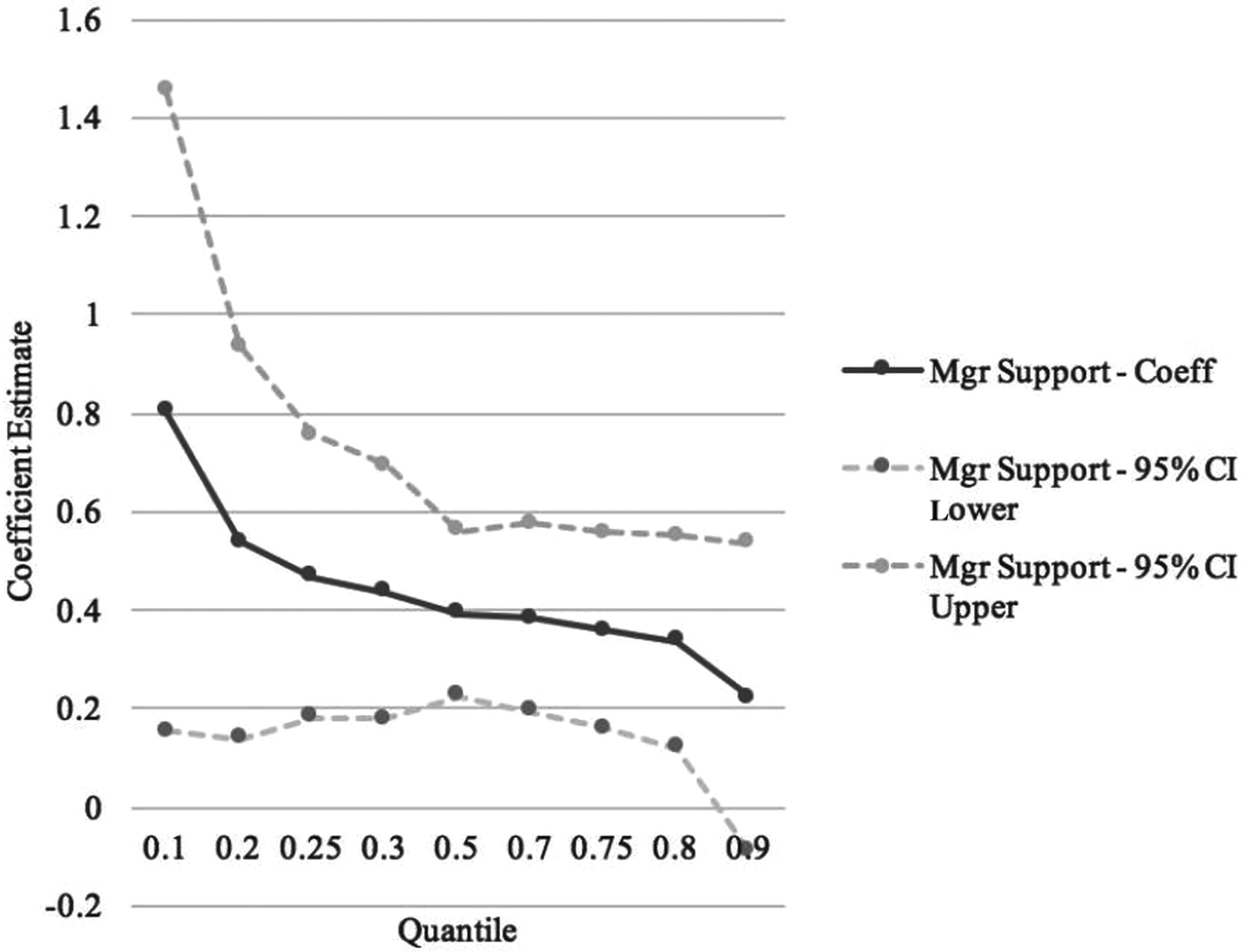
Effect of managerial support for breastfeeding on job satisfaction among female health care employees, by job satisfaction quantile.
Organizational support was also significantly associated with job satisfaction. A standard deviation increase in organizational support increased median job satisfaction by 0.27. At 0.25 quantile, this coefficient increased to 0.33, indicating higher impact of organizational support at lower job satisfaction levels. The effect, however, tapers off quickly after 0.5 quantile with no statistically significant coefficient estimates in the higher quantiles. Figure 2 shows the change in this coefficient across quantiles. Income was also associated with job satisfaction; however, only at lower quantiles. A unit increase in income level increased the 0.25 quantile of job satisfaction by 0.23 points (data not shown).
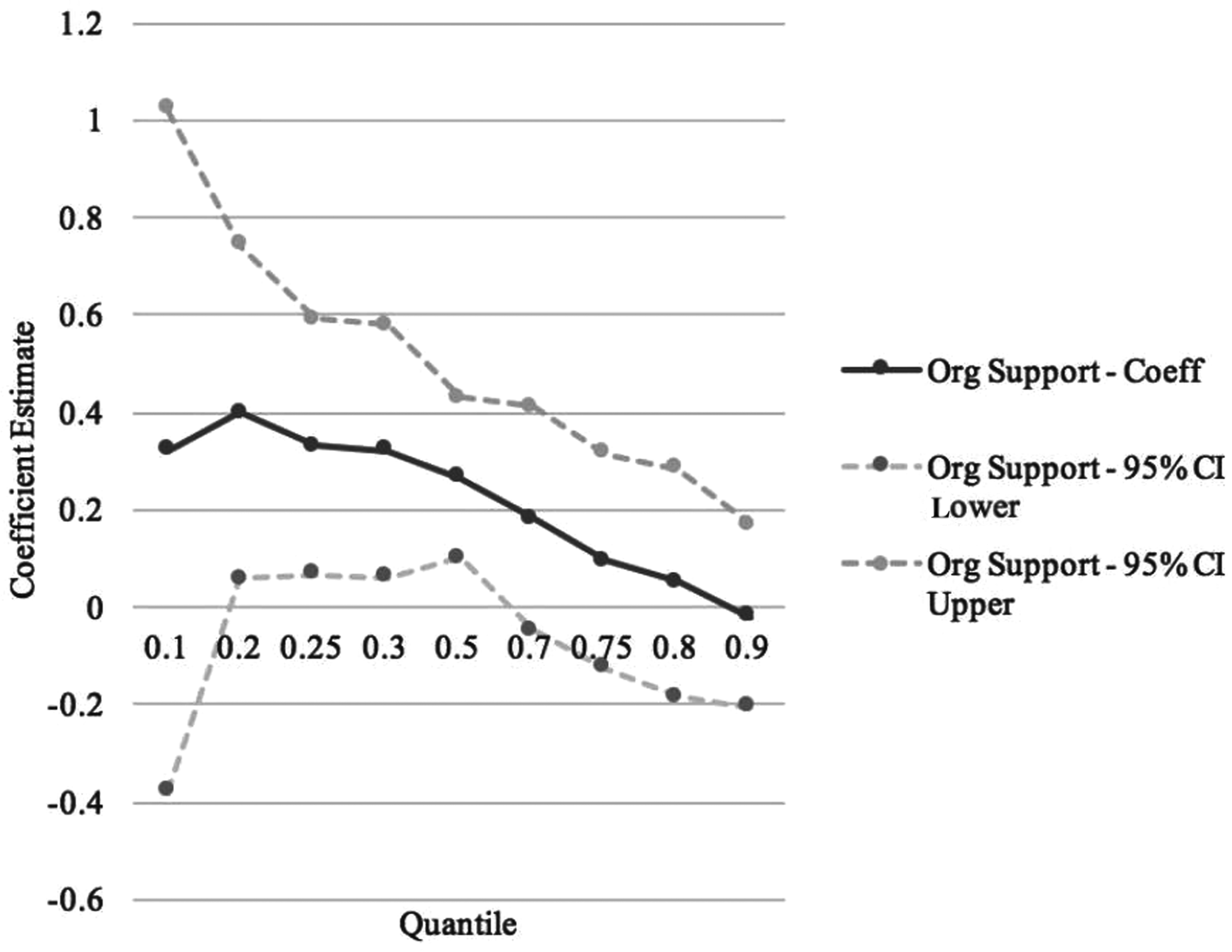
Effect of organizational support for breastfeeding on job satisfaction among female health care employees, by job satisfaction quantile.
Workplace support and breastfeeding duration
Estimates from the ordinal probit model indicated that workplace support factors had no effect on breastfeeding duration (Table 3). Younger mothers (≤35 years) were less likely to breastfeed their children for longer duration (odds ratio [OR] 0.63; CI 0.41–0.98) than older mothers (>35 years). No other demographic variables were associated with breastfeeding duration.
Association Between Workplace Breastfeeding Support and Breastfeeding Duration, Exclusivity, and Exclusive Breastfeeding Duration
Reference group: age >35.
Reference group: other race.
Reference group: graduate degree.
Less than 6 months of breastfeeding duration.
4–5 Months of exclusive breastfeeding duration.
6–12 Months of breasting duration.
6 Months of exclusive breastfeeding duration.
CI, confidence interval; OR, odds ratio.
Workplace support and exclusive breastfeeding
A binary logistic regression model was estimated (Table 3) to understand how workplace support affects the odds of exclusive breastfeeding. One standard deviation increase in organizational support increased the odds of a mother exclusively breastfeeding 1.8 times (OR 1.81; CI 1.06–3.09). Other workplace support variables had no impact on the probability of exclusive breastfeeding. An ordinal probit model was estimated to examine the impact of workplace support on exclusive breastfeeding duration (Table 3). One standard deviation increase in managerial support increased the odds of a longer exclusive breastfeeding duration (from <4 to 4–5 months and from 4–5 to 6 months) by 1.47 times (OR 1.47; CI 1.03–2.09). Mothers with less than a college degree were less likely to breastfeed exclusively for longer durations than mothers with a graduate degree (OR 0.42; CI 0.21–0.84).
Discussion
Our analyses revealed findings that were consistent with previous research as well as new findings that can inform the design of workplace lactation support programs. We identified two workplace breastfeeding support characteristics, managerial support and organizational support, which were significantly associated with job satisfaction. The study by Waite and Christakis also found a significant association between manager support for workplace lactation accommodations and job satisfaction, but did not find a significant association with organizational support. 13 They reported a significant association between co-worker support and job satisfaction, which we did not find in our study. Differences in study samples (children's hospital versus large health care system) may account for the variation in results. Research on the association between key domains of workplace support and job satisfaction in health care settings has been limited; indubitably, additional research is needed to better understand the association.
A new finding from our study was that the effect of managerial support for breastfeeding on job satisfaction is greatest for employees with low levels of job satisfaction and decreases in magnitude with increasing job satisfaction. We also found that the effect of organizational support for breastfeeding on job satisfaction was highest for employees with moderate levels of job satisfaction, suggesting that organizational support for breastfeeding has minimal to no impact on job satisfaction levels for employees who are either highly dissatisfied or highly satisfied with their jobs. The analyses conducted in this study add to the literature by identifying the spectrum of employees who may experience increases in job satisfaction as a result of increased managerial and organizational breastfeeding support.
These study findings provide practical insight into how health care systems can focus on breastfeeding support interventions to be more intentional about increasing employee job satisfaction. In seeking to improve job satisfaction among lactating employees with low-to-moderate job satisfaction levels, employers may reap the greatest return on investment by attending to direct supervisor support quality. Supervisors can demonstrate their workplace support for milk expression by discussing employee lactation needs and working with employees to meet those needs (e.g., adjusting work schedule, identifying other co-workers to provide coverage, and communicating lactation-specific needs to teammates). A recent study by Jantzer et al. 14 suggests that workplace lactation support may increase job satisfaction through a psychological pathway (mediator) by making employees feel that their work is enhancing their personal life.
In addition, job satisfaction levels may be improved for lactating employees by focusing on elements of organizational breastfeeding support (e.g., providing a lactation policy, maternity leave, and information for combining work and breastfeeding). 22 The literature on job satisfaction in health care organizations offers a number of additional suggestions, including working with employees to identify an optimal work arrangement, using a collaborative process for decision making, and soliciting continuous employee feedback.23,24 Increasing employee job satisfaction has downstream gains for the health care system. For example, higher employee job satisfaction is associated with higher patient satisfaction with health care services.25,26
The third study objective examined the relationship between workplace support and breastfeeding duration. Analyses revealed that employee perceptions of workplace breastfeeding support factors did not affect breastfeeding duration. This finding is consistent with Waite and Christakis. 13 The population in this study and the study by Waite and Christakis 13 was predominantly white, married, and educated. These demographic characteristics are associated with higher breastfeeding rates than in the general population 27 and may partially account for the nonsignificant association. Two recent systematic reviews provide additional perspective on the association between workplace support and breastfeeding duration. Specifically, the reviews reported a dose–response relationship between number of lactation services received and breastfeeding initiation, duration, and exclusivity.28,29 Future studies on associations between workplace support and breastfeeding duration might be strengthened by including a measure for number of available workplace support components.
Our fourth study aim examined the relationship between workplace support and exclusive breastfeeding. We found that organizational support was associated with a nearly twofold increase in the likelihood of a mother exclusively breastfeeding. However, our analyses revealed that only managerial support was significantly associated with exclusive breastfeeding duration. Together, these findings suggest that general organizational attributes associated with perceived workplace support for breastfeeding may influence working mothers' decision to breastfeed exclusively; however, the nature of support provided by direct supervisors is the one factor associated with how long these mothers continue to breastfeed exclusively. This finding underscores the importance of both organizational (system wide) support and managerial support for exclusive breastfeeding. Chen et al. describe workplace support for breastfeeding as having both implicit attributes (e.g., workplace culture and climate) and explicit attributes (e.g., policies and access to lactation space), which both require consideration. 30 Their research revealed that even with lactation facilities and policies in place, the underlying workplace culture may still discourage breastfeeding. Some mothers choose not to breastfeed, despite the presence of breastfeeding policies because of concerns about work performance (i.e., the belief that milk expression at work would impact likelihood of receiving productivity bonuses). Supervisors are well positioned to play a key role in aligning explicit and implicit workplace expectations for lactation. Kim et al.'s 29 systematic review of the effectiveness of workplace lactation interventions on breastfeeding outcomes identified three factors significantly associated with duration of exclusive breastfeeding: (1) receiving a breast pump for 1 year, (2) return-to-work consultations, and (3) telephone support. Employers might prioritize these three components of lactation support for lactating employees who return to work within 6 months postpartum.
Limitations
Limitations in the statistical data (missing values and multicollinearity) precluded analysis of two domains of workplace support for breastfeeding, time and physical environment. Further research is needed to clarify whether the issue of multicollinearity was unique to this sample, or if it is a measurement issue specific to the EPBS-Q. 19 While we were unable to assess perceptions of time and lactation space, open-ended responses provided by study participants suggest that availability of both time and lactation space is critical to workplace milk expression.
In addition, our sample included employees who had a baby in the past 3 years. While the study asked participants about their experiences based on breastfeeding their youngest child, it did not record the age of the youngest child. Some respondents may have been actively breastfeeding at the time of survey completion. As such, the data may underestimate breastfeeding duration and exclusive breastfeeding duration. In addition, the cross-sectional study design does not allow us to make causal inferences about the relationship between perceived workplace support and breastfeeding outcomes. Future studies with longitudinal designs would help to overcome these limitations.
Finally, study participants were considerably homogenous in demographic characteristics (mostly young, White, married, and college educated). This may limit the generalizability of the findings to workplaces with a different composition of employee characteristics. Additional research with a more heterogeneous sample is suggested.
Conclusion
Organizational and managerial support are key aspects of workplace lactation support, which may positively impact job satisfaction, rates of exclusive breastfeeding and duration of exclusive breastfeeding among female health care employees. This intersection of outcomes that are salient for the business community with those that are of interest for public health practitioners highlights opportunities for collaborations to improve outcomes. Toolkits such as the Business Case for Breastfeeding provide a step-by-step guide that businesses can use to educate managers and promote a breastfeeding-friendly culture. a Businesses can further improve organizational support for breastfeeding through lactation policies and by providing space and time flexibility for milk expression. In addition to providing educational tools and resources, public health organizations may consider ways to actively engage businesses as partners in achieving goals for exclusive breastfeeding through targeted campaigns, sponsorships, or other means, with the goal of reducing barriers to breastfeeding for mothers who return to work postpartum. Future research should examine the impact of the availability of time and adequacy of lactation space on job satisfaction and breastfeeding duration, as these domains were not adequately examined in this study. Replicating this study in other work settings would also be useful for understanding which findings are unique to health care and which findings may have broader application.
Footnotes
Acknowledgments
This study was funded by the UNCC Faculty Research Grant and the Center for Outcomes Research and Evaluation at Atrium Health. The study was made possible by the CHEBS team and health care system leadership: Katherine Buehler, Crystal Danielle Connor, Jordan McGee, Margaret Gigler, Johnnie Jones, and Brandi Newman.
Disclosure Statement
No competing financial interests exist.