
Abstract
Abstract
Background:
Over half of pregnant women in the United States do not meet the recommended gestational weight gain (GWG). In addition, the prevalence of gestational diabetes mellitus (GDM) is increasing. We examined the combined influence of GDM and GWG on breastfeeding practices on exclusive breastfeeding during the neonatal period and at 3 months postpartum.
Materials and Methods:
A cross-sectional study was performed on 173,603 women from the pregnancy risk assessment monitoring system, 2009–2015. Descriptive statistics and multivariable logistic regression modeling were performed.
Results:
The prevalence of GDM was 9.5%. Only 30.7% of women had weight gain within the Institute of Medicine (IOM) recommended guidelines. Approximately 21.7% and 10.3% of the participants exclusively breastfed their infants during the neonatal period and at 3 months postpartum, respectively. After adjusting for potential confounders, there was a significant multiplicative interaction between GWG and GDM on exclusive breastfeeding during the neonatal period and at 3 months postpartum. Among women with normal and excessive GWG, the odds of exclusively breastfeeding during the neonatal period were lower for women with GDM compared with women without GDM (odds ratio, 95% confidence interval: 0.74, 0.64–0.85 and 0.75, 0.66–0.85, respectively). Similarly, among women with normal and excessive GWG, the odds of exclusively breastfeeding at 3 months postpartum were lower for women with GDM compared to women without GDM (0.67, 0.55–0.81 and 0.71, 0.60–0.85, respectively).
Conclusion:
With the increasing prevalence of GDM and weight gain outside the IOM guidelines, it is critical to identify populations at risk and to promote exclusive breastfeeding practices.
Introduction
Gestational diabetes mellitus (GDM) affects ∼2–10% pregnancies in the United States. 1 Studies have shown an increased risk of GDM due to maternal obesity. 2 Since 1976, the prevalence of obesity in the United States has doubled among women of childbearing age. 3 Recent estimates indicate that more than one-third of women in the United States are obese, nearly 8% of reproductive age women are extremely obese, and more than half of pregnant women are overweight or obese. 3 Maternal prepregnancy obesity has been shown to be associated with excessive gestational weight gain (GWG),4–6 and with a lower rate and shorter duration of exclusive breastfeeding.7–9
Breastfeeding renders health-related benefits to the mother and her infant. For women, breastfeeding is known to reduce the risk of breast and ovarian cancer, 10 and has a protective effect against type 2 diabetes.11–14 For children, breastfeeding has a protective effect against early childhood undernutrition and overnutrition, 15 and may reduce the risk of developing obesity, 16 hypertension, 17 cardiovascular disease, 17 and diabetes later in life.14,18
Current World Health Organization recommendations include 6 months of exclusive breastfeeding and continued breastfeeding for at least 12 months. 19 Research has shown a dose–response relationship between duration of exclusive breastfeeding and weight gain later in life. 18 Increasing the duration of exclusive breastfeeding significantly reduces the risk of being overweight later in life. 18 In addition, infant feeding practices contribute to the early developmental period and have been hypothesized to have a metabolic programming effect, including the development of chronic diseases.20,21
Mothers with GDM who breastfeed are more likely to have improved blood glucose and insulin profiles, increased insulin sensitivity, and reduced risk of diabetes later in life, compared with those who do not breastfeed.22,23 Several studies have reported lower rates of exclusive breastfeeding among women with Type I diabetes,24–26 Type II diabetes,27,28 and GDM.28,29 Another study found no difference in overall breastfeeding initiation rates among women with and without GDM, 30 although the study did not assess exclusive breastfeeding.
Deleterious effects of GDM and inadequate or excessive GWG on maternal and child health outcomes are widely established.31–34 However, population-based research examining the joint effects of GDM and GWG on exclusive breastfeeding is currently lacking. Considering the rising prevalence of GDM and GWG outside the recommended guideline, research is needed to examine the combined effects of GDM and GWG on exclusive breastfeeding. The purpose of this study was to explore the combined influence of GDM and GWG on exclusive breastfeeding in the neonatal period and at 3 months postpartum.
Materials and Methods
We performed a secondary data analysis using pregnancy risk assessment monitoring system (PRAMS) 2009–2015. PRAMS is a surveillance project of the Centers for Disease Control and Prevention and state health departments. A systematic sampling methodology is used to draw representative sample of United States women with recent live births. To be included in the national PRAMS, participating states oversample subpopulations, including minority groups and high-risk deliveries such as low birth weight, and preterm, to achieve a minimum response rate of 65%. At ∼2 to 6 months postpartum, a questionnaire is administered by mail or telephone on a range of topics, including demographics, prenatal care, substance use before and during pregnancy, maternal stress, abuse, and contraception. The core items on the questionnaire are asked by all the states, with the option of each state adding questions. For the purpose of analysis, these self-reported responses are linked to birth certificate data from vital records.
PRAMS data are weighted for sample design, nonresponse, and noncoverage. The questionnaires are revised periodically to reflect changing priorities and emerging issues. The current study utilized data from the core questionnaire. A detailed information on the PRAMS methodology and questionnaire is available elsewhere. 35 To maximize generalizability, PRAMS is designed in such a way that certain high-risk populations are oversampled, such as mothers of low-birth-weight infants, those living in high-risk geographic areas, and racial/ethnic minority groups. However, the sample is restricted to only one randomly selected infant from pregnancies that resulted in twins or triplets and excludes infants from pregnancies that resulted in pluralities of four or more. A total of 247,430 respondents were interviewed during PRAMS phases 6 and 7. We excluded responses from the state of Vermont due to missing information on race/ethnicity (n = 6,725). Similarly, respondents with missing information on GDM status and GWG (n = 3,038), exclusive breastfeeding duration (n = 624), and covariates adjusted in the multivariable model (n = 63,440) were excluded from the analysis. Thus, the final analytical sample consisted of 173,603 respondents. This study was deemed exempt by the Institutional Review Board of the authors' institution because it was a secondary analysis of a publicly available dataset.
Exposure assessment
Prepregnancy body mass index (BMI) and weight gain during pregnancy were used to define GWG categories: inadequate (less than the recommended guideline), adequate (within the recommended guideline), and excessive (above the recommended guideline). This classification is based on the 2009 Institute of Medicine guidelines for recommended GWG (12.5–18 kg for underweight women [BMI <18.5]; 11.5–16 kg for normal-weight women [BMI 18.5–24.9]; 7–11.5 kg for overweight women [BMI 25–29.9]; and 5–9 kg for obese women [BMI ≥30]). 36 GDM status was determined based on how the patients responded to the question, “Have you had gestational diabetes with this pregnancy?” and was coded as “yes” and “no”.
Outcome assessment
The timing of exclusive breastfeeding duration during the neonatal period and at 3 months postpartum was determined using women's response to questions, including breastfeeding initiation, whether or not they were still breastfeeding at the time of the survey, weeks the baby was breastfed, weeks first fed liquid, the infant age in weeks when liquid other than mother's milk was fed for the first time, when solid food was introduced for the first time, and the age of the infant on the day of the survey. Exclusive breastfeeding in the neonatal period (4 weeks) and at 3 months (12 weeks) was determined for women who initiated breastfeeding. Initiation was defined based on yes/no responses to the question, “Did you ever breastfeed or pump breast milk to feed your new baby after delivery, even for a short period of time?” Exclusive breastfeeding in the neonatal (4 weeks) and 3 months (12 weeks) was determined by the questions “How old was your new baby the first time he or she drank liquids other than breast milk (such as formula, water, juice, tea, or cow's milk)?” and “How old was your new baby the first time he or she ate food (such as baby cereal, baby food, or any other food)?” If no other liquids or foods had been introduced by week 4 and 12, then the woman was considered to have breastfed exclusively in the neonatal and 3 months postpartum. The date of survey completion was considered the duration of breastfeeding for women who were still breastfeeding. Exclusive breastfeeding was coded as “yes” and “no” both for the neonatal period and 3 months postpartum.
Covariates
We examined several potential confounders, including maternal age, marital status, race/ethnicity, prepregnancy BMI, prenatal care insurance, poverty to income needs ratio, prenatal smoking, Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) enrollment, pregnancy intention, mode of delivery, Kotelchuck's Adequacy of Prenatal Care Utilization, neonatal intensive care unit admission, and PRAMS data collection phase.
Statistical analysis
Descriptive statistics were used to summarize and describe the distribution of study variables. Rao-Scott chi-square (χ2) test were performed to determine association between exclusive breastfeeding during the neonatal period and at 3 months postpartum by GDM status, GWG, and each covariate. Multivariable logistic regression analyses were used to determine the direction and magnitude of multiplicative interaction between GWG and GDM on exclusive breastfeeding. We used the purposeful selection process to retain only variables with a significant univariate test at α ≤ 0.20 in the multivariable analyses. 37 Statistical interaction of GDM with GWG was assessed using Wald tests for interaction terms at the p ≤ 0.20 in the multivariable models. The corresponding odds ratio (OR), 95% confidence interval (CI), and p-value were determined. We assessed potential multicollinearity using variance inflation factor (VIF). Using a conservative cutoff threshold of VIF greater than or equal to 4, our regression analyses were not prone to multicollinearity. To account for the complex survey, PROC SURVEY procedures were used using SAS 9.4 (SAS Institute, Inc., Cary, NC). Statistical tests were two sided, and statistical significance was set as p < 0.05. Complete-case analysis (listwise deletion) approaches were used in all analyses.
Results
Overall, 24.7%, 30.7%, and 44.6% of the participants had inadequate, adequate, and excessive GWG, respectively. Approximately 9.5% of the participants had GDM, and 21.7% and 10.3% of the participants exclusively breastfed their infants during the neonatal period and at 3 months postpartum, respectively. A majority of the study participants were 25–34 years of age (57.6%), had more than high school education (63.0%), were married (63.2%), non-Hispanic white (63.2%), and had a normal prepregnancy BMI (47.4%) (Table 1).
Characteristics of the Postpartum Women Who Participated in the Pregnancy Risk Assessment Monitoring System Survey 2009–2015 (n = 173,603)
BMI, body mass index; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children; APNCU, adequacy of prenatal care utilization; NICU, newborn intensive care unit; PRAMS, pregnancy risk assessment monitoring system.
In the bivariate analysis, there was a statistically significant association between GWG and exclusive breastfeeding during the neonatal period, at 3 months postpartum. Similarly, there was a statistically significant bivariate association between GDM and exclusive breastfeeding during the neonatal period, at 3 months postpartum, and with all the potential confounders, except for marital status, pregnancy intention, smoking and data collection phase (Table 1).
Bivariate analyses by both outcomes showed statistically significant associations among GDM, GWG, and exclusive breastfeeding during the neonatal period and at 3 months postpartum. Women with GDM were less likely to exclusively breastfeed during the neonatal period (16.8% yes versus 22.2% no) and at 3 months postpartum (6.8% yes versus 9.8% no) compared with those without GDM. Likewise, women with GWG outside the recommended guidelines were less likely to exclusively breastfeed during the neonatal period (20.9% inadequate versus 23.8% normal versus 20.7% excessive GWG) and at 3 months postpartum (9.3% inadequate versus 10.8% normal versus 8.8% excessive GWG) (Table 2).
Characteristics of the Study Sample by Exclusive Breastfeeding During the Neonatal Period and at Three Months Postpartum (n = 173,603)
In the multivariable model, there was a significant multiplicative interaction between GDM and GWG on exclusive breastfeeding during the neonatal period (p for interaction = 0.001) and at 3 months postpartum (p for interaction = 0.005). Table 3 reports the combined effect of GDM and GWG on exclusive breastfeeding during the neonatal period. Among women with normal and excessive GWG, the odds of exclusively breastfeeding during the neonatal period were lower for women with GDM compared to women without GDM (OR, 95% CI: 0.74, 0.64–0.85 and 0.75, 0.66–0.85, respectively). Table 4 presents the combined effect of GDM and GWG on exclusive breastfeeding at 3 months postpartum. Among women with normal and excessive GWG, the odds of exclusively breastfeeding at 3 months postpartum were lower for women with GDM (OR, 95% CI: 0.67, 0.55–0.81 and 0.71, 0.60–0.85, respectively). However, among women with inadequate GWG, there were no significant associations between GDM and exclusive breastfeeding during the neonatal period and at 3 months postpartum.
Association Between Gestational Diabetes Mellitus and Exclusive Breastfeeding During the Neonatal Period Stratified by Gestational Weight Gain (n = 173,603)
AOR, adjusted odds ratio; CI, confidence interval.
Association Between Gestational Diabetes Mellitus and Exclusive Breastfeeding at Month Three Postpartum Stratified by Gestational Weight Gain (n = 173,603)
Discussion
In the current study, we observed a reduction in the odds of exclusive breastfeeding during the neonatal period and at 3 months postpartum in women with GDM who had normal and excessive GWG. These findings are congruent with a recent study in Brazil that found an additive interaction between GDM and obesity on the timing of initiation of any amount of breastfeeding. 38 Although there were other factors that likely influenced this breastfeeding practice, including cesarean delivery and parity, as well as a lack of clarity regarding hospital policy and practice for maternal–infant dyads affected by GDM and obesity, studies have reported reduced prevalence and continuation of breastfeeding among women with GDM, high prepregnancy BMI, and excessive GWG.22,39 Furthermore, in a large Norwegian study, excessive BMI and excessive GWG were synergistically associated with lower rates of exclusive and overall breastfeeding at 4 and 6 months. 40
Two older studies in the United States found early termination of overall breastfeeding among women with excessive GWG41,42 and obese women 42 compared to women with normal prepregnancy BMI or adequate GWG, following animal models suggesting poor lactation associated with maternal obesity. 43 However, contrary to the above study findings, a more recent prospective longitudinal cohort study in Pennsylvania found no statistically significant differences in breastfeeding duration among overweight/obese women, and/or women with excessive GWG, and women who had a normal prepregnancy BMI and adequate GWG, although obese women with excessive GWG experienced delayed onset of lactation. 42 Considering the methodology of the cohort study, which was part of randomized clinical trial 44 that included breastfeeding promotion and support following supplemented breastfeeding education for the nurses working with the research team, it is plausible that participants with excessive BMI and/or GWG were more motivated and encouraged to engage in breastfeeding at rates similar to normal weight women, suggesting that support of these women reduces their risk of poor breastfeeding outcomes.
There are several plausible mechanisms for the observed reduced likelihood of recommended breastfeeding practices among women with excessive GWG that include (i) delayed onset of lactation due to lower prolactin response39,45; (ii) high adipose tissue mass may function as a reservoir for steroid hormones, including progesterone, thereby inhibiting lactation 39 ; (iii) mechanical difficulties such as large breasts and body that may impede positioning 39 ; (iv) psychological influences such as body image dissatisfaction, postpartum depression, and lack of confidence about sufficient milk supply 39 ; and (v) common comorbid conditions with obesity such as obstetric complications, cesarean section, metabolic diseases, and polycystic ovarian syndrome. 39 Delayed onset of lactation could negatively affect breastfeeding outcomes, especially exclusive breastfeeding. 46 Also, lower prenatal intention to exclusively breastfeed is a strong predictor of lower rates of exclusive breastfeeding among women with GDM and excessive GWG. 7
A population-based study in Canada found lower breastfeeding rates among women with GDM compared with women without GDM. 29 Another prospective postpartum cohort study found similar results where women with GDM breastfed for shorter duration compared with women without GDM. 47 However, contrary to some of the above study findings, our study found increased odds of exclusive breastfeeding among women with GDM with inadequate GWG during the neonatal period and at 3 months postpartum. We speculate that the observed findings may be due to a different mechanism of action and an interplay of various hormonal, mechanical, and psychological factors in this subpopulation. Another plausible explanation could be increasing awareness of the importance of exclusive and sustained breastfeeding in mother–infant dyads affected by GDM 48 and a stronger breastfeeding motivation in this subpopulation of women.
Our study is subject to some limitations. The cross-sectional study design precludes causal inferences. The responses were self-reported; hence, the possibility of a recall and self-reporting and social desirability biases cannot be excluded. Furthermore, despite its breadth, PRAMS dataset lacks variables known to be associated with exclusive breastfeeding. These variables include prior breastfeeding experience, degree of GDM, type of medication, blood sugar control (HbA1C), birth weight for gestational age, breastfeeding promotion certification of delivering hospital, timing of breastfeeding after delivery, and timing of skin-to-skin contact. Residual confounding is another study limitation. In addition, several states were excluded from the survey; thus, our study findings might not be generalizable to the entire United States population. Furthermore, the denominators for the estimated prevalence of exclusive breastfeeding in the current study reflect the eligible population as shown in Figure 1. As such, these estimates are not comparable with national estimates of breastfeeding indicators. Nearly 30% of women were excluded from the current study due to missing data, which can also potentially threaten external validity of the current study. Women with missing data were more likely to be younger, had less than high school education, were primiparous, and belong to racial/ethnic minorities (Supplementary Table S1). They also were more likely to be poor, uninsured or enrolled in Medicaid, and more likely to participate in WIC. Despite the limitations, our study has numerous strengths. The data were collected from a very large sample of women in the United States. The data collection process was uniform across all states, and the study's large sample size reduces error due to chance. The extensive details on infant feeding practices in the PRAMS data enabled us to determine breastfeeding practices at different intervals. Also, availability of comprehensive data allowed adjustment of several potential confounders. Finally, random selection of PRAMS participants might have played a role in reducing the possibility of selection bias.
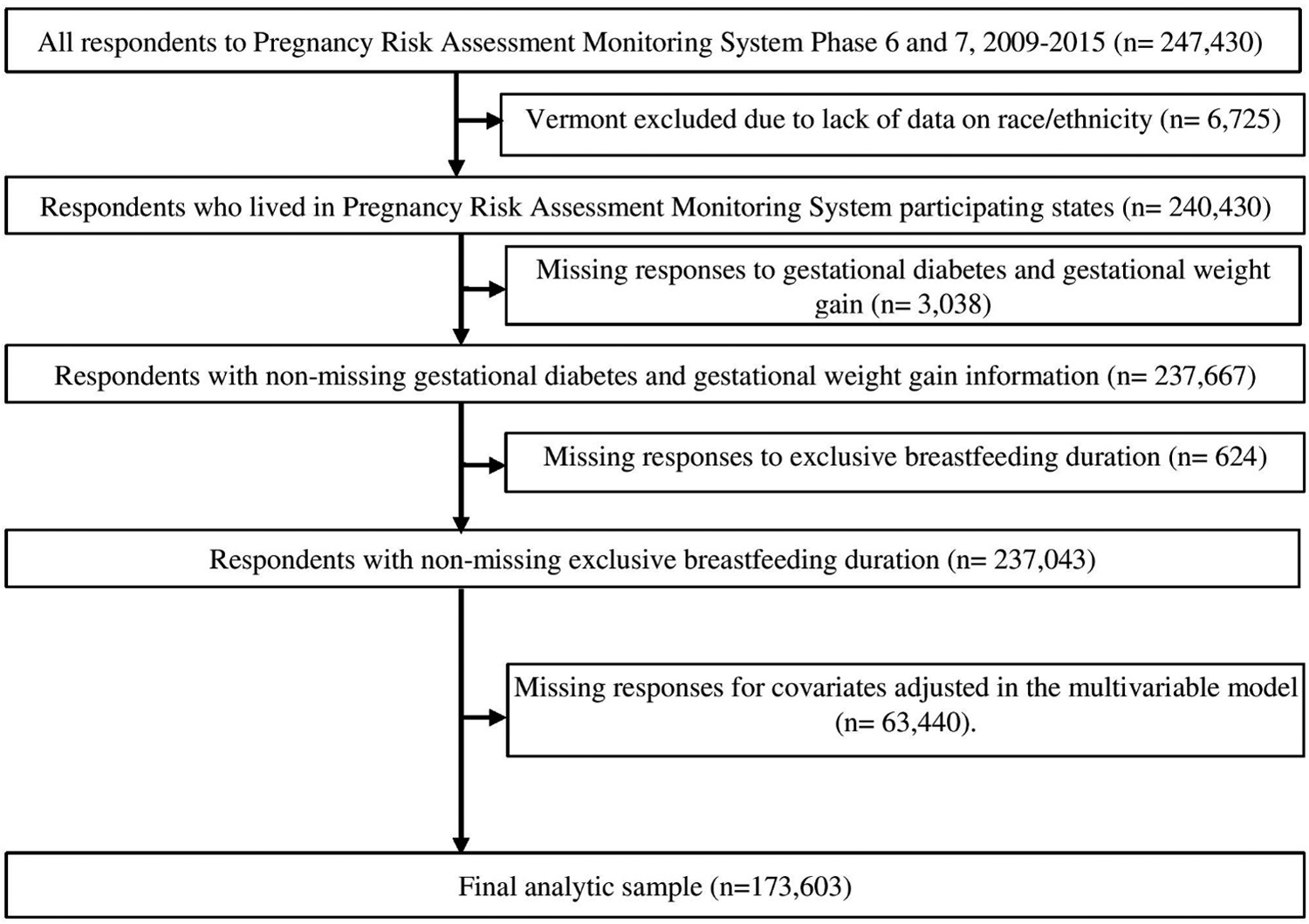
Study sample selection using PRAM Phase 6 and 7, 2009—1,015 dataset.
Our study may have public health implications. As the prevalence rates of excessive GWG and GDM have dramatically risen among women in the United States, along with one of their primary risk factors of maternal obesity, the focus on antenatal health practices is important in reducing poor postpartum health outcomes. The study findings of lower rates of exclusive breastfeeding during the neonatal period and at 3 months postpartum among this subpopulation of women warrant need of targeted interventions to promote and support exclusive breastfeeding. Previous research findings 44 suggest that support by health care providers can facilitate improved breastfeeding outcomes among this at-risk population. 44 More research should be conducted to determine effective approaches to promoting exclusive breastfeeding among the specific population of women with GDM and excessive GWG.
Conclusion
Exclusive breastfeeding is recommended for nearly all maternal–infant dyads, especially those with increased risk for metabolic disorders. Women with GDM and/or excessive GWG have lower rates of exclusive breastfeeding and face challenges that negatively influence the practice, although the exact mechanism of action is yet to be determined. Longer duration of exclusive breastfeeding will help maternal–infant dyads in reducing risks associated with GDM and excessive GWG. Approaches to effectively promote exclusive breastfeeding in this at-risk population are needed to improve breastfeeding outcomes.
Footnotes
Acknowledgments
The authors acknowledge the PRAMS Working Group (Alabama: Izza Afgan, MPH; Alaska: Kathy Perham Hester, MS, MPH; Arkansas: Mary McGehee, PhD; Colorado: Rickey Tolliver, MPHC; Connecticut: Jennifer Morin, MPH; Delaware: George Yocher, MS; Florida: Elizabeth C. Stewart, MSPH; Georgia: Florence A. Kanu, MPH; Hawaii: Matt Shim, PhD, MPH; Illinois: Patricia Kloppenburg, MT (ASCP), MPH; Iowa: Jessica Egan; Kentucky: Tracey D. Jewell, MPH; Louisiana: Rosaria Trichilo, MPH; Maine: Tom Patenaude, MPH; Maryland: Laurie Kettinger, MS; Massachusetts: Emily Lu, MPH; Michigan: Peterson Haak; Minnesota: Mira Grice Sheff, PhD, MS; Mississippi: Brenda Hughes, MPPA; Missouri: David McBride, PhD; Montana: Emily Healy, MS; Nebraska: Jessica Seberger; New Hampshire: David J. Laflamme, PhD, MPH; New Jersey: Sharon Smith Cooley, MPH; New Mexico: Oralia Flores; New York State: Anne Radigan; New York City: Pricila Mullachery, MPH; North Carolina: Kathleen Jones Vessey, MS; North Dakota; Grace Njau, MPH; Ohio: Connie Geidenberger, PhD; Oklahoma: Ayesha Lampkins, MPH, CHES; Oregon: Claudia W. Bingham, MPH; Pennsylvania: Tony Norwood; Rhode Island: Karine Tolentino Monteiro, MPH; South Carolina: Kristin Simpson, MSW, MPA; Texas: Tanya Guthrie, PhD; Tennessee: Ramona Lainhart, PhD; Utah: Nicole Stone; Vermont: Peggy Brozicevic; Virginia: Sara Varner, MPH; Washington: Linda Lohdefinck; West Virginia: Melissa Baker, MA; Wisconsin: Christopher Huard; and Wyoming: Lorie Chesnut, PhD); and Centers for Disease Control and Prevention PRAMS Team, Applied Sciences Branch, Division of Reproductive Health.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.