
Abstract
Abstract
Objectives:
Long-term storage of human milk (HM) requires freezing at low temperatures, the consequences of which upon macronutrients are unclear. The conflicting results of the few studies on freezing-induced changes on HM macronutrients led to different storage recommendations. We examined differences in macronutrients content of HM after long-term storage at −20°C compared with −80°C.
Materials and Methods:
Mature HM samples from 25 mothers of term and preterm infants were collected. Each sample was divided into six aliquots for storage at −20°C and −80°C for 4, 12, and 24 weeks. After thawing and homogenization, energy and macronutrients content were measured using an HM infrared spectroscopy analyzer.
Results:
A total of 150 HM samples were available for analysis. Thirteen samples were removed due to calibration errors. The final analysis was performed on 137 samples with validated results. Fat and energy content were consistently higher in the −80°C samples compared with the paired −20°C samples at each time point (p < 0.05). Comparison of the differences in macronutrients content over time (4 versus 24 weeks) revealed a significant loss of fat (0.3 g/100 mL [7.9%], p = 0.001) and energy (2.3 kcal/100 mL [3.3%], p = 0.03) in the −20°C group. Fat and protein were also significantly decreased over time in the −80°C group (by 0.14 g/100 mL [3%], p = 0.009, and 0.06 g/100 mL [6.4%], p = 0.02, respectively).
Conclusions:
Long-term storage of HM at −80°C is associated with better fat and energy preservation compared with storage at −20°C. These results may help construct evidence-based recommendations and guidelines for optimal HM storage.
Introduction
Human milk (HM) is considered the best nutrition for term and preterm infants. 1 HM enhances gastrointestinal and cognitive functions and provides a host defense against infections. It is associated with shorter duration of preterm infant hospitalization and protection against necrotizing enterocolitis (NEC).2–4 Although breastfeeding is the optimal way to preserve and transfer breast milk nutrients and bioactive components, 5 factors related to both infants (such as prematurity) and mothers (such as maternal medical condition) may impair its implementation. In such cases, HM feeding relies on milk expression and storage of the mother's milk and/or on donor HM banks. 6 The accelerated development of donor HM banks around the world has mandated handling and storage guidelines to optimize the integrity of expressed and long-term stored milk. While freezing at −70°C or −80°C is believed to be the gold standard for long-term milk conservation,7,8 it requires expensive freezers that are not available in most HM banks. 9 The optimal preservation temperature (−80°C or −20°C) of HM has been largely discussed in the literature over the past few decades. Some studies have shown that −20°C is a satisfactory long-term storage freezing temperature for HM components,10–12 whereas others have suggested that it is inadequate.13–15 The data that are available regarding the effect of storage at −80°C derive from studies mostly on antioxidant capacity,8,16 bactericidal activity,7,17 and colostrum. 18
We had shown that freezing preterm HM at −80°C resulted in a significant loss of macronutrients when compared with fresh preterm HM. 19 To the best of our knowledge, there are no studies that examined differences in macronutrients content between HM samples stored at −20°C compared with HM samples stored at −80°C. Our present study was designed to address this question.
Materials and Methods
Patients
Mothers of term and preterm infants were recruited at the delivery room, maternity ward, nursery, or neonatal intensive care unit at the Lis Maternity Hospital, Tel Aviv Medical Center. The study was approved by the local institutional review board, and written informed consent was obtained from all participants. General demographics and medical data were collected using a standard questionnaire.
Laboratory methods
Samples of expressed HM were collected from mid-expression using a commercial breast milk pump (Medela, Baar, Switzerland) at home or in hospital settings. Immediately following extraction, each sample was divided into 6 aliquots of 3 mL each: 3 aliquots for storage at −20°C (storage duration of 4, 12, and 24 weeks) and 3 aliquots for storage at −80°C (storage duration of 4, 12, and 24 weeks) for a total of 150 aliquots. The fresh expressed HM aliquots were stored in hospital/home refrigerators at 4°C for a maximum period of 24 hours before being transferred for long-term storage at −20°C and −80°C.
At precisely 4, 12, and 24 weeks of freezing durations, each aliquot was thawed and analyzed for its macronutrients content. Thawing was performed by heating the aliquot at 40°C in a thermostatic bath in accordance with the HM analyzer (MIRIS, Uppsala, Sweden) thawing protocol. Homogenization was obtained by ultrasonication using a sonicator (MIRIS) as recommended by the manufacturer. As soon as the aliquots were thawed and homogenized, the macronutrients and energy content were measured using an HM analyzer (MIRIS), an instrument based on mid-infrared transmission spectroscopy,20–22 which provides results with repeatability values of <0.05%. 23
Statistical analyses
Paired samples (−20°C and −80°C of the same time point) were analyzed in the same run to minimize any possible batch effects. Descriptive and analytical statistical analyses were performed using standard computerized statistical software (IBM SPSS version 24 for Windows, Armonk, NY). The one-sample Kolmogorov–Smirnov test for normal distribution was used to test for normal distribution of the measured variables. The paired t-test was used to compare macronutrients content at different storage freezing conditions and at different time points for normally distributed data. The Wilcoxon matched signed-rank two-samples test was used for statistical analyses of nonnormal distributed data. The paired comparison design ensures the elimination of any possible confounders, such as prematurity, maternal age, or body mass index, 24 and enhances the power of the study. Differences were considered statistically significant at p < 0.05.
Results
A total of 150 samples of mature HM (20 mL each) from 25 mothers of term and preterm infants were collected and analyzed. We excluded 13 samples due to faulty calibration of the HM analyzer, yielding a total of 137 samples with validated results for inclusion in the final analysis.
All mothers were reportedly healthy, they had a mean age of 31.9 ± 4.9 years (range 18–39 years), and none were being treated by any medication. Among the infants, there was one pair of twins, and a total of 13 (50%) females and 13 (50%) males. Eleven of the 26 babies (42%) were preterm, and the mean gestational age for the entire group was 35 ± 5.5 weeks (range 23–42 weeks). The mean birth weight was 2,524 ± 1,027 g (range 532–4,150 g). Descriptive statistics of protein, fat, carbohydrates, and energy measured by the MIRIS HM analyzer are listed in Table 1.
Descriptive Statistics of Macronutrients in Human Milk, n = 137 Samples
SD, standard deviation.
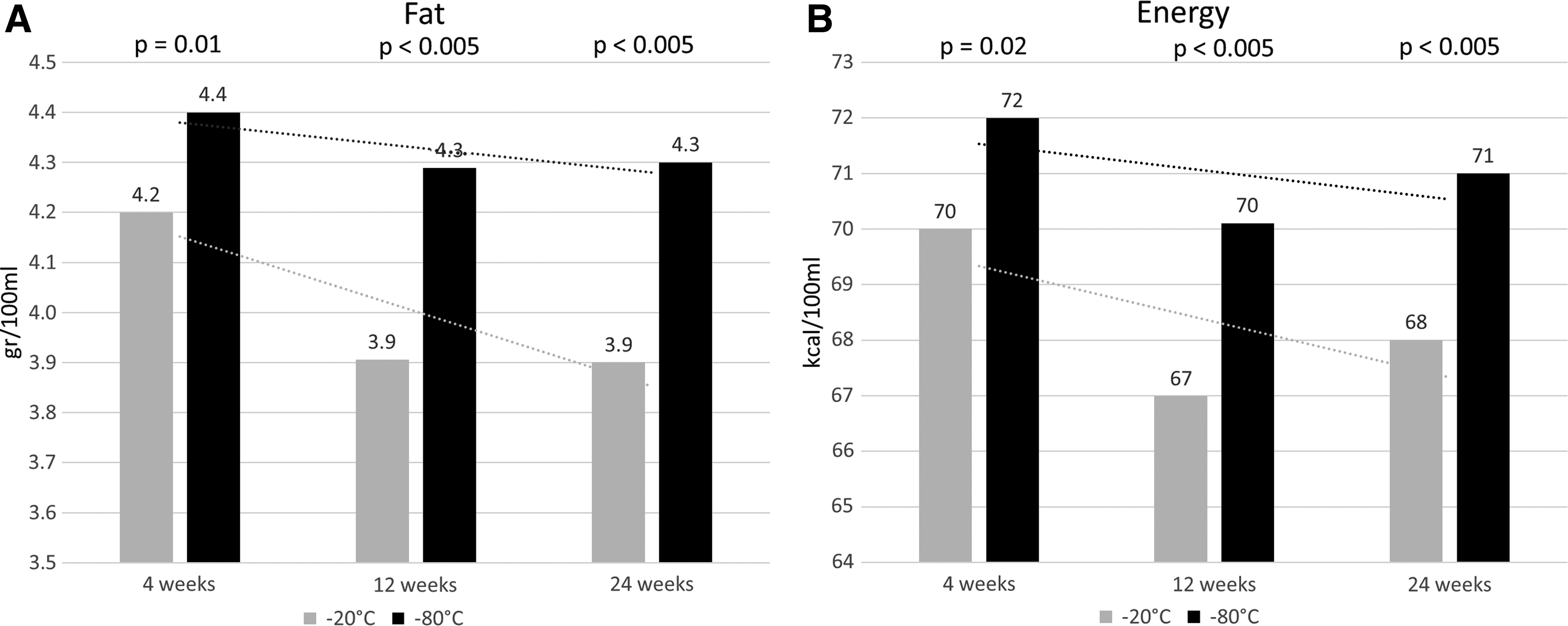
Fat and energy content were consistently significantly higher in the −80°C samples compared with the paired −20°C samples as a complete paired group (p < 0.0005, Table 2) and at each of the time points (Fig. 1). The same group comparisons for proteins (paired-t test) and carbohydrates (Wilcoxon signed-rank test) did not reveal any significant differences (Table 2). The delta of macronutrients loss between the two freezing temperatures and of the loss for each paired sample (paired for both the mother and the duration of freezing) were calculated, and the means of all deltas per macronutrients are depicted in Table 3. The mean fat loss between samples maintained at −80°C and those maintained at −20°C was 0.4 g/100 mL (equal to a 9.5% decrease), and the mean energy loss was 4 kcal/100 mL (equal to a 4.3% decrease). The loss of proteins and carbohydrates was negligible and insignificant (Table 3).
Comparison of Fat, Protein, and Carbohydrate Content Between the −20°C and −80°C Groups
Data are presented as mean ± SD.
Paired t-test.
Wilcoxon matched signed-rank test.
Paired Losses (Absolute and Percentage) Between −20°C and −80°C
SEM, standard error of the mean.
Comparisons of the macronutrients concentrations over time (4 versus 24 weeks) revealed a significant loss of fat (0.3 g/100 mL [7.9%], p = 0.001) and energy (2.3 kcal/100 mL [3.3%], p = 0.03) in the −20°C group. Fat was also significantly decreased over time in the −80°C group (0.14 g/100 mL [3%], p = 0.009) as were proteins (0.06 g/100 mL [6.4%], p = 0.02) (Fig. 1).
Discussion
Storage of expressed HM at a temperature of −80°C might be significantly beneficial in terms of fat and energy preservation compared with storage at −20°C. We demonstrated the advantage of freezing at −80°C at several time points. The absolute mean difference between the two freezing temperatures was 0.4 g/100 mL for fat, 4 kcal/100 mL for energy, and negligible for proteins and carbohydrates. Hence, most of the calories drop was caused by the reduction of fat content. The fact that different storage temperatures result in a significant change in fat content but did not influence significantly the composition of carbohydrates and protein is consistent with several other studies that showed that fat is more prone to biodegradation when HM is subjected to processes, such as pasteurization, freezing, or thawing.23,25–27 Given that the average nutrition requirement for a term baby is 140–200 mL/kg/day of HM, 28 the study findings should be interpreted according to the baby's weight and daily intake. For example, a preterm baby who weighs 1 kg and consumes 160 mL/kg/day (160 mL/day of HM), will benefit from HM stored at −80°C instead of −20°C by consuming an additional 0.6 ± 0.1 g of fat per day (12% of the daily requirement) and 6.4 ± 1.9 kcal/day (5% of the daily requirement).
The current guidelines for freezer storage temperatures of HM in donor HM banks are between −20°C and −25°C. 9 A recent study has demonstrated that freezer storage of HM for 9 months at −20°C compared with fresh HM is associated with the preservation of key macronutrients and immunoactive components. 10 Friend et al. showed a minimum loss of the biological activity of HM when stored at −25°C for 3 months. 11 Evans et al. demonstrated that freezing at −20°C for 3 months does not affect IgA, IgG, C3, or lysozyme concentrations. 12 Other nutritional factors, such as amino acids, vitamin E (tocopherol), retinol, and lactoferrin, were also not influenced by freezing at −20°C. 11 In contrast, other studies suggested that long-term freezing at −20°C versus fresh HM might result in loss of important HM components, such as fat, lactose, caloric content, 13 and lactoferrin.14,15
There are few data on the effect of HM storage at −80°C on HM content. We had earlier shown that storage of preterm HM at −80°C resulted in a significant loss of fat, carbohydrates, and energy content compared with fresh HM. 19 The present study was designed to determine the optimal long-term storage freezing temperature and the relevance for HM banks to invest in −80°C freezers.
Additional HM components should be taken into consideration to arrive at the optimal temperature for long-term storage of HM. One study showed that storage of preterm colostrum at −80°C for 3 months preserves its antioxidant capacity when compared with fresh HM. 16 Another study concluded that it is advisable to store HM at a temperature of −80°C for a maximum duration of 30 days to retain the antioxidant properties of mature HM. 8 The content of bioactive factors in colostrum was maintained during freezing storage for 6 months at either −20°C or −80°C compared with 4°C. 18 In terms of “loss over time,” we now demonstrated that the decrease in fat and energy occurred mostly at the beginning of the storage period, whereas content remained stable over time. This finding may suggest favoring the use of the most recently frozen milk.
Our results are limited to the strict time frames of the samples analysis. However, a similar observation about storage temperatures was made by Garcia-Lara et al. 23 In addition, the finding of a significant decrease in fat and energy over time partially supports the results of other studies.13,23 Although they reached a level of significance, changes over time were relatively minor: taking “energy” as an indicator of the total macronutrients losses, only 3% and 1.4% of the energy content were lost in the −20°C and −80°C groups, respectively.
The last decade has seen an increase in HM banks around the world, 29 thus mandating recommendations for the handling and preservation of optimal long-term frozen milk. Handling procedures of HM differ between the HM banks in terms of cooling temperature, cooling duration, and cooling method. 30 Since HM confers major protective effects to premature infants, its availability is an important quality of care issue. 6 From a nutritional point of view, the effect of freezing temperature on HM macronutrients content is of paramount significance for its potential to help establish a fortification regimen for this target group.
Our findings should be interpreted in the context of several limitations; first, referring to a single aliquot as a representative of macronutrients content of a whole milk. Problems such as creaming, adherence of fat to container walls, and loss of substance due to residual enzymatic activity might have their influence in different HM volumes. 31 Therefore, it is evident that 3 mL of HM does not accurately represent freezing of HM in real life. In addition, lack of data on fresh HM macronutrients content of the same subjects, and limited freezing durations tested (we could not take a larger milk volume for ethical reasons), should also be considered.
Conclusions
In conclusion, we found that long-term storage of HM at −80°C allows better fat and energy preservation compared with storage at −20°C. The study results may help construct evidence-based recommendations and guidelines for HM banks and provide better understanding of the HM macronutrients changes at different freezing conditions.
Footnotes
Acknowledgments
The authors are grateful to all the mothers participating in the present study. The study would have not been possible without their kind milk donation. There was no honorarium, grant, or other form of payment given to anyone to produce this article.
Disclosure Statement
We state that there is no potential real or perceived conflict of interest.