
Abstract
Abstract
Background:
Studies demonstrate a protective effect of antibodies (Abs) in breast milk (BM) against mother-to-child transmission (MTCT) of human immunodeficiency virus (HIV). Contribution of the BM cellular component has been overlooked. The only clinical HIV vaccine trial to demonstrate efficacy, RV144, correlated protection with Abs mediating functions through the constant immunoglobulin region—the crystallizable fragment (Fc). These data support induction of vaccine Abs triggering antiviral activities by leukocytes through Fc receptors (FcRs).
Objective:
To measure Ab-dependent cellular phagocytosis (ADCP), an essential Fc-mediated response, by BM phagocytes.
Materials and Methods:
Cells were isolated from five human BM samples obtained at 7–183 days postpartum and analyzed for ADCP. Fluorescent beads coated with HIV envelope (Env) epitopes were used as targets. Sixty-seven to 100 mL of milk was utilized.
Results:
Total cell concentrations per milliliter were 16,083–222,857, with 1.6–12.3% being CD45+ leukocytes. ADCP activity was measurable using the HIV-specific Ab 830A. Use of the actin inhibitor cytochalasin D and FcR blocker indicated that ADCP was actin dependent and required FcR engagement. ADCP scores were variable, but largely consistent, across the samples studied, exhibiting <4-fold difference from lowest to highest activity for CD45+ cells. Of the CD45+ ADCP, significantly more activity was granulocyte derived (72–95%), while the remaining activity was monocyte driven.
Conclusions:
The data indicate that BM phagocytes can manifest antiviral activities in the presence of specific Abs and therefore may contribute to reduction of MTCT of HIV.
Introduction
Mother-to-child transmission (MTCT) of human immunodeficiency virus (HIV) remains a crisis in resource-limited countries. Greater than 200,000 MTCTs occur annually, with as many as half of infections due to exposure through breast milk (BM).1,2 Even in the absence of antiretroviral drugs, only ∼10–15% of infants breastfed by HIV-infected mothers become infected, suggesting a strong protective effect of BM.1–5 Adherence to maternal highly active antiretroviral therapy (HAART) reduces MTCT to ∼1–5%, although there are concerns of toxicity and drug resistance, and the availability and adherence to HAART are not guaranteed.6–12
As diarrheal and respiratory diseases are responsible for substantial rates of mortality among infants in resource-limited countries, and these illnesses are significantly reduced by exclusive breastfeeding, the benefits to HIV-infected mothers of breastfeeding far outweigh the risks.13–15 Unless access to clean water and appropriate infant formula is reliable, the WHO does not recommend cessation of breastfeeding for HIV-infected mothers. 16 It is evident that although BM is a vehicle for HIV transmission, its virus-blocking properties are significant. Numerous factors likely work in tandem to prevent transmission. Importantly, HIV-specific antibodies (Abs) in BM have been correlated with reduced MTCT and/or reduced infant death from HIV infection.17,18 Human BM contains all immunoglobulin isotypes and subclasses, with IgA being dominant. 19 Notably, either BM IgA or IgG has been associated with reduced risk of MTCT in various studies.18,20 What remains largely unclear is the contribution of the cellular fraction of BM to its antiviral qualities.
BM comprises maternal cells that are >90% viable. 21 Cell composition is impacted strongly by the stage of lactation, health status of mother and infant, and individual variation, which remains poorly understood.21–24 Given that BM contains ∼10 2 –10 5 leukocytes per milliliter, it can be estimated that breastfed infants ingest ∼10 5 –10 8 maternal leukocytes daily. 25 Varied cell classification methods have found macrophages and neutrophils to dominate in colostrum (40–50% of total leukocytes, respectively), followed by lymphocytes (5–10%), although very few studies of BM composition beyond early lactation exist. 21 Colostrum exhibits a significantly higher cell count than mature milk.21–24 Yet, considering the increasing volume of milk ingested by young infants over the initial weeks, this difference may not be significant in a practical sense. As milk transitions to its mature composition, neutrophils appear to increase, while certain monocyte subsets decrease, although this has not been studied extensively. 26
Various in vivo studies have demonstrated that maternal leukocytes provide critical immunity to the infant and are functional well beyond these sites of initial ingestion.25,27–32 All maternally derived cells ingested by the infant have the potential to perform immune functions alongside or to compensate for the infant's own leukocytes. 33 This is likely in conjunction with other BM components, such as maternal Abs.
Many Abs that are unable to prevent viral entry per se are capable of binding to the viral surface or to viral proteins on the surface of infected cells to facilitate a variety of antiviral activities that ultimately contribute to viral clearance. These latter functions are mediated by the constant region of the immunoglobulin molecule—the crystallizable fragment (Fc)—through interaction with Fc receptors (FcRs) found on virtually all innate immune cells. 34 Follow-up analyses of RV144—the only clinical HIV vaccine trial to date to show statistical efficacy—found that reduced infection rates correlated with the level of non-neutralizing Abs specific for the V2 region of the gp120 Env (envelope) and that Fc-mediated activities, including Ab-dependent cellular phagocytosis (ADCP), correlated with the level of total serum V2 Abs.35–37 As a result, the field now recognizes the importance, in humans, of Abs that mediate antiviral functions through Fc/FcR interactions. ADCP has been demonstrated as necessary for clearance of viral infections and has been understudied in the case of prevention of MTCT of HIV.38–42 Given the paucity of knowledge about the potential contribution of ADCP activity by BM phagocytes to prevention of MTCT of HIV, we undertook the study described below of ADCP mediated by cells from BM obtained at 7–183 days postpartum.
Materials and Methods
Antibodies
The anti-HIV human mAb 830A was used for all experiments. 43 It was derived from an HIV-infected individual and is weakly neutralizing, specific for a conformational epitope in the V2 region of Env, representative of V2i-specific Abs commonly elicited by natural infection, and been shown previously to function well in ADCP assays.44,45 Anti-anthrax human mAb 3865 was used as a nonspecific negative control. These mAbs were originally isolated from human peripheral blood mononuclear cells and later reexpressed as IgG1, as previously described.46,47 Monoclonal Abs were only used after they passed all QC assays. 48
Human BM
Samples were obtained from healthy lactating women who had signed informed consents. Milk was expressed using double electronic or manual pumps. Each participant was recruited and interviewed in accord with Institutional Review Board (IRB) approval with the guidance and authorization of Mount Sinai's Program for the Protection of Human Subjects using an IRB-approved protocol for obtaining BM samples. Participants were recruited using community social media postings and flyers. Study participants met with recruiters compliant with patients' privacy and with HIPAA. The recruiter discussed the protocol with the patient and obtained written informed consent. All milk samples were picked up by courier from the woman's home, kept at room temperature, and processed in the laboratory within 4 hours. Samples were not stored for later use. BM samples were centrifuged at 600 g for 15 minutes, skim milk and fat layers were removed, and the cell pellet was washed 3 × with Hank's balanced salt solution (HBSS) by centrifugation at 350 g for 10 minutes. Care was taken to gently resuspend pellets to avoid cell activation and apoptosis. All samples were processed in precisely the same manner. Cells were counted using a Countess II FL Automated Cell Counter.
Measurement of ADCP
The ADCP assay was adapted from that described by Ackerman et al. 49 A recombinant fusion protein, V1V2-2F5K, was used as the target antigen. It was designed to mimic the trimeric V1V2 conformation in the stabilized BG505 SOSIP.664 crystal structure that is thought to be representative of the ground-state conformation of native HIV Env. 50 This scaffolded V1V2-Env protein has been found to elicit V2-specific Abs in rabbits and nonhuman primates (NHP) and is part of a larger study aimed to design V2-based immunogens following the RV144 finding that protection correlated with elicitation of V2-specific Abs in vaccines, although it was not one of the immunogens included in the RV144 trial43,51 (NHP manuscript submitted). V1V2-2F5K was produced in-house, as described by Jiang et al., 50 and subsequently biotinylated using the EZ-Link™ NHS-LC-LC-Biotin kit (Thermo Fisher) according to the manufacturer's protocol.50,52 This biotinylated protein was conjugated to 1-μm FluoSpheres® NeutrAvidin®-labeled microspheres (Thermo Fisher) at 5 μg protein per 12 μL of stock beads for 2 hours at 37°C according to manufacturers' instructions. Ten microliters of bead solution was aliquoted per well in 96-well round-bottom plates. Five-fold dilutions of mAbs in HBSS, starting at 50 μg/mL, were added and incubated for 2 hours at 37°C. Two hundred microliters of HBSS was added to wells, plates centrifuged at 2,000 g for 10 minutes, and supernatant carefully removed to avoid disturbing the bead pellet.
Fifty thousand freshly isolated BM cells were added to each well and incubated for 2 hours at 37°C. For certain control experiments, 10 μg/mL of the actin inhibitor cytochalasin D (CytoD; Sigma), 50 μg/mL of FcR-blocking agent FcBlock (Becton Dickenson), or a combination of both was preincubated with cells before their addition to the plates. After incubation, plates were centrifuged as above, washed twice, stained with viability dye (Becton Dickenson) in phosphate-buffered saline (PBS), followed by anti-CD45-PE (Becton Dickenson) in 1% bovine serum albumin-PBS, fixed in 0.5% formaldehyde, and analyzed by flow cytometry on an LSR Fortessa. Initial gating was performed to eliminate doublets, debris, and dead cells. A side scatter (SSC) versus CD45 plot was used to differentiate the major leukocyte classes (granulocytes, monocytes, and lymphocytes) as extensively described.26,53 Percent of CD45+ cells and percent of each CD45+ subset were averaged from four wells and the data reported (Table 1) as mean ± standard error. ADCP activity (bead-positive cells) was measured in the FITC channel. ADCP scores were calculated as follows: [(MFI of bead-positive cells) × (% of total CD45+ cells in the positive population)]. Scores at each mAb concentration were plotted using GraphPad Prism, and area under the curve (AUC) values were calculated. If the negative control mAb elicited ≥mean AUC +3SD determined in pilot experiments with three donors, data were excluded.
Sample Characteristics
Samples were obtained from five different women.
Results
Sample characteristics
As described in Table 1, BM samples were obtained from five women at 7–183 days postpartum. Between 67 and 100 mL of milk was utilized for cell purification. Total cell concentration per milliliter of milk ranged from 16,083 to 222,857. Leukocytes were identified as described in the Materials and Methods section by SSC versus CD45 staining. This analysis found the CD45+ proportion of BM cells to range from 1.6% to 12.3%. Within the CD45+ monocyte population, the dominant population of myeloid precursors/immature monocytes was characterized by multicolor flow cytometry classification of BM cells according to Trend et al. who previously found immature monocytes to outnumber mature monocytes by as much as 10-fold in mature milk. 26 As such, monocytes were defined as SSClow-intermediate/CD45low, although a very minor fraction of these cells exhibited higher CD45 staining levels distinct from the lymphocyte population (SSClow/CD45low) and more typically associated with mature monocytes (Fig. 1).26,53 Monocytes were found to comprise 9.1–65.9% of CD45+ cells. Granulocytes were defined relative to the monocytes as SSChigh/CD45intermediate and found to comprise 17.9–47.8% of CD45+ cells.26,53 Although these sample characteristics varied immensely (as previously reported21,26) and did not correlate with the number of days postpartum at which the samples were obtained, the earliest sample analyzed, acquired 7 days after birth—previously defined as late colostral/early transitional milk—was the most cell dense and most replete with leukocytes. 26

Definition of leukocyte subsets in BM defined by SSC and CD45 staining. Samples were centrifuged and the cell pellet was washed with HBSS. Cells were counted and then stained with anti-CD45-PE (Becton Dickenson) in 1% BSA-PBS, fixed in 0.5% formaldehyde, and analyzed on an LSR Fortessa. Initial gating was performed to eliminate doublets, debris, and dead cells. CD45+ cells were classified for the present study as granulocytes (G), monocytes (M), or lymphocytes (L) based on well-established and expected SSC parameters. Note here that the monocyte population consisted primarily of CD45low immature cells. Data shown are from sample 3 and are representative of the five samples analyzed herein. BM, breast milk; BSA, bovine serum albumin; HBSS, Hank's balanced salt solution; PBS, phosphate-buffered saline; SSC, side scatter.
ADCP activity by BM leukocytes requires actin dynamics and FcR engagement
Using the ADCP protocol modified from the Ackerman et al. assay, preliminary testing found that ADCP activity of freshly isolated leukocytes from BM could be measured (Fig. 2). HIV-specific human mAb 830A-induced ADCP activity in the total population of CD45+ cells was ∼25- to 35-fold above nonspecific background levels defined by using the control anti-anthrax mAb at comparable concentrations. Granulocytes exhibited robust ADCP activity that was 12- to 29-fold higher than background. Monocyte ADCP was measurable, but notably less potent, with mAb 830A-induced scores ∼2- to 3-fold above background (Fig. 2). Lymphocytes did not exhibit any measurable ADCP activity (data not shown). Cells from the sample shown were also used for control experiments to assess FcR dependency and true internalization of the target beads, which relies on actin dynamics. Cells were preincubated with actin inhibitor CytoD and/or FcR-blocking Abs (FcBlock) before their incubation with the Ab-bound/antigen-coupled beads. In these experiments, ADCP activity dropped to that of the control mAb level or below, indicating that bead-positive cells observed for the 830A-elicited ADCP represented FcR engagement and bead internalization (Fig. 2).
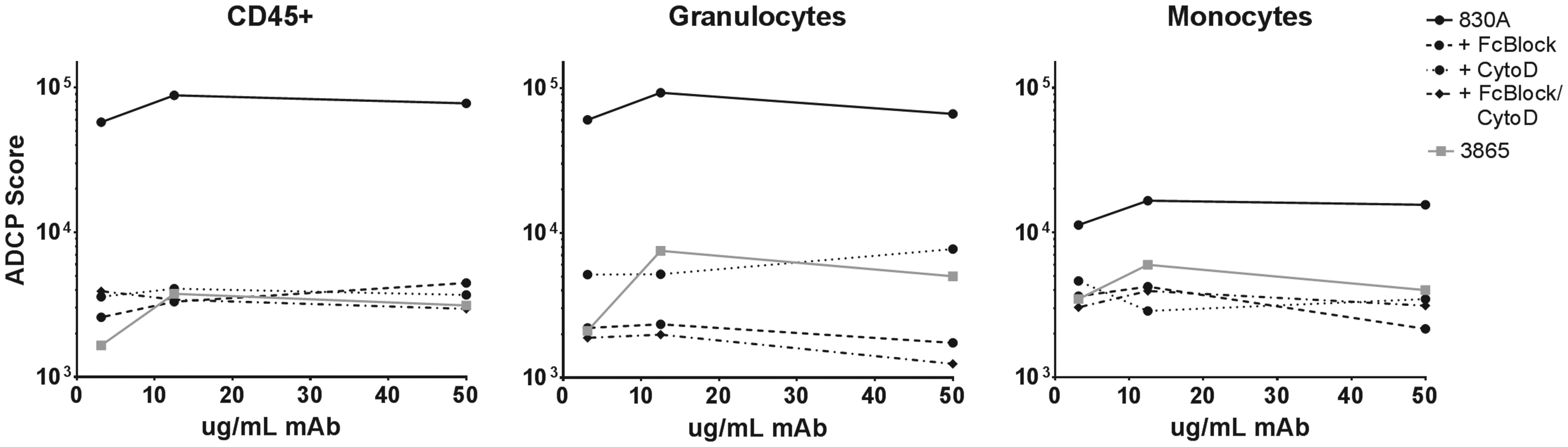
ADCP activity by BM leukocytes requires actin dynamics and FcR engagement. The ADCP assay performed is based on the assay adapted from the study by Ackerman et al. 49 ADCP target beads were incubated with dilutions of HIV V2i-specific human mAb 830A (black circles) or negative control anthrax-specific human mAb 3865 (gray squares). Plates were washed and 50,000 freshly isolated BM cells were added. For control experiments, actin inhibitor CytoD, FcBlock, or a combination of both was preincubated with cells before their addition to immune complexes. Cells were then treated, stained, and analyzed as in Figure 1. ADCP activity (bead-positive cells) was measured in the FITC channel. ADCP scores were calculated as follows: [(MFI of bead-positive cells) × (% of total CD45+ cells in the positive population)]. The data shown are from an experiment using BM sample 4 collected 31 days postpartum. ADCP, Ab-dependent cellular phagocytosis; CytoD, cytochalasin D; FcBlock, FcR-blocking agent; FcR, Fc receptor; HIV, human immunodeficiency virus; mAb, monoclonal antibody.
ADCP activity by BM leukocytes during early and mature lactation appears largely driven by granulocytes
Cells were purified from BM samples derived from different women at 7, 12, 29, and 183 days postpartum and assessed for ADCP activity (Fig. 3A). CD45+ leukocytes present in all samples exhibited specific ADCP, at least fivefold above background, mediated by both granulocytes and monocytes (Fig. 3B, C), as seen for the initial sample tested (Fig. 2). For all five samples, ADCP scores at each mAb concentration were used to determine AUC values to better compare the datasets (Fig. 3D). AUC values were variable, but largely consistent, across the samples studied, exhibiting ≤4-fold difference from lowest to highest activity for total CD45+ cells (Fig. 3D). Granulocyte activity was similarly consistent, while monocyte ADCP ranged ∼20-fold from the lowest to the highest activity measured. It was quite evident that the majority of ADCP activity in every sample analyzed was dominated by granulocytes. Of the total CD45+ activity, 72–95% was mediated by granulocytes, while the remaining minority of ADCP was monocyte driven (Fig. 3E). When granulocyte and monocyte ADCP activities across all samples were compared, AUC values for granulocytes were significantly higher than those for monocytes (p = 0.0159; Fig. 3F).
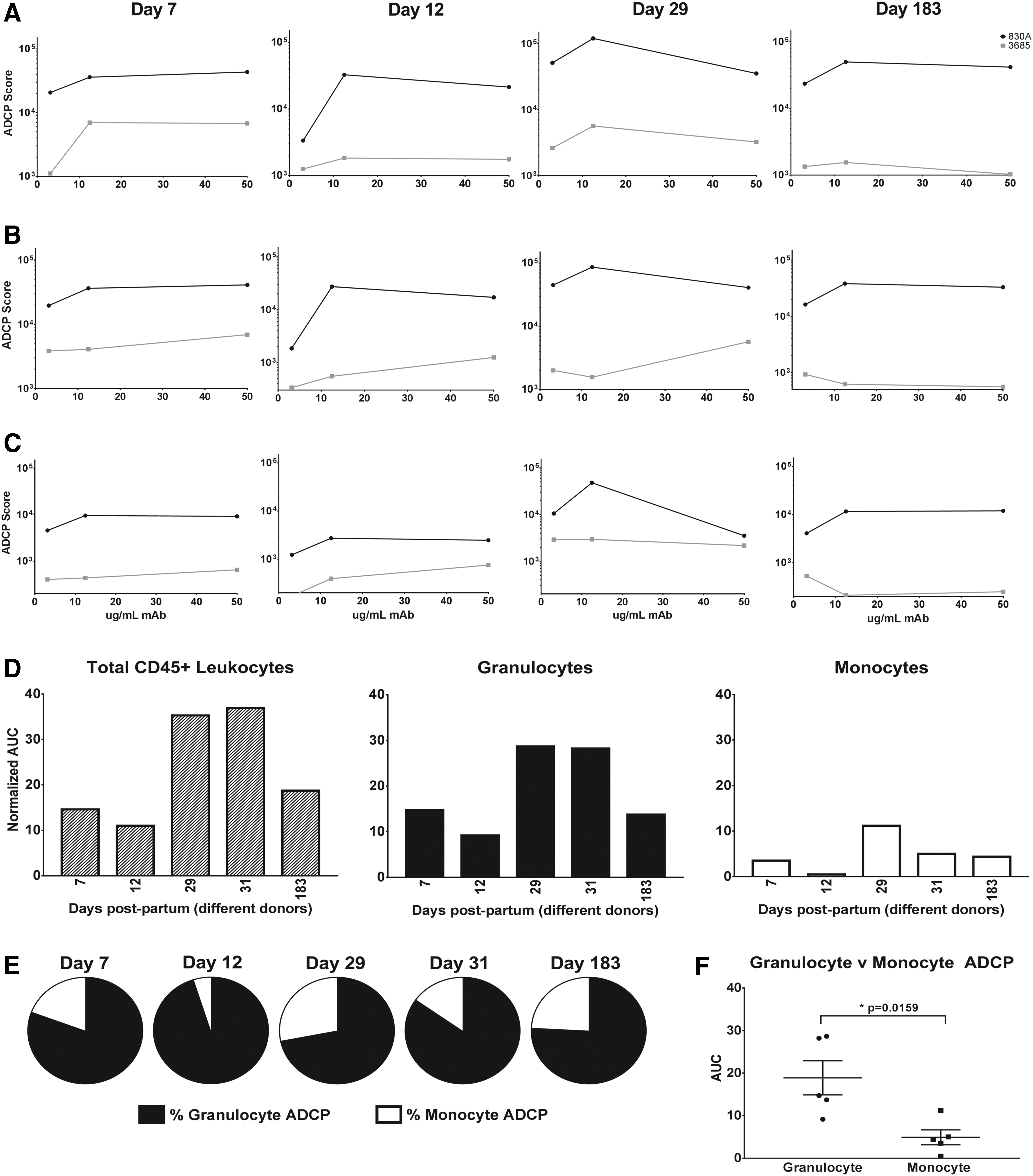
ADCP activity by BM leukocytes is largely driven by granulocytes. The ADCP assay was performed and analyzed using four BM samples obtained at the times designated postpartum. ADCP activities mediated by anti-HIV mAb 830A (
Discussion
This pilot study demonstrates that a highly sensitive, flow cytometry-based technique is useful for measuring the ADCP activity of primary BM leukocytes obtained at various time points postpartum. 49 Previous studies of Fc-mediated functionality by BM cells have been largely limited to measurement of oxidative bursts or histology-based phagocytosis assays using cells isolated from colostrum (0–4 days after birth). Virtually no studies have examined cells in human BM past the colostrum phase. Studies using colostral cells have generally concluded that the granulocytes in colostrum are less active than those isolated from blood, behaving as exudate cells that have moved into the extravascular space, 54 although conflicting studies have reported similar phagocytic and bactericidal capacities. 55 Similarly, analyses comparing colostral granulocyte and monocyte ADCP have been conflicting and likely assay and target dependent, with certain data demonstrating that monocytes were highly functional compared with granulocytes, 56 while separate studies have demonstrated similar activities for the two cell types. 55 Colostral monocytes have been found to release a greater superoxide burst compared with granulocytes, especially against opsonized pathogens. 55 The present data strongly suggest that BM-mediated ADCP is largely performed by granulocytes—assumed to be neutrophils—irrespective of the stage of lactation, although this may be a feature of the target size/type and/or the Ab isotype/subclass used.
Past the colostral stage, human BM contains ∼10 3 –10 4 leukocytes per milliliter,21–25 and it has been shown recently that as BM matures over the first month, the neutrophil concentration increases. 26 Importantly, various animal studies have demonstrated that maternal leukocytes in BM are functional and migrate within the infant to the liver, thymus, spleen, and lymph nodes and lymphocytes, in particular, appear to home to Peyer's patches of the newborn's intestines.28–32 Intact leukocytes certainly cross from the stomach of the infant despite the acidic environment and are likely an important defense against infection and possible key factors for teaching the newborn immune system, with at least 0.1% of cells ingested from milk infiltrating the peripheral tissues. 57 Notably, neutrophils of newborn humans during days 1–3 of life are functionally diminished compared with those of an adult, and deficiencies in newborn lymphocyte function have also been noted.32,33 The potent ADCP by granulocytes noted in the present study suggests a critical role for BM leukocytes in early protection from infection.
The correlates of protection found for the RV144 HIV vaccine study demonstrate that we must focus on designing a vaccine capable of eliciting highly functional Abs that can trigger relevant leukocytes through FcRs to destroy the virus, kill infected cells, and restrict viral spread. In humans, neutrophils comprise >50% of leukocytes in the blood and are key gatekeepers that can rapidly phagocytose pathogens. 58 The key protective functions of human neutrophils are mediated by a unique repertoire of FcRs that act by highly specialized coordinated mechanisms. These essential gatekeeper cells are numerous and active not only in blood but also in mucosal tissues relevant to transmission of HIV. 58 Neutrophils are a critical first line of defense against essentially all pathogens, likely including HIV, although this has been relatively poorly studied. Indeed, analysis of the influence of neutropenia on HIV-1 susceptibility has shown an ∼3-fold increased risk of HIV-1 acquisition, 59 and in studies of neutrophils in HIV-infected mothers and their newborns, infant neutrophil counts of infected infants were significantly lower than those of uninfected infants, with every 1,000-cell per microliter increase in the infants' neutrophil counts being associated with an 11% reduction in infection risk. 60
The signals generated and activities elicited by a given FcR type are determined, in part, by the Ab subclass, isotype, and isoform. Moreover, different FcRs deliver different signals. Most FcγRs have a measurable affinity for all IgG isotypes, although selectivity for a given isotype certainly exists. 61 For example, IgG3 has been shown to be a potent inducer of ADCP by monocytes, and the RV144 clinical HIV vaccine trial identified a correlate of reduced risk of HIV infection with V2-specific IgG3 Abs.35,62 Binding to most FcγRs requires the Ab to be part of an immune complex, and in this form, both IgG1 and IgG3 bind all FcγRs comparably, with only a slightly better binding profile exhibited by IgG3. 61 Notably, IgA is vastly dominant in BM, although studies have found colostral neutrophils to lack the FcαR signaling domain, reducing their IgA/Fc-mediated activities; however, this has not been studied among other cell types or in mature BM.58,63–66 Furthermore, when considering ADCP by BM leukocytes, there are various target sizes to consider, including free virions, virus/Ab immune complexes, and infected cells, as MTCT of HIV through BM occurs through both free virus and infected cells.2,67 It is evident that a large study using additional Ab isotypes, variably sized targets, and samples obtained throughout the lactation period is essential to develop a comprehensive understanding of ADCP by these relevant primary cells.
Conclusions
The data presented above establish a role for antiviral activities of BM phagocytes working in conjunction with HIV-specific human Abs, and further studies of the function of BM cells and the optimal conditions for assessing these activities will allow the field to better understand the contribution of BM cells and Abs in reduction of MTCT of HIV as well as other pathogens.
Footnotes
Acknowledgments
The authors thank Dr. Susan Zolla-Pazner, Professor in the Department of Medicine and Department of Microbiology at the Icahn School of Medicine at Mount Sinai, for manuscript review. The NIH/NICHD provided funding for this project under grant number R21 HD095772-01A1. In addition, R.L.R.P. was supported by funds from the Department of Medicine, Division of Infectious Diseases, Icahn School of Medicine at Mount Sinai.
Disclosure Statement
No competing financial interests exist.