
Abstract
Abstract
Backgrounds:
The effect of breastfeeding on weight status of individuals after a large-scale natural disaster in a developed country is unclear. We aimed to investigate the association of breastfeeding with childhood overweight and/or obesity in areas affected by the Great East Japan Earthquake.
Materials and Methods:
From health examination records of 15,563 children, we retrospectively obtained anthropometric and feeding practice (formula, mixed, and breastfeeding) data during early childhood. According to their age at the time of the earthquake, we subdivided the children into study groups 1 (42–48 months), 2 (18–24 months), and 3 (<3 months). Overweight, obesity, and underweight were defined on the basis of body mass index. To assess the association between feeding practice at 3 months of age and the risk of overweight and/or obesity at 3 years of age, we developed generalized linear mixed models that included a random effect of the municipality of residence; for this analysis, we combined “mixed feeding” and “formula feeding” into a single category: “mixed plus formula feeding.”
Results:
Mixed- plus formula-fed children had a significantly higher risk of overweight and/or obesity than breastfed children in all three study groups (odds ratios, 1.20–2.22; all p ≤ 0.047). The rate of underweight at 3 years of age was ≤0.3%, irrespective of feeding practices.
Conclusion:
Breastfeeding, even during a large-scale natural disaster in a developed country, maintained its protective effect against overweight and/or obesity in childhood.
Introduction
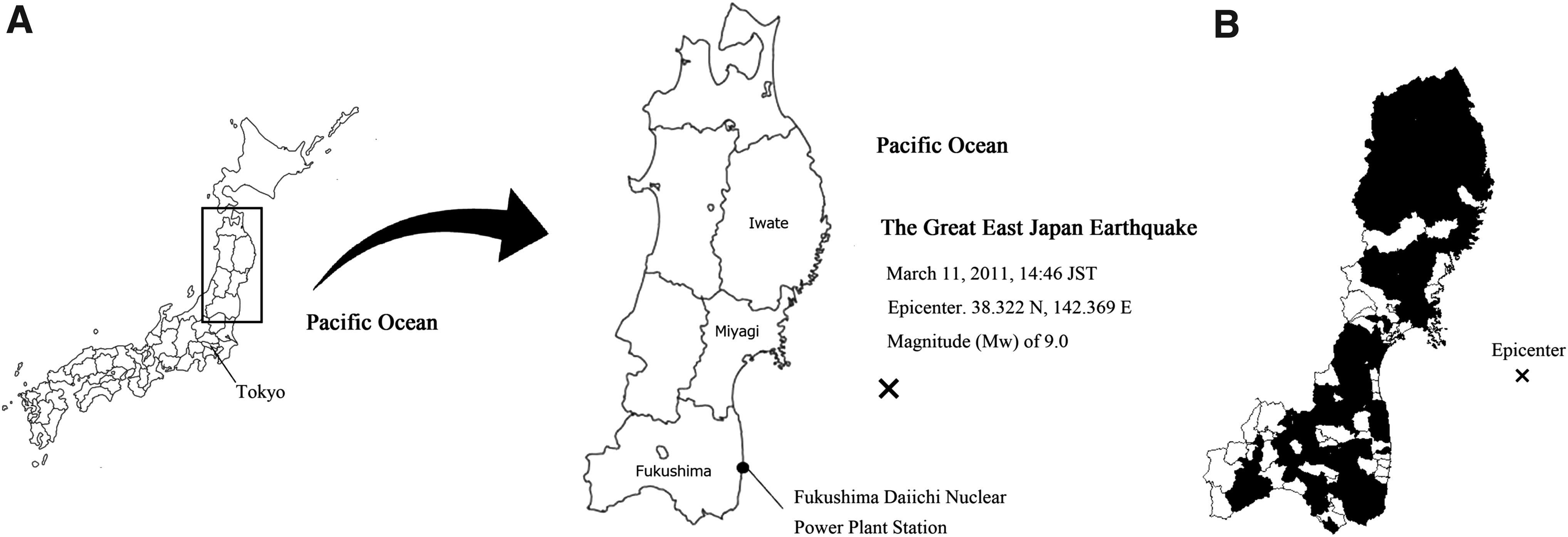
On March 11, 2011, the Great East Japan Earthquake (GEJE) and the subsequent huge tsunami wreaked massive damage on the Pacific coastal areas of northeast Japan (Fig. 1). This earthquake registered a magnitude (Mw) of 9.0, and it created >400,000 refugees. 1 As of March 1, 2017, the number of victims (dead and missing) was estimated at 22,233, with most of this impact occurring in three prefectures: Iwate, Miyagi, and Fukushima. 2 Vital infrastructure assets such as the systems supplying electric power, water, and gas were severely damaged in these affected areas. Fortunately, electric power supply, water supply, and gas lines were restored to 90% of the pre-earthquake levels in 6, 36, and 35 days, respectively. However, although such services were gradually restored in most of the damaged areas, the coastal areas in the most heavily damaged prefectures remained without these systems for a longer period. 3 Taking into consideration this large-scale natural disaster, the World Health Organization (WHO) specifically recommended that mothers continue to breastfeed their very young children in the same manner as in ordinary circumstances because breast milk substitutes could be more dangerous due to poor hygiene, lack of clean water and fuel, and unreliability of supplies. 4
Obesity in childhood is recognized as a serious public health concern because it is associated with the incidence of many serious health conditions in adulthood, such as coronary heart diseases. 5 Obese children >3 years of age could correspondingly have a much higher risk of adulthood obesity. 6 Although numerous studies on the association between breastfeeding and childhood obesity have been conducted, whether breastfeeding has protective effects against overweight and/or obesity remains controversial.7–13 Furthermore, the association between breastfeeding and overweight and/or obesity in Japanese school-age children8,9 at ordinary times and the effect of the GEJE on the risk of overweight and/or obesity in toddlers affected at 3–5 years of age14,15 have been reported; however, the effect of the GEJE on breastfeeding and latent risk of overweight and/or obesity is poorly documented. Therefore, it is unclear whether breastfeeding affects weight status after a large-scale natural disaster in a developed country.
The purpose of our research was to investigate the association between breastfeeding and the risks of childhood overweight and/or obesity at 3 years of age each in the different age before and after the GEJE.
Materials and Methods
Study design
This study employed data from the Health Examination Survey on Early Childhood Physical Growth in the GEJE Affected Areas, which was conducted for a 3-year period from July 2012 to October 2014. Details of these surveys are reported elsewhere. 16 In Japan, most municipalities provide regular health examinations to children during their early childhood in accordance with the Mother and Child Health Act. In 2015, the 3-year-old health examination was performed in children in 95.5% of the municipalities in Japan. 17 From these health examination records, we retrospectively retrieved the data accumulated in 80 of the 127 municipalities (63.0%) in three disaster-stricken prefectures. We analyzed the data from 79 municipalities, which provided data accumulated for the 3-year period; the municipal of Sendai city—the largest city in the three prefectures—was excluded since only 1-year data were available. Ethical approval was obtained from the Institute Review Board of Tohoku University Graduate School of Medicine (No. 2012-1-125). The requirement of informed consent from participants was waived due to the retrospective nature of data collection.
Participants
Health Examination Survey on Early Childhood Physical Growth in the GEJE Affected Areas 16 included children who were born between June 1, 2010 and April 30, 2011. From these, we selected children from the most damaged three prefectures for whom 3-year-old health examination data were available. In this study, we stratified the collected data into three study groups with respect to birth dates (Fig. 2). Study group 1 comprised 11,960 children who were born between March 1, 2007 and August 31, 2007. They had experienced the GEJE just before or after their health examination, indicating that they were affected at 42–48 months of age by the GEJE. Study group 2 comprised 13,554 children who were born between March 1, 2009 and August 31, 2009, indicating that they were affected at 18–24 months of age by the GEJE. Study group 3 comprised 8,132 children who were born between January 1, 2011 and April 30, 2011, indicating that they were affected at <3 months of age by the GEJE.
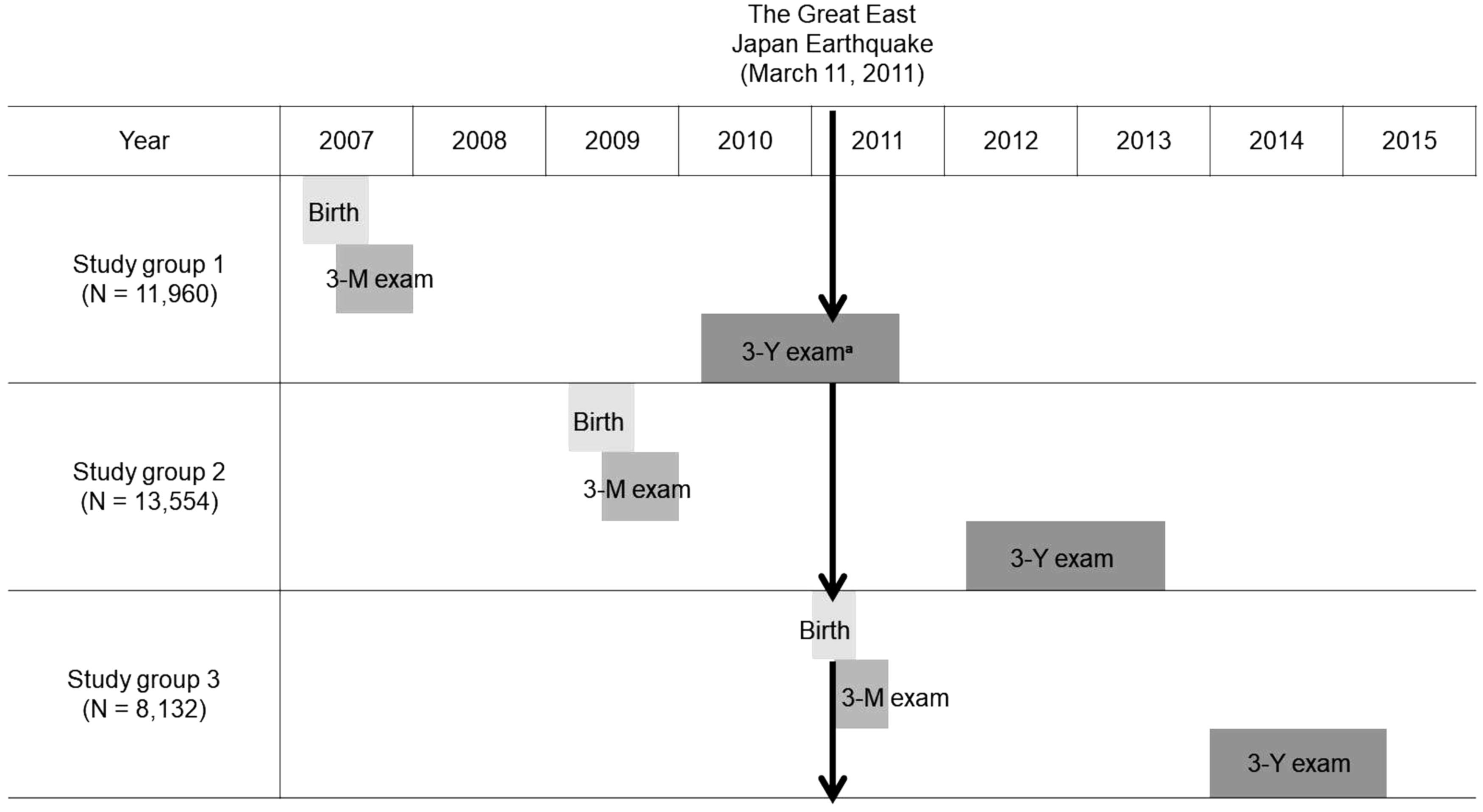
Timeline of birth and health examinations. Study groups 1, 2, and 3 comprised children who were affected at 42–48, 18–24, and <3 months of age by the GEJE, respectively. 3-M exam: health examination at 3–4 years of age. 3-Y exam: health examination at 3 years of age. aNo children in this study underwent a 3-Y exam after the GEJE. GEJE, Great East Japan Earthquake.
Children who were ≥3–4 months of age, who were born between January 1, 2011 and April 30, 2011, and who had a “normal” health examination were included in this study (Fig. 3). Children with nonoptimal gestational terms (<37 weeks, ≥42 weeks, or missing data); those with low birth weight (<1,500 g or missing data); those with missing data regarding feeding practices at 3–4 months of age; those who did not routinely undergo health examination; and those for whom any data of age, height, or weight were missing were excluded. Unfortunately, data from Morioka city—the largest municipality in Iwate Prefecture—were excluded since data of feeding practices were not available. Finally, a total of 15,563 children were analyzed, comprising 6,308, 7,044, and 2,211 in study groups 1, 2, and 3, respectively.
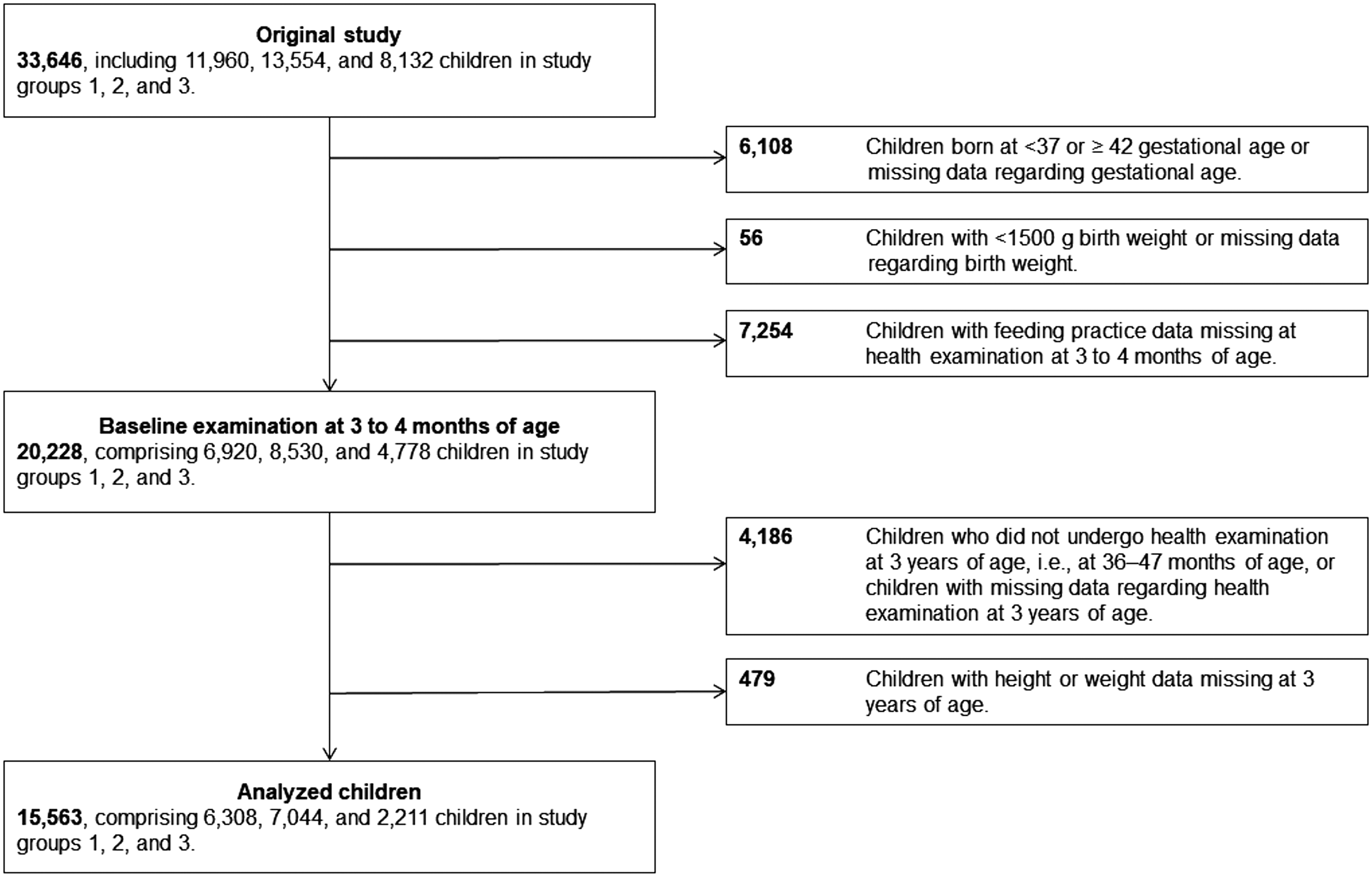
Flowchart for the selection of participant children. Study groups 1, 2, and 3 comprised children who were affected at 42–48, 18–24, and <3 months of age by the GEJE, respectively. GEJE, Great East Japan Earthquake.
Survey items
We used the following survey items: gender, gestational age, birth weight, municipality of residence, anthropometric data, and feeding practice (breastfeeding, formula, or mixed feeding). Data of gender, gestational age, birth weight, and feeding practice were collected through health examinations, and the municipality of residence was determined as municipality in which the 3-year-old health examination was conducted. Anthropometric data of height and weight at both 3–4 months and 3 years of age were used. Data of feeding practice were determined by interviews with mothers conducted by medical staff or health nurse employed by each municipality and were recorded as practice at 3–4 months of age. If the percentages of breastfeeding were roughly >80%, 20–80%, and <20%, feeding practices were generally defined as breastfeeding, mixed feeding, and formula feeding, respectively. 18
Definitions of overweight, obesity, and underweight
We defined overweight, obesity, and underweight on the basis of body mass index (BMI) criteria of the International Obesity Task Force.19,20 The cutoff points were determined on the basis of the age- and gender-specific BMI: 25 kg/m 2 for overweight, 30 kg/m 2 for obesity, and 16 kg/m 2 for underweight, at 18 years of age. To determine the cutoff points for 3.0-, 3.5-, and 4.0-year-old children in this study, we linearly interpolated each child's age as of the 3-year-old health examination. 19
Statistical analysis
We used chi-squared test to compare the significance of categorical variables among the three groups. To calculate the odds ratios (ORs) and 95% confidence intervals (CIs) for the association of feeding practice at 3–4 months of age with the risk of overweight and/or obesity at 3 years of age, we developed and fitted generalized linear mixed models by gender and study groups. Because the impact of the earthquake, tsunami, and Fukushima Daiichi Nuclear Power Plant accident varied substantially across the affected municipalities, we computed the model with a logit link function that included a random effect for the municipality of residence but used feeding practice as a fixed effect, specifying the category of “breastfeeding” for each study group as the base reference. To evaluate the effect on mainly breastfed children, we combined mixed feeding and formula feeding into a single category: “mixed plus formula feeding.” In the sensitivity analyses, we repeated the analyses, excluding birth weight <2,000 g children. We furthermore conducted the analyses in the similar manner, using birth weight (categorical value; 1,500–2,499, 2,500–3,999, and ≥4,000 g) for confounding factor. All statistical analyses were performed using SAS software version 9.4 (SAS Institute, Inc., Carey, NC), and the significance level was defined as <0.05 in two-tailed tests.
Results
Gender, birth weight, and feeding practice percentages at 3–4 months of age were not significantly different from the baseline between the analyzed children (N = 15,563) and excluded children (N = 4,665) in each study group (all p ≥ 0.31 for gender, all p ≥ 0.21 for birth weight, and all p ≥ 0.07 for feeding practice) in Figure 3. In contrast, there were differences in prefecture between analyzed and excluded children (all p < 0.001). The characteristics of the analyzed children are presented in Table 1. The rate of low birth weight and breastfeeding at 3–4 months of age was slightly higher in study group 3 than in other study groups. Interestingly, rates of breastfeeding at 3–4 months of age were 38%, 40%, and 41% in study groups 1, 2, and 3, respectively.
Characteristics of Analyzed Children by Study Groups
Study groups 1, 2, and 3 comprised children who were affected at 42–48, 18–24, and <3 months of age by the GEJE, respectively. p-Values were computed by chi-squared tests.
Feeding practices were determined in health examination at 3–4 months of age.
GEJE, Great East Japan Earthquake.
BMI category at 3 years of age is presented in Table 2. The rate of overweight and/or obesity at 3 years of age in breastfed children was lower than that in children fed using other practices in all study groups regardless of gender. In addition, the rate of underweight at 3 years of age was ≤0.3% in all categories and approximately equal across all three groups.
Body Mass Index Category in Health Examination at 3 Years of Age According to Study Group and Feeding Practice in Health Examination at 3–4 Months of Age
Study groups 1, 2, and 3 comprised children who were affected at 42–48, 18–24, and <3 months of age by the GEJE, respectively. The cutoff points were based on the age- and gender-specific BMI: 25 kg/m 2 for overweight, 30 kg/m 2 for obesity, and 16 kg/m 2 for underweight, at 18 years of age. Using the cutoff points of 3.0-, 3.5-, and 4.0-year-old children on the basis of the International Obesity Task Force,18,19 we linearly interpolated participants' age in health examination at 3 years of age.
BMI, body mass index; GEJE, Great East Japan Earthquake.
The mixed- plus formula-fed children had a significantly higher risk of overweight and/or obesity than the breastfed children across gender and study groups (ORs, 1.20–2.22; all p ≤ 0.047). Interactions between study group and feeding practice were not significant (boys: p = 1.00 (reference) for study group 1, p = 0.86 for study group 2, and p = 0.30 for study group 3; girls: p = 1.00 (reference) for study group 1, p = 0.81 for study group 2, and p = 0.089 for study group 3). In particular, children in study group 3 showed a higher risk of overweight and/or obesity than those in the other groups regardless of gender (Table 3). There were no significant interactions effects between genders (all p ≥ 0.20 for interaction) and among prefectures (all p ≥ 0.080 for interaction). After excluding <2,000 g children (ORs, 1.20–2.22; all p ≤ 0.045) or adjusting for birth weight (ORs, 1.22–2.23; all p ≤ 0.034), there were minor differences in the results.
Association Between Feeding Practice (Breastfeeding Versus Mixed Plus Formula Feeding) and Overweight and/or Obesity at 3 Years of Age Study Groups
Study groups 1, 2, and 3 comprised children who were affected at 42–48, 18–24, and <3 months of age by the GEJE, respectively. ORs and 95% CIs were calculated using generalized linear mixed models to adjust for clustering within municipalities. Feeding practices were determined in health examination at 3–4 months of age. The breastfeeding category for each study group was used as a reference.
CIs, confidence intervals; GEJE, Great East Japan Earthquake; ORs, odds ratios; Ref., reference.
Discussion
We analyzed the association between feeding practices and weight status at 3 years of age in the disaster-stricken areas. This study demonstrated that breastfed children, even in the context of a large-scale natural disaster, had a reduced risk of overweight and/or obesity than mixed- and formula-fed children.
These results show that continuing breastfeeding mainly for 3 months after birth could have a protective effect against overweight and/or obesity not only in ordinary times but also just after a large-scale natural disaster in a developed country. Nonetheless, whether breastfeeding has a protective effect against overweight and/or obesity even in ordinary times remains controversial.7–12 Previous systematic reviews conducted by the WHO 7 suggest that breastfeeding could have a protective effect against overweight and/or obesity; however, recent studies from Sweden, 10 the Netherlands, 11 and Hong Kong 12 did not report any such effect. However, the difference in the results obtained in the studies conducted in Japan8,9 and those from other countries10–12 can be attributed to ethnic or cultural differences in lifestyles, such as the duration of breastfeeding, timing and ingredients of solid food introduction, and habit of smoking during pregnancy.8,10,21
Several mechanisms can be proposed to explain our findings. First, hormones present in breast milk, such as leptin, adiponectin, and ghrelin, reduce excess appetite. 22 Second, bottle feeding decreases an infant's ability to self-regulate milk intake as they grow up. A previous study has indicated that the feeding mode (bottle versus breast) may be more important than the type of milk in the bottle. 23 Third, formula milk is generally considered to contain higher protein content than breast milk. Two randomized controlled trials have indicated that nutrient-enriched formula produces faster weight gain in infancy and increased fat mass later in childhood. 24
The WHO, United Nations Children's Fund, and American Academy of Pediatrics emphasize the importance of breastfeeding in emergencies owing to its protective effects against respiratory and infectious diseases, including diarrhea.4,25 Immediately after GEJE, United Nations Children's Fund and other support groups released a joint statement for guidelines on infant nutrition in disaster-stricken areas. 26 In our study, the proportion of breastfed children who were born just before or after the GEJE was considerably greater than other study groups. A survey conducted in Fukushima Prefecture has reported similar results. 27 The results indicated that governments or other related organizations should establish campaigns encouraging breastfeeding not only just after the disaster but also during ordinary times, which may be effective for maintaining the proportion of breastfeeding even after a large-scale natural disaster.28,29 Ministry of Health, Labour, and Welfare in 2007 30 and Japan Pediatric Society in 2011 18 published guidelines for promoting breastfeeding. In actuality, breastfeeding rate in Japan was increasing from 38.0% in 2005 to 54.7% in 2015. 31
To the best of our knowledge, there has been no report regarding the latent risk of overweight and/or obesity in children after a large-scale natural disaster in a developed country, and our study appears to have several particular strengths. First, the sample size is large, which includes victims from a large affected area. Our analyses were based on regular health examination data from 80 of the 127 municipalities in Iwate, Miyagi, and Fukushima prefectures, which were conducted in accordance with the Mother and Child Health Act. 32 Therefore, almost all children in the participating municipalities could be included in our study. As shown in Figure 1B, there was no obvious deviation in the geographical distribution of municipalities, and particularly no deviation was observed in the distribution between coastal and inland area. Furthermore, all anthropometric and feeding practice data were measured by medical staff at the time of health examinations. Regular health examination records were employed in the study because we believe they are more suitable for evaluating anthropometric data in the same manner before and after the GEJE. Second, we used a generalized linear mixed model to adjust for clustering within municipalities. By nesting within municipalities, we were able to analyze the association between breastfeeding and overweight and/or obesity because impacts of the GEJE, including the subsequent huge tsunami, and Fukushima Daiichi Nuclear Power Plant accident as well as the potential differences in lifestyle and environmental factors could have varied across the municipalities of residence.
There are several limitations in our study, which was based solely on health examination records. For this reason, our findings should be interpreted with caution. First, the differences in characteristics from the baseline between the analyzed and excluded children could have affected the results. However, the percentages of gender, birth weight, and feeding practice at 3–4 months of age were not significantly different from the baseline between the analyzed and excluded children. Second, we could not obtain potentially important birth information, such as birth order, mode of delivery (vaginal or caesarean delivery), and single or multiple births. However, these omissions may have minor influence on the results because the children included in our study were those with a normal gestational age of 37–41 weeks and birth weights >1,500 g. Third, we could not obtain information regarding the socioeconomic status of the mothers, such as household income, education level, employment status, and smoking status. A study from European countries has shown that the children of parents with a lower socioeconomic status may have a higher risk of developing unhealthy eating habits. 33 In contrast, two studies from Japan have shown results similar to ours regardless of adjusting for socioeconomic status.8,9 Consequently, we are confident that this particular omission had little if any impact on our results.
Conclusion
In conclusion, breastfeeding young children, even during a large-scale natural disaster in a developed country, maintained its protective effect against overweight and/or obesity at 3 years of age.
Footnotes
Acknowledgments
This survey was conducted as a part of the “Surveillance study on child health in the GEJE disaster area.” This survey was supported in full by funding from the Health and Labour Sciences Research Grant (H24-jisedai-shitei-007, fukkou).
Disclosure Statement
No competing financial interests exist.