
Abstract
Abstract
Background:
Most mothers in the United States express their milk, which is then bottle fed to their infants. The National Immunization Survey (NIS), used to report national breastfeeding prevalence, asks about infant breast milk consumption, regardless of whether it is consumed at the mother's breast or from a bottle. The NIS data are often erroneously interpreted, however, to mean prevalence of at-the-breast feeding. We hypothesized that over half of infants classified as breastfed at 3, 6, and 12 months by the NIS questions would also be consuming expressed breast milk.
Materials and Methods:
A convenience sample of 456 mothers of infants 19–35 months of age recruited through ResearchMatch.org completed an online infant-feeding questionnaire. The questionnaire included both the NIS questions and more-detailed questions about feeding mode, distinguishing between at-the-breast and bottle.
Results:
Based on responses of our sample to the NIS questions, it could be interpreted that 74%, 64%, and 39% of mother–infant dyads were at-the-breast feeding at 3, 6, and 12 months, respectively. However, at each time point, most infants consumed at least some breast milk from a bottle. As infants got older, the proportion of breast milk consumed from a bottle increased.
Conclusions:
In this U.S. sample, the predominant breast milk feeding style involves both at-the-breast and expressed breast milk feeding. Future research and national surveillance should consider including separate measures of maternal breast milk expression and infant consumption of expressed breast milk to enable meaningful exploration of maternal and infant outcomes associated with these asynchronous behaviors.
Introduction
It is well established that infant formula is associated with worse infant outcomes1–3 than breastfeeding as traditionally defined, namely an infant suckling milk from his or her mother's breast. Studies have shown beneficial outcomes for infants fed directly at their mothers’ breast versus infants fed formula from a bottle.4–11 Thus, health organizations worldwide promote what has been considered to be “breastfeeding.”12,13 However, with the wide availability of efficient electric breast pumps, and the high proportion of mothers working outside the home, 14 a significant proportion of mothers now express their breast milk, which is then fed from a bottle.15,16 Thus, the dichotomous classification of infants as breastfed or bottle-fed, with bottle-fed signifying the feeding of infant formula, is no longer completely accurate, and the meaning of the word breastfeeding has become unclear.17–20
The national breastfeeding surveillance tool in the United States, the National Immunization Survey (NIS), has been used to monitor and report breastfeeding prevalence since 2001. 21 However, the NIS questions ask only about infant breast milk consumption, regardless of whether breast milk was consumed at the mother's breast or from a bottle. Given that the NIS questions ask how long an infant was “breastfed or fed breast milk,” this could be taken to mean a combination of at-the-breast feeding and expressed breast milk feeding. However, the NIS data are often interpreted, erroneously, to mean the prevalence of at-the-breast feeding.12,22 This is problematic because maternal breast milk production and infant breast milk consumption are no longer synchronous behaviors. 19
It is important to understand and recognize the complexity of breast milk feeding practices because recently published data associated infant expressed breast milk consumption with higher infant growth velocity during the first year of life,5,6,11 higher risk of wheezing and coughing, 7 increased risk of otitis media, 9 lower satiety responsiveness in children, 4 and less desirable children's eating behavior at 6 years of age 8 when compared with feeding directly at the breast. It is possible that other outcomes differ by infant breast milk consumption mode, but that they remain to be studied. Given that 85% of mothers of infants 1.5 to 4.5 months of age who responded to the Infant Feeding Practices Study II (IFPS II, 2005–2007) 23 reported that they had expressed their milk at some time and 25% reported doing so on a regular schedule, the infant health outcomes associated with these feeding behaviors warrant further study.
Our primary aim in this research was to compare alternative infant-feeding questions, which include indicators for maternal breast milk expression and infant expressed breast milk consumption, with the current NIS questions—which do not elicit data about maternal breast milk expression or infant breast milk consumption—to determine whether the prevalence of feeding behaviors differs depending on the questions asked. Based on the prevalence of maternal breast milk expression observed on the IFPS II, 23 we hypothesized that most mothers in our sample would have expressed their milk at some time and more than 50% of infants who were classified as breastfeeding at 3, 6, and 12 months by the NIS questions would have been consuming breast milk both at the breast and from a bottle. We also aimed to explore the discordance between the duration of maternal breast milk production and infant breast milk consumption, and the timing of cessation of infant formula consumption.
Materials and Methods
Data collection
We conducted a cross-sectional, online questionnaire that included the NIS questions, an alternative set of infant-feeding questions (the Questionnaire on Infant Feeding [QIF]), and demographic questions. The QIF (Supplementary Table S1) asked about the timing of initiation and cessation of several behaviors: at-the-breast feeding, maternal breast milk expression, infant expressed breast milk consumption, infant formula consumption, the timing of introduction of foods or liquids other than breast milk or infant formula, instances of breast milk sharing, and the frequency of maternal breast milk expression. A description of the development, construct validity testing, and reliability testing of the QIF has been published elsewhere. 24 Participants could respond in days, weeks, months, or a combination of these; we recoded responses into days for analyses. We also asked categorical, closed questions about the mode of feeding (breast/bottle) at 3, 6, and 12 months postpartum and the proportion of breast milk infants consumed from a bottle. The QIF included a prompt encouraging mothers to think carefully and respond as accurately as possible.
We recruited participants through ResearchMatch, a U.S. national health volunteer registry supported by the National Institutes of Health as part of the Clinical Translational Science Award program. 25 Between March and July 2015, we contacted all women in the registry between 18 and 50 years of age with a message that invited mothers of children 19–35 months of age to complete a questionnaire about infant and child feeding. The child's age range was chosen to mimic the sampling strategy of the NIS. Those interested clicked a link in the e-mail, which gave ResearchMatch permission to release their contact details to the investigators. We then e-mailed mothers a personalized link to the questionnaire. The first page of the questionnaire explained the purpose of the study; respondents were informed that participation was voluntary and confidential and asked for their agreement to participate. Respondents clicked a button labeled “I AGREE” to begin the questionnaire. Respondents were considered to have consented to participate when they began to complete the questionnaire. All mothers were eligible to participate, whether they ever fed breast milk or not. The questionnaire was only offered in English. We compensated participants with a $5 electronic gift card, e-mailed to them within 24 hours of questionnaire completion. This protocol was approved by the Cornell University's Institutional Review Board.
Data cleaning
We modified or removed implausible and logically impossible responses to questions about maternal and infant behaviors and demographic characteristics during data cleaning. In some cases, implausible responses (n = 10) appeared to be typographical errors; we manually altered these to the more plausible response. For example, one participant responded “no” to the NIS question “Was [child] breastfed or fed breast milk?” but all other responses—to both the NIS questions and the QIF questions—indicated that the child was fed breast milk, so this response was modified to “yes.” In cases where there was no obvious correct response (13 responses to individual questions), we set values to missing. We excluded participants with internally inconsistent responses. Internally inconsistent responses included participants who indicated that they stopped a behavior (e.g., expressing breast milk) before they started it (n = 20), participants who reported continuing a feeding behavior for longer than their child had been alive (n = 4), and participants whose responses were inconsistent across the two feeding questionnaires (NIS and QIF; n = 4).
Variable creation
With the NIS questions, we used continuous responses to create dichotomous variables indicating whether the infant was “breastfed or being fed breast milk” at 3, 6, and 12 months. For example, if a mother responded to the question “How old was [child's name] when [child's name] completely stopped breastfeeding or being fed breast milk?” with “7 months,” then the infant was coded as “breastfed or being fed breast milk” at 3 and 6 months, but not at 12 months. Similarly, we used continuous responses to the QIF questions to create dichotomous variables indicating whether the mother–infant dyad was at-the-breast feeding, whether the mother was expressing breast milk, and whether the infant was consuming expressed breast milk at 3, 6, and 12 months. For example, the two questions “If day 0 is the day [child] was born, how old was he/she when he/she was first fed directly from your breast?” and “Thinking only about feeding directly from your breast, if day 0 is the day [child] was born, how old was he/she when he/she completely stopped feeding directly from your breast?” (QIF questions available in the Supplementary Table S1) were used to determine whether a child was consuming milk at-the-breast at 3, 6, and 12 months.
Data analyses
First, we calculated the proportion of mothers who ever expressed breast milk. Second, we used the responses to the NIS questions to calculate the proportion of infants who were consuming any breast milk at 3, 6, and 12 months, and exclusively consuming breast milk at 3 and 6 months. We then compared these proportions with responses to the QIF questions that distinguish between at-the-breast consumption of breast milk and expressed breast milk consumption.
We explored the discordance between the duration of maternal breast milk production and infant breast milk consumption and the timing of cessation of infant formula consumption using descriptive statistics. All analyses were conducted using SAS version 9.3 software (SAS Institute, Inc., Cary, NC).
Results
Eight hundred ninety-three people expressed interest in this research and were e-mailed the questionnaire; the questionnaire was completed by 496 respondents (Fig. 1). Before conducting the present analyses, we assessed the construct validity and reliability of our questionnaire 20 and reported that a small number of participants had incompatible responses across the two surveys; these participants (n = 8) were excluded from the present analyses. We also excluded participants who had questionable responses discovered during data cleaning (n = 28) and those who provided demographic information but did not complete infant-feeding questions (n = 4) from the final analyses. Thus, final analyses include 456 participants (92%, 456/496).

Flowchart of participants in the questionnaire on infant feeding, 2015.
Most respondents were white, non-Hispanic, 30 years of age or older, married, normal weight, had at least a bachelor's degree, and had children who did not participate in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) (Table 1). Although we aimed to recruit mothers of infants between 19 and 35 months of age, some of the respondents had younger (∼4%) and some had older (∼13%) infants. Infants in the sample were born in 2011, 2012, and 2013.
Demographic Characteristics of Participants in the Questionnaire on Infant Feeding 2015, Total n = 456
At survey completion.
Based on participant-initiated self-report.
BMI, body mass index; WIC, the Special Supplemental Nutrition Program for Women, Infants, and Children.
Maternal breast milk expression and infant breast milk consumption
Of the breast milk feeding mothers surveyed, 94% ever expressed their milk, and the majority (51.5%) of breast milk feeding mothers expressed several times every day. Most mothers (∼75% of the total sample) used a mixed-mode feeding style, including at-the-breast feeding and at least some expressed breast milk feeding (Fig. 2). Fewer than 10% of all mothers only ever fed breast milk solely at the breast (Fig. 2, Column 2). A small proportion of respondents reported that their infants only ever consumed expressed breast milk (∼3%) and for a few of the respondents (n = 4), the only breast milk their child consumed was another mother's milk (Fig. 2). The NIS questions do not ask about maternal breast milk expression or infant breast milk consumption; as such, we cannot report the prevalence of these behaviors based on this questionnaire.
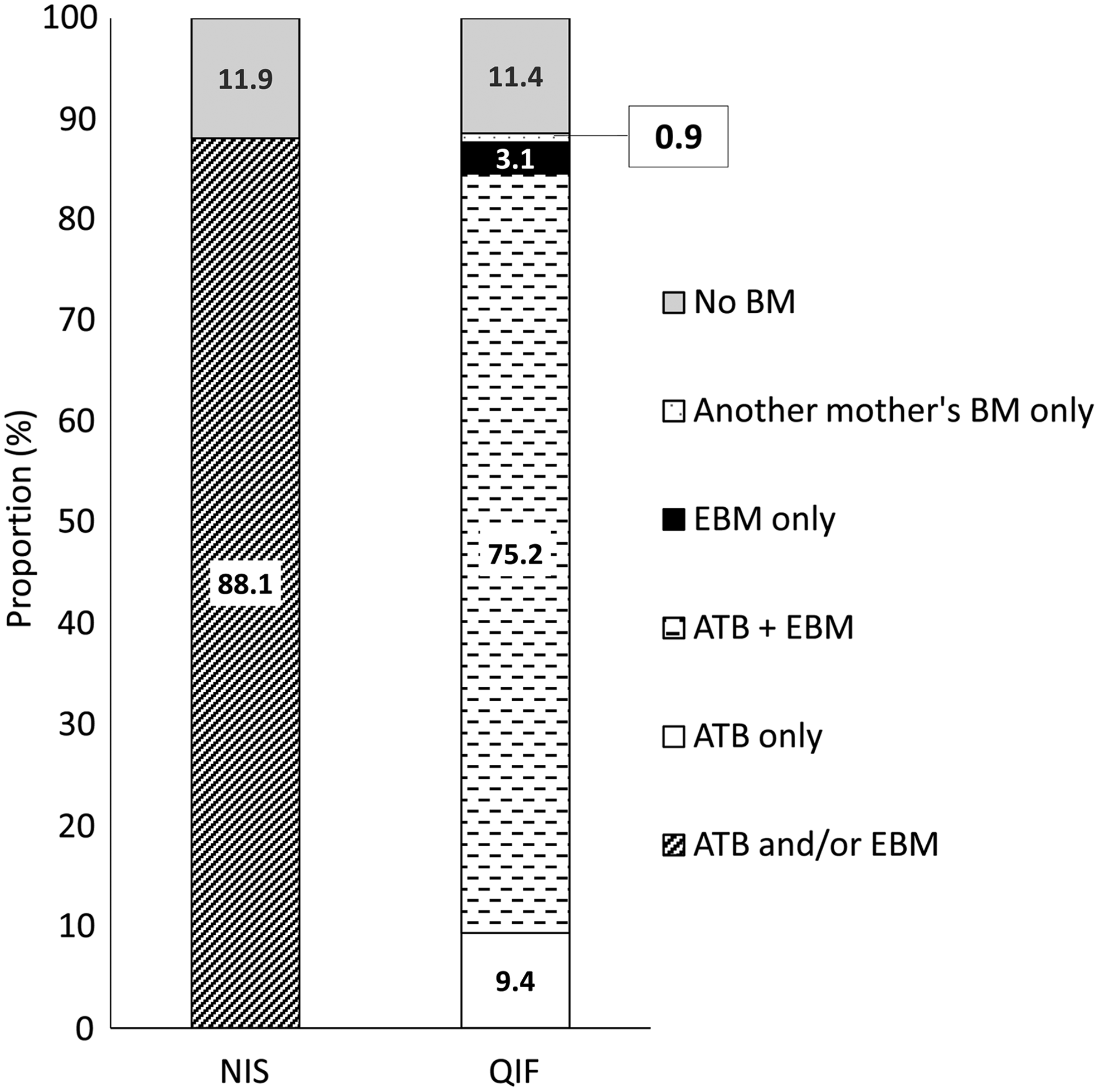
Proportion of infants in the QIF (2015) ever fed breast milk by question type (NIS versus QIF), calculated using responses to questions about timing of initiation and cessation of feeding behaviors. ATB, at-the-breast; BM, breast milk; EBM, expressed breast milk; NIS, National Immunization on Survey; QIF, Questionnaire on Infant Feeding.
The proportion of infants consuming breast milk at 3, 6, and 12 months is roughly the same when measured by the NIS and the QIF (Fig. 3). However, using the additional data collected in the QIF, we can report that of the infants who consumed breast milk at 3, 6, and 12 months, most consumed both at the breast and expressed breast milk (Fig. 3), making a mixed-mode style the predominant feeding style across the infant's first year—confirming our hypothesis. Prevalence of exclusive breast milk consumption at 3 and 6 months was similar regardless of question type (NIS: 22.6% and 8.1%, respectively, versus QIF: 19.5% and 6.1%, respectively).
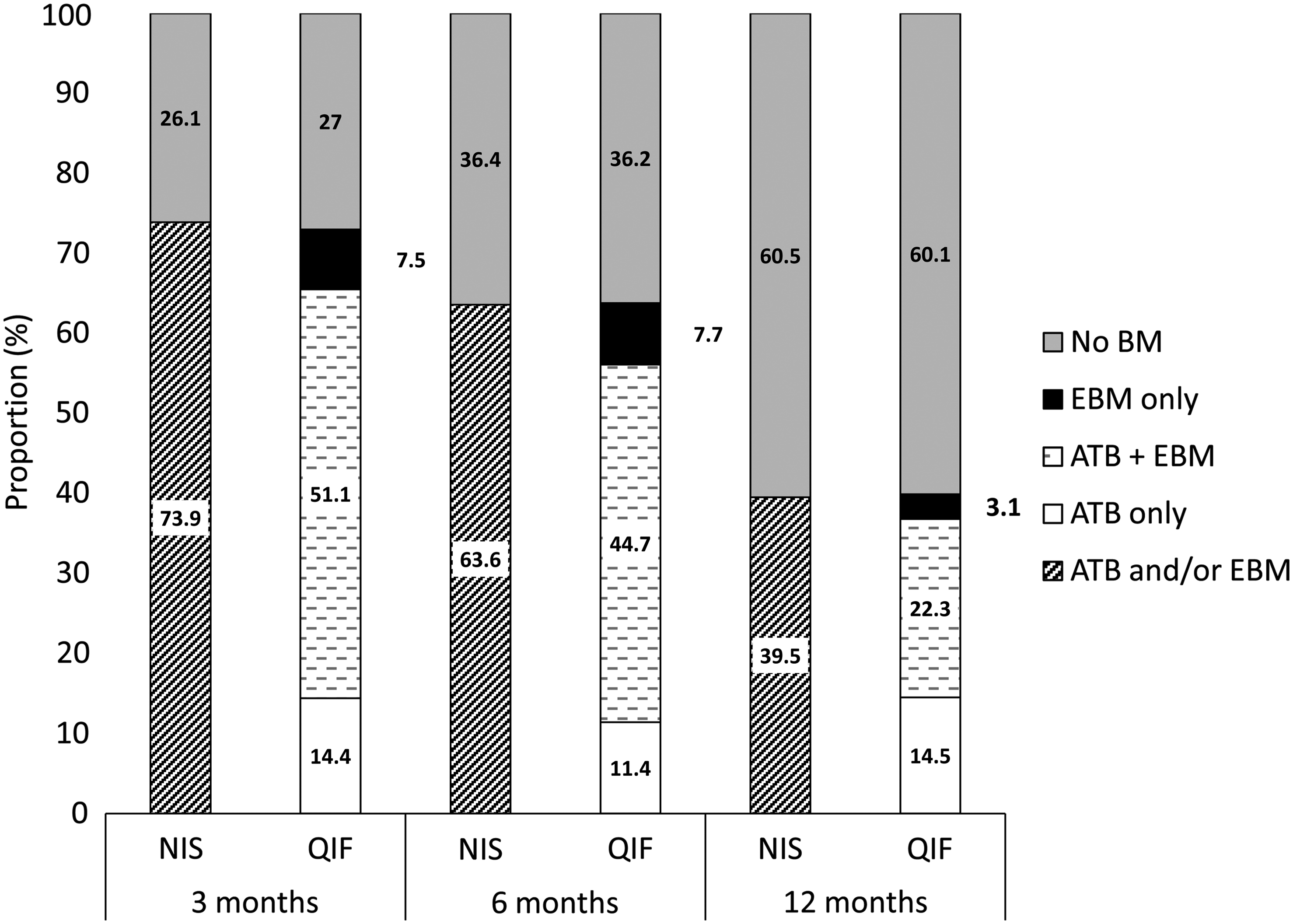
Prevalence of breast milk feeding at 3, 6, and 12 months in the Questionnaire on Infant Feeding (2015) by question type (NIS versus QIF), calculated using responses to questions about timing of initiation and cessation of feeding behaviors.
Based on responses to a categorical question about the proportion of expressed breast milk consumed at different times throughout infancy, at 3 months postpartum, nearly 70% of breast milk feeding mothers reported that their infants consumed at least some breast milk from a bottle (Table 2). However, at-the-breast feeding was the predominant breast milk feeding mode at 3 months. At 6 and 12 months postpartum, the proportion of infants who consumed breast milk from a bottle increased, as did the proportion of breast milk they received from a bottle relative to at-the-breast (Table 2).
Mode of Breast Milk Feeding in the First Year Postpartum Among Breast Milk Feeding Participants in the Questionnaire on Infant Feeding, 2015
Values are percent of the total number of mothers who reported breast milk feeding on this question. See Supplementary Table S1 for full text of question from which these data are obtained.
Participants were free to interpret the words “mostly” and “some” as they felt appropriate.
ATB, at-the-breast; EBM, expressed breast milk.
Additional behaviors of public health interest
Of the breast milk feeding mothers in this sample, 36 (10.1%) continued to feed their infants expressed breast milk for at least 4 weeks after they stopped lactating. The median duration of infant breast milk consumption after cessation of maternal lactation—among those who continued to feed their infant expressed breast milk for at least 4 weeks after cessation of maternal lactation—was 57 (range 28–162) days. Of those women whose infants consumed expressed breast milk for at least 4 weeks after cessation of maternal lactation, 58% (n = 21) provided answers to the NIS questions that reflected the shorter duration of maternal breast milk production and not the duration of infant breast milk consumption, which is the focus of the NIS questions. The remaining 42% (n = 15) provided answers to the NIS questions that reflected duration of infant breast milk consumption.
The majority (75%) of mothers reported that their infant ever consumed infant formula in response to the QIF. Of these, 5.2% of infants (n = 17) received infant formula for 3 days or less. Six of these mothers with a short duration of infant formula feeding reported that their infant never consumed infant formula in response to the NIS questions, but subsequently reported feeding infant formula on the more-detailed questionnaire.
Discussion
Our results indicate that a mixed-mode breast milk feeding style—combining both at-the-breast feeding and expressed breast milk feeding—is the predominant breast milk feeding style among a large sample of U.S. mothers. Given that a mixed-mode breast milk feeding style is the predominant feeding style, and that expressed breast milk feeding may not confer the same benefits as at-the-breast feeding, the health outcomes associated with this feeding mode warrant in-depth study.
At all times across infancy that we explored, the predominant breast milk feeding strategy included both at-the-breast feeding and expressed breast milk feeding. If the NIS questions are interpreted literally, as the duration a child was “breastfed or fed breast milk,” then most infants in our sample would be correctly classified by the NIS as it stands now. However, the NIS questions do not accurately reflect the behavior of the mothers only feeding at the breast or the infants only consuming expressed breast milk. For example, based on responses of women in our sample to the NIS questions, it could be interpreted that 74%, 64%, and 39% of all mother–infant dyads were breastfeeding at 3, 6, and 12 months, respectively. However, at 3, 6, and 12 months 14.4%, 11.4%, and 14.5% of infants, respectively, were consuming breast milk solely at the breast and 7.5%, 7.7%, and 3.1% of infants were consuming expressed breast milk only. The prevalence of exclusive expressed breast milk consumption observed among our sample is comparable with a recent report of a cross-sectional study from one geographic location. 26
This less-extensive classification of maternal and infant behaviors by the NIS questions is important because public health authorities 12 recommend that women breastfeed. This recommendation is based on associations of breastfeeding with positive maternal and infant outcomes 2 —associations based on studies comparing infants fed at the breast with those fed infant formula from a bottle. However, most mothers feed infants at the breast and express their milk, and thus most infants are fed breast milk both at the breast and from a bottle; the latter feeding style may modify the benefits of at-the-breast feeding and could even be associated with negative infant outcomes.
Our results not only describe the complexity of breast milk feeding, but also the complexity of measuring these behaviors. When dichotomous variables were created from responses to questions with continuous responses, ∼14% of dyads were classified as solely at-the-breast feeding at 3 months postpartum. In contrast, when asked a categorical question specifically about the proportion of breast milk fed at the breast, ∼30% of dyads were classified as solely at-the-breast feeding at 3 months postpartum. This difference likely occurs because expressed breast milk feeding may be an episodic behavior; for example, a mother may choose to express enough milk to spend a few nights away from her infant but may only feed at the breast when they are together. Thus, it is insufficient to ask only about the initiation and cessation of this behavior to describe, for example, the behavior of an infant who started consuming expressed breast milk before 3 months, stopped after 3 months, but was only fed at the breast at 3 months of age.
The difficulty in measuring breast milk production and consumption behaviors highlighted in this study is essential for investigators to consider when developing studies to explore maternal and infant outcomes related to maternal lactation and infant breast milk consumption. Take, for example, the association between breastfeeding and the development of the infant gut microbiome. Compared with formula feeding, breastfeeding is associated with development of a more favorable infant gut microbiome,27,28 which itself is associated with reduced risk of metabolic and immune diseases. 27 However, infants who consume expressed breast milk may develop a gut microbiome than is less favorable than that of the infant who consume milk at the breast. This is because practices for storing and reheating expressed breast milk 29 can decrease the pH and change the bacterial profile of the milk. 30 Thus, the proportion of expressed breast milk consumed would be an important exposure to measure when exploring the complex relationships among infant feeding, the gut microbiome, and infant health outcomes.
The other feeding behaviors of public health interest that we explored, about which no national data are collected, suggest a possible need for revision of the current national breastfeeding surveillance questions. Based on formative qualitative data, 19 we predicted that some infants would continue consuming breast milk after their mothers had stopped producing breast milk. Although this occurred, most mothers of infants who continued to consume expressed breast milk after their mother had stopped lactating provided answers to the NIS questions that reflected their own duration of lactation, which underestimates the infant's duration of breast milk consumption. This finding supports the need for more specific questions for measuring infant feeding.
In this study, when presented with questions about both the initiation and cessation of infant formula feeding, 6 (1.3%) mothers who had previously indicated that their child never consumed infant formula provided information about formula feeding. This is important for two reasons. First, investigators may misclassify infants as never formula fed if they only ask about initiation of infant formula feeding. Second, when mothers in a study we previously conducted were not offered the opportunity to provide a timing of infant formula cessation, they were frustrated, 21 which may be sufficient justification for collecting the data.
Strengths and limitations
A strength of this study is the development of the questionnaire based on formative qualitative research.19,31 Questions were rigorously tested to ensure they were contextually appropriate and reliable. Additionally, by administering the questionnaire online to a large sample from a wide geographic area, we verified the inferences we drew from our smaller qualitative study, conducted in a single geographic location.19,31 The similar conclusions drawn from these studies, particularly the finding that a mixed-mode breast milk feeding style is the predominant feeding style, supports the generalizability of these findings, despite the fact that we surveyed a convenience sample of women.
However, because we administered this questionnaire online to a convenience sample of mothers recruited through ResearchMatch.org, 25 we have no proof that our respondents were indeed mothers of infants between 19 and 35 months of age. We addressed this by conducting internal consistency checks to identify and discard implausible responses. Finally, this sample of mothers were well educated and predominantly white; selection bias may explain why infants in our sample were more likely to have consumed any breast milk during the first year of infancy than a national sample.
Conclusion
Our results highlight that the term “breastfeeding” does not adequately describe the range of contemporary infant-feeding behaviors employed by this sample of U.S. women. Most lactating mothers are expressing breast milk several times every day and most infants are consuming breast milk both at the breast and from a bottle. This is important because we know that the mode of breast milk feeding is associated with infant health outcomes, and that the mode of breast milk feeding is often not addressed on infant-feeding surveys. These results suggest that considerable thought and care must be given to devising infant-feeding questions for use in research, and that revision of current national breastfeeding surveillance questions may be warranted.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.