
Abstract
Abstract
Background:
Although current evidence suggests that there are unique benefits of breastfeeding for mothers receiving comprehensive treatment, including counseling and pharmacotherapy, for opioid use disorder (OUD) and their infants, breastfeeding rates in this population are low. Support and counseling about breastfeeding are key predictors of infant feeding behaviors. Thus, identifying knowledge and attitudes regarding breastfeeding of individuals who work in OUD treatment facilities could offer insight into targets for breastfeeding-promotion interventions in such settings.
Materials and Methods:
Individuals who work at two urban perinatal OUD treatment centers were e-mailed a link to complete a questionnaire electronically. Breastfeeding knowledge, attitudes, and perceptions of those who completed the questionnaire were described using descriptive statistics.
Results:
Among the 24 survey respondents, most correctly identified the health benefits of breastfeeding for infants with neonatal abstinence syndrome, whereas less than half correctly identified the health benefits of breastfeeding for all infants. Only 16% reported receiving work-related breastfeeding education. The leading perceived breastfeeding challenges for women in treatment for OUD were (1) concern with transfer of medication (e.g., methadone) through breast milk, (2) daily commutes for treatment, and (3) beliefs that formula is better than breastfeeding.
Conclusions:
Professionals who work in perinatal OUD treatment centers could benefit from education regarding breastfeeding in mothers in treatment for OUD.
Introduction
There is increasing evidence that breastfeeding is beneficial for infants with neonatal abstinence syndrome (NAS). In the United States, length of hospital stay is up to 42% shorter for breastfed NAS infants compared with nonbreastfed NAS infants.1,2 Shorter hospitalizations may equate to savings of >$3,000 per inpatient treatment day. 3 Among infants with NAS, breast milk intake is also associated with delayed onset and reduced severity of NAS, and decreased need for pharmacologic treatment. 4
There are also unique benefits of breastfeeding for mothers with opioid use disorder (OUD) who are receiving comprehensive treatment, including counseling and pharmacotherapy (e.g., methadone), the recommended treatment for OUD during pregnancy. 5 Enhanced maternal-infant bonding and attachment associated with breastfeeding, along with the hormone release of oxytocin during breastfeeding, may protect mothers against stress and subsequent relapse.6,7 It has also been reported that women in treatment for OUD regard breastfeeding as a facilitator in their recovery. 8 The American College of Obstetrics and Gynecologists, 5 the American Academy of Pediatrics, 9 and the Academy of Breastfeeding Medicine 10 support breastfeeding among these women if there are no contraindications to breastfeeding, and it has been recommended that breastfeeding and lactation support be incorporated into perinatal OUD treatment programming. 11 Despite the benefits of and recommendations for breastfeeding, existing data suggest that breastfeeding is not common among women in treatment for OUD. Breastfeeding initiation rates in this population range from 20% to 46%,12–15 which is considerably lower than the national rate of 83%. 16
Efforts to increase breastfeeding could be an effective mechanism to improve the trajectory of mothers in treatment for OUD and their infants. Developing breastfeeding promotion programs for these mothers remains a challenge, however, with limited information on the determinants of infant feeding decisions and behaviors in this population. Conversely, factors associated with breastfeeding in the general population have been studied extensively, and among other things, health care provider support and counseling about breastfeeding has consistently been identified as a key predictor of breastfeeding behaviors.17–21 Because women in treatment for OUD may face additional obstacles and perceived barriers to breastfeeding (e.g., past sexual trauma, fear of medication transmission, and fear of hepatitis C transmission),22,23 support from a professional within the treatment setting may be quite important among these women. However, in a recent small qualitative study of women receiving medication-assisted treatment (MAT), the majority reported that their prenatal care providers and the staff at their treatment center had not discussed breastfeeding with them during their pregnancy. 24
It may be possible that lack of awareness of current recommendations regarding breastfeeding and MAT and attitudes about breastfeeding among women with OUD influence the type and level of support a woman receives from health care and treatment staff and providers.24,25 As such, assuring that these professionals are equipped with accurate knowledge, timely information, and positive attitudes regarding breastfeeding is important. However, the level of knowledge about and attitudes toward breastfeeding have not been described previously in a population of professionals who work in perinatal treatment settings. The objective of this pilot study, therefore, was to evaluate the knowledge, attitudes, and perceptions regarding concurrent breastfeeding and maternal MAT for OUD among individuals who work in OUD treatment centers for pregnant and parenting women.
Materials and Methods
Study design and participants
This study was a descriptive cross-sectional pilot study. Investigators e-mailed information about the study, including a link to complete a questionnaire electronically, to two perinatal treatment centers from the same urban geographic area. One person from each center subsequently distributed the information and the link to individuals 18 years of age or older who worked in the treatment centers. There was no criteria for exclusion other than age <18 years. No identifiable information was recorded on the questionnaires completed by the participants. The Institutional Review Board at Thomas Jefferson University approved this study.
Data collection
The medical literature was reviewed for previously validated infant feeding-related questionnaires used with professionals in perinatal OUD treatment centers; no prior questionnaires were identified. Therefore, investigators designed the questionnaire and most of the questionnaire items. The questionnaire consisted of 40 items plus an additional 9 items that were contingent on participant's answers, and included an assessment of participant: demographic and work-related characteristics, breastfeeding knowledge and attitudes, and perceptions regarding concomitant maternal MAT and breastfeeding.
Demographics and work-related characteristics
Demographic characteristics assessed included age (25–29 years, 30–39 years, 40–49 years, and 50+ years), gender (female, male, and other), race (black, white, and other), ethnicity (Hispanic and non-Hispanic), and relationship status (married and not married). Participants were asked whether they had any children and, if yes, whether their child(ren) were ever breastfed. Participants were also asked to report work title, the number of years in their current position, whether they had ever received any breastfeeding education, and whether they ever provide breastfeeding support to and/or discuss breastfeeding with their clinic's patient population.
Knowledge, attitudes, and perceptions
Breastfeeding knowledge was evaluated with 13 multiple choice questions, some of which originated from the Infant Feeding Practice Survey. 26 Question topics included knowledge regarding the benefits of breastfeeding for all infants, the benefits of breastfeeding for infants with NAS, and current infant feeding recommendations. Knowledge questions were assessed as being answered correctly or incorrectly. A composite knowledge score, representing the percent correct of the 13 knowledge questions, was calculated for each participant. A 3-point Likert-type scale (“not at all important,” “somewhat important,” and “very important”) was used to assess provider attitudes on the importance of discussing nine maternal and infant health topics with mothers in treatment for OUD, including breastfeeding, immunizations, child development, infant car safety, infant safe sleep practices, contraception, maternal mental health, smoking, and weight gain. Lastly, participants were asked to identify what they perceived to be breastfeeding challenges for mothers receiving MAT for OUD by choosing from a list of 19 options, and subsequently asked to choose what they perceived to be the top three breastfeeding challenges for these mothers.
Statistical analyses
Frequency counts and percentages were used to describe participant demographic and work-related characteristics and responses on the knowledge, attitude, and perception items. The mean number of knowledge questions correctly answered was calculated. All statistical analyses were conducted using SAS software version 9.4 (SAS Institute, Inc., Cary, NC).
Results
Twenty-four individuals completed the electronic survey (85% response rate). The majority of respondents were female, white, non-Hispanic, and at least 30 years of age (Table 1). Half of respondents had children of their own, of which three-quarters had ever been breastfed. Most were in their current position for at least a year. Three-quarters of respondents reported that they have ever provided support and/or discussed breastfeeding with mothers in treatment for OUD. Only 16% reported ever receiving work-related breastfeeding education.
Demographic and Work-Related Characteristics of Study Participants
Note: Missing data: ethnicity, n = 2.
Among those who reported having children.
Includes administrators, case managers, social workers, and childcare staff.
In current position.
Knowledge
Less than half of respondents knew the general infant health benefits of breastfeeding, including that infants who are breastfed are generally less likely to get diarrhea (41%) and ear infections (45%; Table 2). The majority agreed that, among infants with NAS, breastfeeding was associated with reduced NAS scores (83%), treatment duration (75%), treatment dose (75%), and length of hospital stay (66%). Most respondents agreed that MAT is not a contraindication to breastfeeding, whereas only 38% agreed that tobacco smoking is not a contradiction to breastfeeding. The mean composite knowledge score was seven (range 1–13).
Knowledge of Breastfeeding Benefits and Recommendations Among Study Participants
ACOG, American College of Obstetrics and Gynecology; MAT, medication-assisted treatment; NAS, neonatal abstinence syndrome; OUD, opioid use disorder.
Attitudes
Approximately two-thirds of participants (69%) reported that talking to their clinic's patient population about infant feeding was very important (results not shown). In comparison, the proportion who reported the following as very important discussion topics was 95% for maternal mental health, 87% for infant safe sleep practices, 87% for child development, 83% for smoking, 74% for contraception, 68% for immunizations, 61% for car safety, and 44% for maternal weight.
Perceptions
The most frequently selected breastfeeding challenges for women receiving MAT for OUD were lack of breastfeeding knowledge (54%), worry about transfer of medication through breast milk (29%), lack of support from family and friends (29%), lack of support from health care providers (25%), daily commutes for methadone treatment (25%), long infant hospitalizations (21%), and other children to take care of (13%) (Fig. 1).
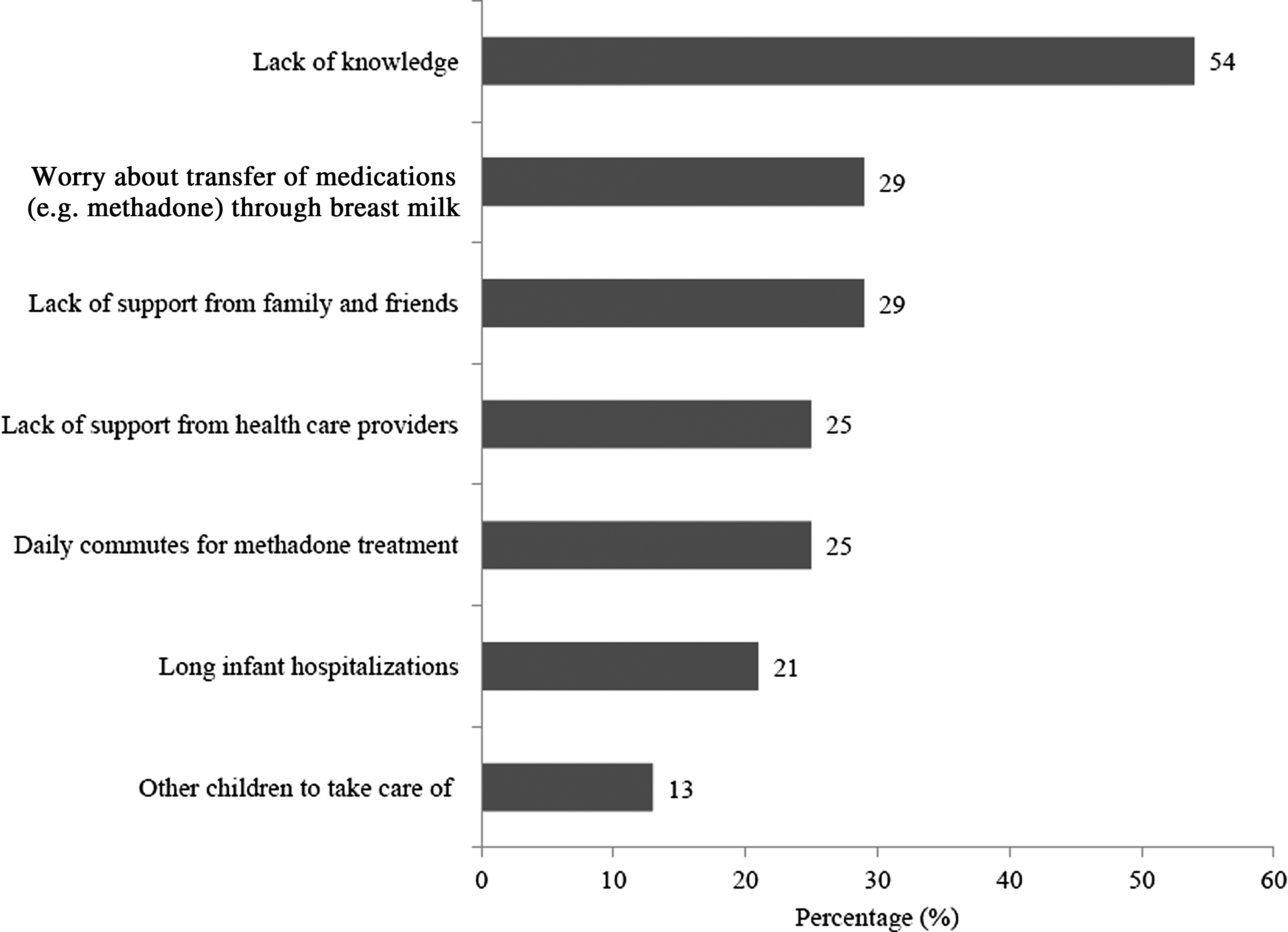
Breastfeeding challenges for mothers receiving medication-assisted treatment for opioid use disorder as reported by study participants.
Discussion
Perinatal OUD treatment centers could be a key source of support and education for expectant and new mothers who are receiving MAT for OUD. Individuals who work in such settings are in frequent, if not daily, contact with women as they present for MAT and for individual and group therapy and other psychoeducational group programs as part of their comprehensive OUD treatment. Although results from this pilot study indicate that the majority of these professionals do discuss breastfeeding with their patient population, results also suggest that individuals working in perinatal OUD treatment centers may be lacking general knowledge regarding breastfeeding benefits, recommendations, and contraindications, and do not view breastfeeding as important as other maternal-infant health issues.
Study participants were generally aware of the benefits of breastfeeding for infants with NAS, but they were far less familiar with the other protective effects breastfeeding has on infants in general (e.g., protection against obesity, diarrhea, ear infections, and respiratory illnesses). Moreover, the majority of participants incorrectly identified tobacco smoking as a contraindication to breastfeeding 27 and did not know the current recommendation that infants be fed only breast milk for the first 6 months of life. 16 This lack of knowledge could have important implications if inaccurate information is being shared with their patient population. Understanding the benefits of breastfeeding and receiving information from clinical providers have both been reported as motivators to breastfeed among women in treatment for OUD,8,24,28 although whether OUD treatment centers provide the same level of influence is not known. However, based on our findings, within the context of OUD treatment, women may not be receiving accurate and appropriate information regarding the benefits and recommendations of breastfeeding, which could subsequently impact their infant feeding decisions. As such, efforts to improve knowledge about breastfeeding among professionals in perinatal MAT programs, therefore, may be warranted. The need for such efforts is further supported by this study's finding that only 16% of respondents had ever received breastfeeding education. Educational initiatives targeting health care providers have been associated with improved staff beliefs about and practices toward breastfeeding and subsequent increased rates of breastfeeding among patient populations,29,30 and it is possible that such initiatives could similarly effect those working in treatment settings.
Our study also indicates that professionals in perinatal OUD treatment centers rate the importance of other maternal-infant health topics, including maternal mental health, infant safe sleep practices, child development, smoking, and contraception, higher than the importance of breastfeeding. It may be possible that the high prevalence of poor mental health, smoking and unintended pregnancies in women with OUD,11,31 concerns about physical health and development among opioid-exposed infants, and the complexity of other challenges mothers with OUD often face influence how professionals perceive these topics. Lack of skill and inadequate time needed to manage infant feeding issues could also affect perceived importance, and it is not all that surprising that other topics receive more attention. Still, due to the significant benefits breastfeeding has for all mothers and babies, focusing on breastfeeding should be a higher priority.
It may also be that study participants did not feel comfortable discussing breastfeeding because they did not know what the real challenges were for their clients. Participants of this study perceived barriers to breastfeeding to be predominantly knowledge deficits rather than structural or relational barriers (e.g., other children and prolonged infant hospitalizations). How these align with patient-reported challenges is difficult to evaluate due to the limited literature on breastfeeding challenges and concerns in women with OUD. Small single-site qualitative studies among women in treatment have identified lack of support from the health care community, misinformation, infant hospitalization, and past sexual trauma as significant barriers to breastfeeding success.8,22,24 Larger studies are needed to further explore patient-reported challenges unique to mothers in treatment for OUD so that individuals who work with these mothers can better anticipate such barriers and assist women with overcoming them.
Limitations of this pilot study include the small convenience sample and recruitment from a single geographical area, which limits generalizability of findings. In addition, because of the level of anonymity in this survey, it is unclear how the treatment facilities contacted were represented among the respondents and if between-site differences existed. Social desirability bias may have been present, although bias was likely minimized given the questionnaires were self-administered and anonymous. Lastly, the small sample size prevented us from ascertaining the association between participant characteristics and outcomes. Future studies with a larger and/or more diverse sample could allow for a more complete psychometric analyses of the questionnaire items, and as well as a more thorough analysis of the impact of variables such as years of experience, clinical training, and level of patient interaction on outcomes.
Despite these limitations, this pilot study provides novel information regarding breastfeeding knowledge, attitudes, and perceptions of individuals who work in perinatal OUD treatment centers. Findings can be used to develop larger studies and future educational interventions or quality improvement initiatives with the goal of improving professionals' breastfeeding knowledge and attitudes to ultimately increase breastfeeding among women in treatment for OUD.
Footnotes
Acknowledgments
The authors would like to thank all study participants.
Disclosure Statement
No competing financial interests exist.