
Abstract
Abstract
Objective:
We examined the influence of maternal body mass index (BMI), and of breast and nipple anatomic variations, on breastfeeding difficulties and duration.
Methods:
In this prospective observational study, we collected demographic and anthropometric data from 109 mothers of full-term newborns. Women were classified as underweight, normal weight, overweight, and obese using the World Health Organization definitions and were otherwise healthy. Breast anthropometrics assessments were recorded after delivery and during hospitalization. Latching difficulties were collected as reported by the mothers. Breastfeeding duration was assessed by phone interview at 3, 6, 1 year, or more postdelivery.
Results:
The four prepregnancy BMI groups included 12 underweight, 59 normal weight, 20 overweight, and 18 obese women. The higher the BMI group, the larger the breast was (p = 0.005). In univariate regression, nipple diameter, nipple length, and areola diameter correlated significantly with breast size. The overall rate of latching difficulties was 15.5%, without significant differences among all four BMI groups. In multivariate analysis, the higher the BMI group the lower was the likelihood of breastfeeding at 6 months of age (odds ratio [OR] = 0.88, 95% confidence interval [CI]: 0.79–0.99), and the higher the birth order the higher was the likelihood of breastfeeding at 6 months of age (OR = 3.36, 95% CI: 1.44–7.83). Early latching difficulties predicted shorter breastfeeding duration.
Conclusion:
We conclude that high prepregnancy BMI has a negative impact on breastfeeding initiation and duration.
Introduction
Breastfeeding difficulties at the initiation of breastfeeding during the first few days of life are a strong predictor of breastfeeding failure and of short breastfeeding duration (<6 months).1,2 Obese women experience many breastfeeding difficulties,3–5 have lower breastfeeding initiation rates,6,7 and shorter breastfeeding duration7–9 than nonobese women. Maternal anatomic factors have been implicated in the success of breastfeeding, with a negative impact of large breasts 10 and a positive impact of long nipples. 11
We, therefore, conducted the following prospective and observational study. We examined in a relatively large sample of subjects, the influence, if any, of maternal body mass index (BMI), a widely accepted estimate of maternal adiposity, and of breast and nipple anatomic variations, upon breastfeeding difficulties and breastfeeding duration. We tested the hypotheses that (1) high BMI, large breasts, and short nipples are independent risk factors for difficulties at the initiation of breastfeeding and (2) the abovementioned factors, when they lead to initial breastfeeding difficulties, predict shorter breastfeeding duration.
Methods
Sample population
Mothers of full-term newborn infants were enrolled for this study at the Lis Maternity Hospital of the Tel Aviv Medical Center, Tel Aviv, Israel. The study was approved by our local Institutional Review Board and written informed consent was obtained from the mothers. One hundred nine breastfeeding mothers, recruited between December 2013 and February 2016, were followed up after delivery. Criteria for exclusion were maternal diabetes, gestational hypertension, any chronic disease, and intake of medications other than prenatal vitamins and minerals. Similarly, mothers were excluded if their children had any postnatal complications that required admission to the neonatal intensive care unit. Mothers who delivered by cesarean delivery but were otherwise healthy were not excluded.
We systematically recorded demographic and anthropometric data from the mothers, to the inclusion of maternal age on the day of delivery, gestational age (by last menstrual period (LMP) and ultrasound (US)), mode of delivery, parity, ethnic origin, self-reported prepregnancy weight and height, maternal weight on the day of delivery (before the delivery itself), weight gain during pregnancy, and infant gender, and birth weight (BW). Maternal BMI was calculated as prepregnancy weight/height 2 and expressed as kg/m2. Women were classified as underweight (BMI <18.5), normal weight (BMI 18.5–25), overweight (BMI 25.1–29.9), and obese (BMI 30 or more) using the World Health Organization definitions. 12
Breast anthropometrics assessment
After delivery and during hospitalization, breast size of recruited mothers was recorded (based on the Bra database classification: bratabase.com, 12 and nipple length and diameter and areola diameter were measured using a Ribbon Centimeter Band (single use centimeter from Agit, www.aguda.co.il). Whenever relevant, the presence of sore nipples and the use or not of a silicone nipple were noted.
Breastfeeding duration assessment
Recruited mothers were contacted by phone at different time points postdelivery (3, 6 months, and >1 year), and exclusive breastfeeding duration was assessed until that time.
Statistical analyses
The Minitab Statistical Package, version 16 (Minitab, State College, PA), was used for analyses. Descriptive statistics (mean and standard deviations [SDs]) were calculated for demographic data and breast shape. Univariate analyses using Kruskal–Wallis tests were applied to reveal the possible contribution of BMI, breast size, and nipples size in difficulties at the initiation of breastfeeding. Backward stepwise logistic regression analysis was conducted to judge the effect of BMI, breast size or shape, nipple size, and self-reported breastfeeding difficulties (sore nipples and/or use of silicone nipples and/or difficulties in latch) at the initiation of breastfeeding upon duration of breastfeeding. Results are expressed as mean ± SD if normally distributed and as median and range otherwise.
Results
Major demographic characteristics of the population are depicted in Table 1. All recruited mothers were Caucasian. In brief, the four BMI groups did not differ significantly in terms of maternal age, height, gestational age, or years of education. The underweight mothers had a lower parity than the other three groups (p < 0.05 by analysis of variance [ANOVA] with Bonferoni correction). As expected, the four groups differed in terms of prepregnancy weight and BMI. Weight gain was significantly lower in the obese group than in the other three groups (p = 0.05). BW correlated weakly but significantly with maternal BMI (R 2 = 0.072, p = 0.005).
Maternal and Neonatal Characteristics by Body Mass Index Group
Data are presented as mean ± SD (median, range) or n (%).
BMI, body mass index; SD, standard deviation.
Table 2 depicts the anthropometric analyses per BMI group of breast size, and of nipple and areola dimensions. In brief, by ANOVA, the higher the BMI group the larger the breast (p = 0.005). In contrast, the percentage of protruding nipples or that of flat nipples did not differ among groups. There were no significant differences among groups in nipple diameter or length, but the areola diameter was significantly smaller in the underweight group than in the three other BMI groups (p < 0.05, by ANOVA with Bonferoni correction). In univariate regression, breast size correlated with nipple diameter (R 2 = 5.7%, p = 0.014), areola diameter (R 2 = 4.6%, p = 0.029), and nipple length (R 2 = 3.9%, p = 0.045).
Breast Anthropometric Data Per Body Mass Index Group
NA, not assessed.
The overall rate of latching difficulties was 15.5%, without significant differences among all four BMI groups. However, 58.7% of women did not answer the question on latching difficulties, and the sample size in the overweight and obese groups dropped to only six participants (Table 3). In univariate analyses (Kruskall–Wallis), there were no significant differences between women experiencing latching difficulties and those who did not in terms of maternal age, parity, gestational age, BW, education, maternal height, prepregnancy weight, BMI, breast size, or areola diameter or nipple diameter or length. A total of 14 patients were lost to follow-up and we were not able to determine in these mothers the duration of exclusive breastfeeding (Table 4).
Reported Difficulties at the Initiation of Breastfeeding in Mothers with Complete Follow-Up
Duration of Breastfeeding
FU, follow-up.
In the remaining 95 mothers with complete follow-up until 6 months, 71.4% of mothers who did not report latching difficulties were still exclusively breastfeeding at 6 months, as compared with only 28.6% of those who experienced initial latching difficulties (p = 0.034), (Fig. 1). Sore nipples and use of silicone shields were not significant predictors of exclusive breastfeeding at 6 months of age.
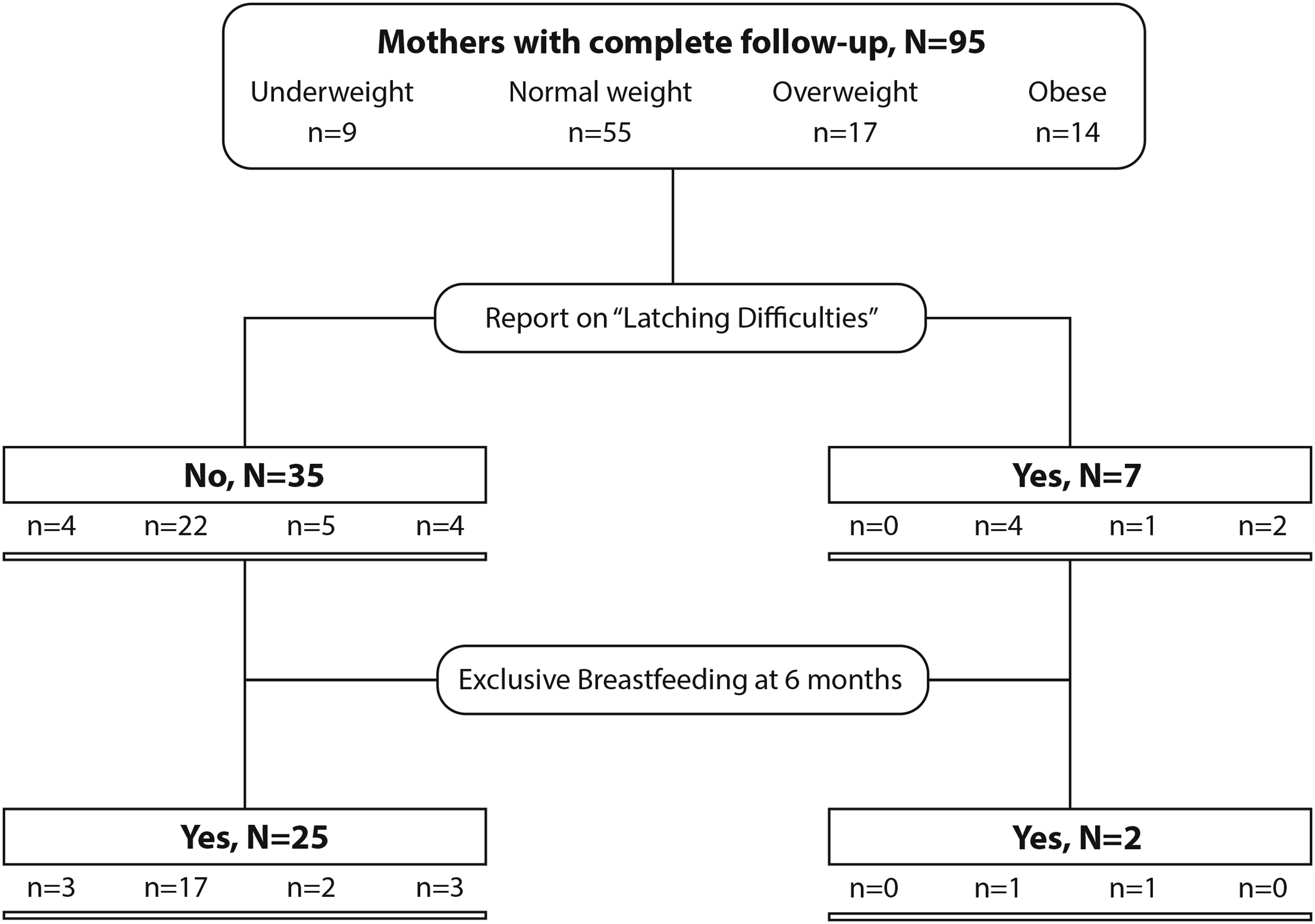
Reported latching difficulties and exclusive breastfeeding.
We performed backward stepwise logistic regression analysis wherein breastfeeding at 6 months of age was used as the dependent variable and eight predictors (maternal BMI, birth order, gestational age, infant BW, sore nipples at initiation of breastfeeding, nipple length, use of silicone nipples, and breast size). In this analysis, the variables that remained significant were prepregnancy BMI (odds ratio [OR] = 0.88, 95% confidence interval [CI]: 0.79–0.99, p = 0.03) (the higher the BMI, the lower the likelihood of breastfeeding at 6 months of age) and birth order (OR = 3.36, 95% CI: 1.44–7.83, p = 0.005) (the higher the birth order, the higher the likelihood of breastfeeding at 6 months of age). Nipple length was significant with a p-value of 0.047 in logistic regression, but not in binary logistic regression (OR = 0.86, 95% CI: 0.70–1.05) (the longer the nipple, the higher the likelihood of breastfeeding at 6 months of age).
Discussion
Several articles have described breastfeeding difficulties in obese mothers.3–5 When compared with nonobese mothers, obese mothers have lower breastfeeding initiation rates6,7 and shorter breastfeeding duration.7–9 . The reasons for these breastfeeding difficulties are probably multifactorial 13 as many factors have been suggested as possible culprits. For instance, the physiology of lactogenesis may be affected by maternal obesity 14 through insulin resistance 15 as well as through decreased prolactin response to infant suckling. 16
Obese mothers may also be at a higher risk for cesarean deliveries 17 which is a known risk factors for delayed breastfeeding initiation. 18 In addition, maternal anatomic factors have also been implicated in the success of breastfeeding. It has been reported that large breasts 10 and short nipples 11 may impair latch. Moreover, the presence of breastfeeding difficulties at the initiation of breastfeeding during the first few days of life has been found to be a strong predictor of breastfeeding failure and of short breastfeeding duration,1,2 which was also found in our study. Finally, Kair and Colaizy recently described that obese women had lower odds of breastfeeding because “babies were not satisfied by breast milk alone” or because of breastfeeding difficulties. 13
In this study, we examined duration of breastfeeding versus breastfeeding difficulties at initiation of breastfeeding in a convenience cohort of 109 women of various BMIs, in relation to specific issues related to the mothers' breasts. We found that the higher the BMI group, the larger the breast (p = 0.005), whereas the percentage of protruding nipples or that of flat nipples did not differ among groups. There were no significant differences among groups in nipple diameter or length, but the areola diameter was significantly smaller in the underweight group than in the three other BMI groups. The overall rate of initial latching difficulties was 15.5%, without statistically significant differences among all four BMI groups.
A limitation of our study was that since we carefully excluded type 2 and gestational diabetes, and since the prevalence of these two conditions is much higher in obese women than in other BMI groups, our findings may not be generalizable to obese women overall. However, the number of underweight women followed up was very small, and the study was not sufficiently powered to detect differences among the four groups. In addition, our findings cannot be generalized to other ethnic groups as all the mothers in our study were Caucasian. In stepwise regression analysis, the variables that influenced significantly the duration of breastfeeding up to six full months were prepregnancy BMI (the higher the BMI the lower the likelihood of breastfeeding at 6 months of age) and birth order (the higher the birth order the higher the likelihood of breastfeeding at 6 months of age). Nipple length was at the border of statistical significance.
We conclude that anatomic and anthropometric issues related to the breasts of obese women may affect breastfeeding initiation and breastfeeding continuation and duration. The breasts of obese women are in average larger, with a larger areola, longer nipple length, and higher nipple diameter. Nevertheless large breasts in obese women may contribute to breastfeeding difficulties. Short nipples may add their own independent effect, but this effect does not appear to be related and is not specific to maternal obesity. Since early latching difficulties appear to predict shorter breastfeeding duration, we suggest that such difficulties should trigger prompt intervention and early referral to lactation consultation.
Conclusions
The higher the maternal BMI, the larger the breast.
The higher the maternal BMI, the lower the likelihood of breastfeeding at 6 months of age.
The higher the birth order, the higher the likelihood of breastfeeding at 6 months of age.
Early latching difficulties appear to predict shorter breastfeeding duration.
Footnotes
Authors' Contributions
All authors have made an active contribution to the conception, design, analysis, and interpretation of the data and drafting of the article, and all have reviewed its content and have approved the final version submitted for publication.
The article has been read and approved by all authors and all authors agree to the submission of the article to the Journal.
Disclosure Statement
No competing financial interests exist.