
Abstract
Abstract
Background/Objective:
Performance of ocular examinations on children who were breastfed, fed with formula, and combination of the two for the first 6 months of age. Subsequently, refractive errors, allergic conjunctivitis, and retinal nerve fiber layer (RNFL) thickness were evaluated.
Materials and Methods:
The present study included a total of 242 eyes of 121 children (aged 60–84 months, 65 males, 56 females) admitted to the outpatient clinic of our institution. The patients were divided into three groups according to their feeding pattern during their first 6 months postdelivery: breastfed children (Group 1, n = 40), children fed with a combination of breast and formula milk (Group 2, n = 41), and children exclusively fed with formula-milk (Group 3, n = 40). All patients underwent detailed ophthalmologic examinations, and measurements of the RNFLs were recorded.
Results:
No significant difference was observed between the groups in terms of refractive error. In Group 3, we found that allergic conjunctivitis was significantly higher than in the other groups. In addition, in Group 3, the thickness of the RNFL was found to be significantly higher in the superior quadrants of both the eyes of children than in Groups 1 and 2 (p < 0.05).
Conclusions:
We found that the type of feeding experienced by infants in their first 6 months has no effect on refractive error but has significant effects on both allergic conjunctivitis and RNFL. To determine the cause of this difference in the RNFL and to further validate the present study, future studies with larger patient groups and animal experiments are needed.
Introduction
Although breast milk is considered to be more important for developing countries, it is very important for all babies regardless of their socioeconomic status. While the rate of breastfeeding in the first 6 months of life is 37% in developing countries, this rate is quite low in developed countries. 1 Especially in developed countries, formula foods are widely used instead of breast milk. However, the World Health Organization strongly recommends only breastfeeding during the first 6 months of life. 2
It is thought that breastfeeding is not only a simple source of nutrients but also that it supports the immunity of infants and that it contributes to brain maturation through the polyunsatured fatty acids, which it includes. Breast milk is considered to be an almost “miraculous” substance that provides positive emotional support to the baby separated from the uterus in the postnatal period and has many other benefits.3,4
In this context, the relationship between the intake of breast milk and many diseases has been examined. In particular, the role of breastfeeding in protection against obesity and malnutrition has been studied. Likewise, the positive relationship between breast milk and brain development, cognitive functions, and educational success is known.5,6 The relationship between ocular morbidity and breastfeeding is similarly of interest.
Although differing results have been obtained, studies on allergic conjunctivitis, refractive errors, visual acuity, and amblyopia have been performed.7–9
To our knowledge, this is the first study to examine the relationship between retinal nerve fiber layer (RNFL) measurement and breastfeeding and formula use. The aim of this study was to evaluate the relationship of breastfeeding and formula intake to ocular morbidity and RNFL measurements.
Materials and Methods
The study was planned as a prospective and cross-sectional study. Two hundred forty-two eyes of 121 children who were admitted to the Ophthalmology outpatient clinic of our hospital aged between 60 and 84 months were included in the study. The age, gender, sociodemographic features, and nutritional status of the patients were recorded.
The best corrected visual acuity was evaluated with (LogMAR) in all cases. Refraction conditions were measured with an auto kerato-refractometer (Topcon KR-1, Japan) and intraocular pressures were measured with a noncontact tonometer (Tomey FT-1000, Japan). Anterior segment examination was conducted with slit lamp biomicroscopy and detailed fundus examinations were performed with 90 D lens. Optical coherence tomography (Optovue OCT V 5.1, RTVue 100-2; Optovue, Fremont, CA, ABD) was performed to measure RNFL in both eyes of the patients. For the optic nerve, measurements of the four quadrants (upper, inferior, nasal, and temporal) were recorded. The patients were divided into three groups according to their feeding pattern during the first 6 months after delivery.
Patients fed only breast milk during the first 6 months were classified as Group 1 patients, fed both breast milk and formula Group 2, and Group 3 comprised patients fed only formula, without any breastfeeding. The parents of all patients included in the study were informed about the study and their written informed consent was obtained.
During the study, the ethical standards set out in the Declaration of Helsinki were complied with and approved by the local Ethics Committee. Approval was obtained from the local Ethics Committee of 2018/05 dated March 28, 2018.
Visual assessment: patients were measured with an auto refractometer without using cycloplegics. The best corrected visual acuity at a distance of 3 meters was assessed by the LogMAR scale (Keeler Ltd., Windsor, United Kingdom). Spherical and cylindrical values for both eyes, −1.00, and more negative values were recorded as myopia, +1.00, and higher values were recorded as hypermetropia.
Inclusion criteria
Sixty to 84 months, birth at full term with normal birth weight (2,500–4,000 g), height and weight within normal limits, no condition such as congenital glaucoma that could cause damage to the optic nerve, no corneal scarring that could prevent imaging, no nephelion, or lens disease.
Exclusion criteria
Height and body weight less than third percentile, obesity, prior ocular surgery, history of ocular trauma, systemic chronic disease, optic disc head abnormalities such as myelinated nerve fiber, and papillary edema.
In addition, mothers who used drugs for any reason were excluded from the study.
For statistical analysis, descriptive, chi-square test and ANOVA-bonferroni tests were applied using the SPSS 21 program.
Results
Of the 121 children included in the study, 53.7% (n = 65) were male and 46.3% (n = 56) were female. Group 1 consisted of 40 patients fed only breast milk in the first 6 months postpartum, Group 2 consisted of 41 patients fed breast milk with formula, and Group 3 consisted of 40 patients fed only formula. The spheric and astigmatic values of the patients according to autorefractometer measurements are considered to have a significant refractive error when they are bigger or smaller than ±1. A significant refractive error was found in 27.5% of Group 1, 36.5% of Group 2, and 32.5% of Group 3. A hyperopic shift was observed in Groups 1 and 2, whereas myopic values were more prominent in Group 3, but this difference was not statistically significant (Fig. 1 and Table 1).
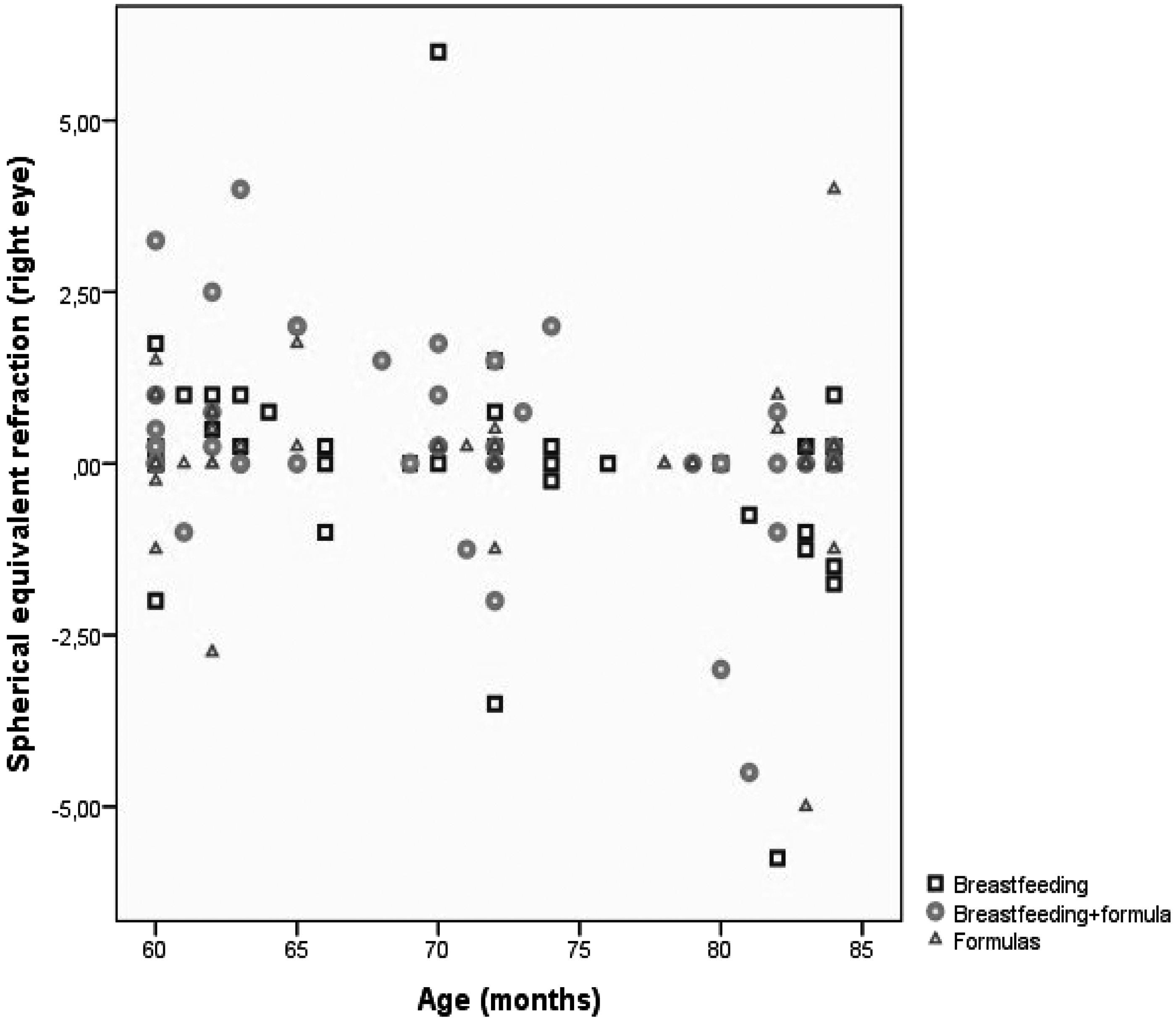
Right eyes spherical equivalent refraction.
Gender, Age, Allergic Conjunctivitis, and Refractive Disorder
Chi-square, one-way ANOVA.
p < 0.05.
In the biomicroscopic examination, patients with symptoms of conjunctival hyperemia and the presence of papillae under the eyelids were defined as having allergic conjunctivitis. The proportion of allergic conjunctivitis was 7.5% in Group 1, 9.7% in Group 2, and 32.5% in Group 3. The frequency of allergic conjunctivitis in patients using only formula was significantly higher than in the other two groups (Table 1).
RNFL thickness was analyzed in four quadrants, including superior, inferior, nasal, and temporal by analyzing the head of the optic nerve in both eyes of all patients. The parameters of the RNFL section ring, which is 3.45 mm away from the disc center, were automatically evaluated with the OCT device. In Group 3, we found that the superior, inferior, and nasal parts of the retina nerve fiber layer in the right eye and the superior and temporal parts in the left eye were statistically significantly higher than in Groups 1 and 2 (Fig. 2 and Table 2).
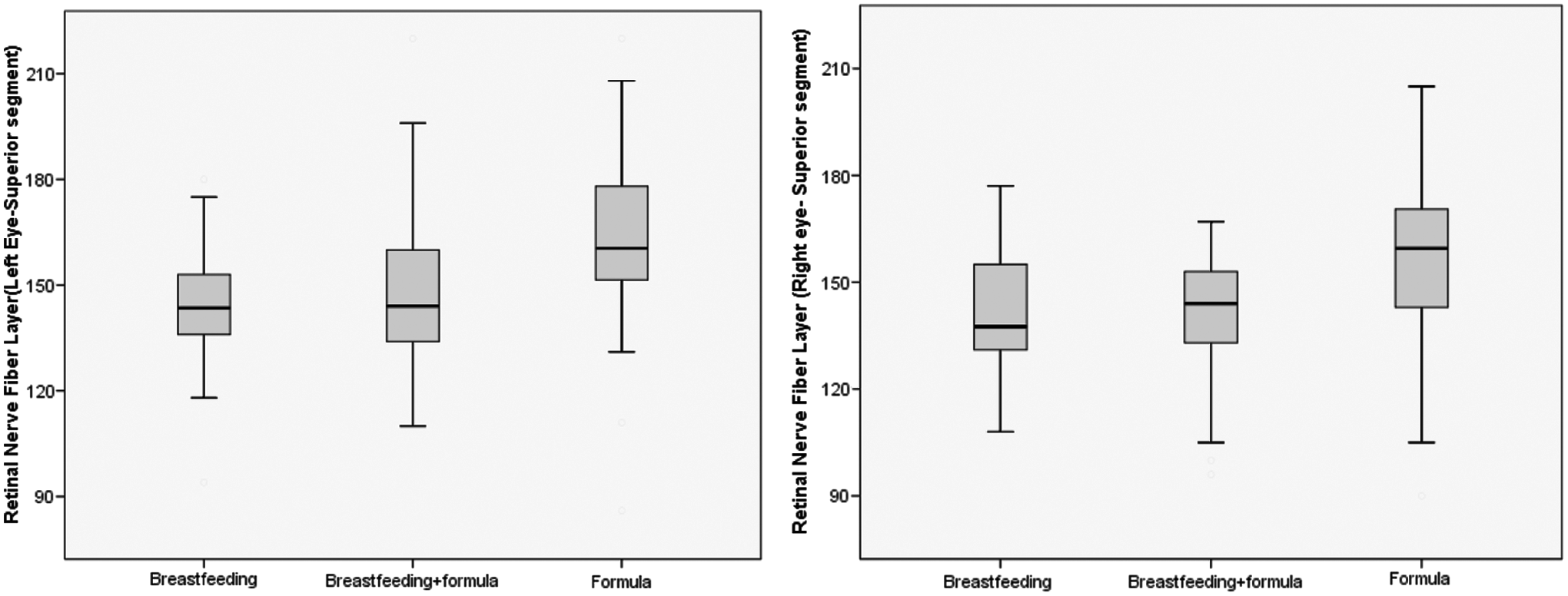
Retinal nerve fiber layer superior segment for right and left eyes by the groups.
Retinal Nerve Fiber Layer Thickness by Groups
One-way ANOVA.
p < 0.05.
The sociodemographic characteristics of the groups namely residence, education, economic income, and nutrition were evaluated. No statistically significant difference was found between the sociodemographic features of the mothers in relationship to the groups (Table 3).
Sociodemographic Feature of Patients
Chi-square.
Discussion
The effect of breast milk intake on diseases has been examined for many years. In particular, the polyunsatured fatty acids and antioxidants contained in breast milk have been directly related to the development of the retina and neural development.10,11 Since formula feeding is frequently used in developed countries, formulas which are close to breast milk have been developed. For example, docosahexaneoic acid (DHA), which was present in lower amounts in the formulas than in breast milk, has been added to formula foods in recent years. Although the fatty acids in the content of the mother's milk depend on the mother's diet, it is known to contain ∼8–30% linoleic acid, 0.5–2% a-linoleic acid, 0.5–0.8% arachidonic acid (ARA), and 0.1–0.4% DHA. 12
DHA is known as a long-chain polyunsatured fatty acid and is important for neuroretinal development. In fact, before scientists found that the retina was a continuation of the brain in a developmental and anatomical way, philosophers discussed this issue with the idea that the “eye is a window to the soul.” Over time, studies have shown that the optic nerve fibers formed by the ganglion cell axons of the retina are actually central nervous system axons. 13 Therefore, we expect to see similar effects of breast milk on the brain and on the retina.
In a study of children between 10 months and 4 years of age, Deoni et al. found that there was a positive relationship between the duration of breastfeeding and white matter development, and that the increase in white matter volume in late-mature areas, especially in the frontal and temporal regions was noteworthy. 14 In another study, the same group of researchers found that breastfeeding in children between 16 months and 2 years positively correlated with the increase in myelinization along with the development of white matter. They reported that the duration of breastfeeding affected the time of myelinization, that formula feeding reduced the growth of white matter, and that the volume of white matter was lower than in children fed with breastmilk. The volume of white matter in children fed with formula which contained DHA and ARA was close to that in children fed with breast milk; although it was lower than that in breastfed children.
In the light of these findings, Deoni et al. stated that helped the development of white matter in infants that were fed with formula. 15 In an experimental animal study on rhesesus monkeys, Liu et al. found that there was no difference in the size of the brain or the volume of gray and white matters in the groups that received breast milk and formula. 16 However, this finding has been contradicted in numerous studies on people.17,18
Using electroencephalography (EEG) and magnetic resonance imaging (MRI) in patients up to 1-year-old, Jing et al. reported that myelinization peaked at an early age in infants fed with formula (at 6 months) and at the ninth month in infants fed with breast milk. This study emphasized that differential trajectories and cognitive development in the brain may trigger different pathways in neurodevelopment. 19 In another study examining breast milk and brain development between 12 and 18 years of age, the parietal cortex was found to be thicker in the breast milk group, and it was found that it did not have any effect on vision and refractive disorder. 20
While there are many studies on the physiological effect of breast milk and the development of the brain, there has been no previous study in which the thickness of the RNFL in the orbit known as an extension of the brain has been evaluated. In this study, we investigated whether there was a relationship between the intake of breast milk and RNFL thickness. We found that the superior, inferior, and nasal parts of the right eye and the superior and temporal parts of the left eye of children fed only formula were significantly thicker in the right and left eyes compared with the other two groups. Although the retina appears to be the continuation of the embryogenetic and anatomical brain, this finding shows that nutrition may have different effects on the retina and brain.
Neurotrophic substances are known to be present in breast milk. In recent years, formula foods that are close to breast milk in content have been developed. 21 Synthetic supplements such as DHA and ARA, which are now present at a high level in formulas and which are important in the development of white matter, can also increase RNFL. Therefore, a marked thinning of RNFL is not expected in children with a formula-fed diet. In our study, we found that the RNFL was thicker in the formula-fed infants, although we were expecting it to be thicker in the breastfed children.
Despite this result, thickness of the RNFL does not always mean neurotrophy. RNFL thickness may be increased by certain pathological events. For example, amiodarone induced lipidosis by inhibiting the axoplasmic flow in retinal toxicity causes an increase in RNFL thickness. 22 Thiamin deficiency also increases RNFL thickness in the acute period. 23 Moreover, it is not known whether this increase in thickness is a healthy increase or an adaptive change in the RNFL. How children whose RNFL is thicker will respond at a later age to neurodegenerative diseases with increased intraocular pressure, such as glaucoma, and the degree of resistance to atrophy remain to be determined. In the light of this, it is not clear whether the RNFL increase in children fed with formula is a healthy neurotrophy or an abnormal hypertrophy. More extensive studies with more patients are needed to clarify this situation.
Our next study, using electroretinography (ERG) will be to investigate ganglion cell functions and histopathological changes such as hypertrophy and hyperplasia in the optic nerves of rats fed with formula and breast milk. We believe that this work will provide an important impetus for new research.
The relationship between refraction defects and breastfeeding intake has been investigated in several studies and differing results have been obtained. In 2018, Liu et al. reported that spherical equivalent refraction (SER) is more hyperopic in breastfed children, that there is a correlation between reduced myopic risk and breastfeeding, but that there is no correlation between axial length and breast milk. 24 In another study Sham et al. emphasized that breastfeeding is associated with hyperopic SER. 25 Shirzadeh et al. did not find any relationship between feeding pattern during the first 6 months of life and refractive errors or the level of vision. 26 In this study, we observed that diet did not make a significant difference in SER, but the tendency to myopia was observed in the formula-fed children as in Shirzadeh et al.'s study.
A number of studies have been conducted in recent years on whether there is a link between allergic diseases and the duration of breastfeeding. Among these studies, there are studies which suggest that breast milk is not associated with allergic diseases as well as studies which suggest that it prvides a defense against allergic diseases. Huang et al. found that children who had been breastfed for 3–6 months had a lower risk of asthma and wheezing, and that the risk of fever, rhinitis, pneumonia, and eczema was significantly lower in children who had breastfed for more than 6 months. 27 On the contrary, Bion et al. argued that the duration and intensity of breastfeeding was not associated in the long term with allergic diseases such as asthma, eczema, rhinitis, and atopy. 28
In our study, we found that the frequency of allergic conjunctivitis in children fed only formula was significantly higher than the other two groups. Although the frequency of allergic conjunctivitis in children feeding both of breast milk and formula was found to be more than feeding only breast milk, there was no significiant difference.
Conclusions
As a result of this study, we found that breast milk protects against allergic conjunctivitis.
Even though there was a hyperopic shift in the group fed with breast milk, there was no significant effect on SER in our study. In addition, the significantly higher level of RNFL thickness in the superior quadrants, especially in the formula-fed children should be further investigated in studies to be performed with large patient groups and animal experiments are needed to explain the pathophysiology.
Footnotes
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure Statement
Conflicts of interest: None.