
Abstract
Abstract
Background:
Breastfeeding rates among low-income children participating in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) lag behind national rates. In Los Angeles County (LAC), recent efforts have been made to increase the number of Baby-Friendly designated hospitals. This study examines changes in Baby-Friendly hospital practices, breastfeeding outcomes, and their relationships with Baby-Friendly hospital status among WIC-enrolled children in LAC.
Methods:
Cross-sectional data from the triennial LAC WIC Survey (2008 through 2017) were analyzed (n = 6,449) to examine changes in Baby-Friendly hospital practices over time, and differences in breastfeeding outcomes by specific Baby-Friendly hospital practices. Multivariate logistic regression was used to evaluate the relationship between the number of Baby-Friendly hospital practices that mothers met and any and exclusive breastfeeding outcomes.
Results:
In 2017, mothers surveyed were more likely to engage in Baby-Friendly hospital practices compared with 2008. Any and exclusive breastfeeding outcomes at 1 and 3 months significantly increased since 2014, and breastfed infants were more likely to have mothers who participated in Baby-Friendly hospital practices. The more Baby-Friendly hospital practices mothers met, the better the breastfeeding outcomes. However, there is room for improvement in the uptake of Baby-Friendly hospital practices in Baby-Friendly hospitals.
Conclusion:
Effort is needed to ensure Baby-Friendly hospitals have support to continuously comply with all steps to maintain Baby-Friendly designation, and non-Baby-Friendly hospitals have support to incorporate these practices into hospital protocols.
Introduction
Breastfeeding provides advantages for infants, mothers, and families through nutritional, immunologic, social, and economic benefits. 1 Many health organizations, including the World Health Organization (WHO), recommend exclusively breastfeeding newborns for the first 6 months of life.1–3 Though breastfeeding continuation rates and exclusive breastfeeding rates have steadily increased in the United States since 2002–2003, overall rates remain low. 4 Among infants born in 2015, only 24.9% were exclusively breastfed through 6 months. 5
According to the Surgeon General, barriers to breastfeeding in the United States include lack of knowledge, social support, or access to childcare, lactation problems, as well as barriers related to health services, such as hospital practices and policies in maternity settings. 6 In 1991, the WHO and the United Nations Children's Fund (UNICEF) launched the Baby-Friendly Hospital Initiative (BFHI) to promote breastfeeding and safe feeding. 7 For hospitals to become designated as Baby-Friendly, they must demonstrate successful implementation of the Ten Steps to Successful Breastfeeding—evidence-based standards of care such as having a written breastfeeding policy, training staff to implement the policy, and helping mothers initiate breastfeeding within 1 hour of birth.8,9 Owing to the Ten Steps, evidence suggests that infants born at Baby-Friendly hospitals benefit from increased breastfeeding initiation and duration.10–12
As is the case with many health outcomes and behaviors, low-income children are disproportionately affected by low rates of breastfeeding. The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), a federally funded nutrition program for low-income pregnant, breastfeeding, and postpartum women, infants, and children under 5 who are at risk for poor nutrition, provides breastfeeding support, nutrition education, and food assistance. 13 Despite this support, WIC participants experience lower rates of breastfeeding—among children born in 2015, 44.5% of WIC children were breastfed at 6 months compared with more than 70% of children nationally. 4 Though breastfeeding uptake is lower in this population, only a handful of studies have examined the effect of Baby-Friendly hospital practices among low-income children.11,12
In Los Angeles County (LAC), where about two-thirds of all infants are currently served by WIC, 14 the number of Baby-Friendly hospitals is quickly expanding. Among 57 birthing hospitals, four achieved Baby-Friendly designation by 2010, 13 by 2012, 18 by 2014, and as of December 2018, there were 38 Baby-Friendly hospitals.15,16 Studies show that implementation of Baby-Friendly hospital practices is associated with increased rates of breastfeeding duration.17,18 A review found a dose–response relationship between the number of Baby-Friendly steps that mothers were exposed to and the likelihood of improved breastfeeding outcomes. 11 Among the WIC population in LAC, Nobari et al. found increasing rates of uptake in Baby-Friendly hospital practices between 2008 and 2014. 19 However, the proportion of Baby-Friendly hospitals in LAC has more than doubled since 2014 from about 30% to 67% in 2018. Our study, therefore, attempts to re-evaluate changes in Baby-Friendly hospital practices since 2014 among the WIC population in LAC. We also evaluate changes in breastfeeding outcomes, and the relationship between both hospital practices and breastfeeding outcomes with Baby-Friendly hospital status.
Materials and Methods
Data sources
The LAC WIC Survey is a triennial cross-sectional survey conducted in English or Spanish through a computer-assisted telephone interviewing system that randomly samples about 5,000–6,000 WIC families living in LAC. 14 Families are eligible to participate if the mother was pregnant and enrolled in WIC, or had a child younger than 5 years enrolled in WIC. Survey respondents are asked questions about one child from each family in addition to questions about the family's sociodemographic characteristics, child's birthing hospital, and mother's breastfeeding practices. Data for this study came from the 2008, 2011, 2014, and 2017 surveys. The complete survey methodology has been published elsewhere. 20 Survey responses were used to examine changes in Baby-Friendly hospital births and breastfeeding outcomes between 2014 and 2017, changes in Baby-Friendly hospital practices between 2008 and 2017, differences in Baby-Friendly hospital practices by Baby-Friendly hospital status in 2017, differences in breastfeeding outcomes by Baby-Friendly hospital practices in 2017, and the relationship between the number of Baby-Friendly hospital practices met and breastfeeding outcomes in 2017.
Sample
The study was restricted to infants born in LAC hospitals, no older than 2 years of age at the time of the survey, and whose biological mothers were interviewed, resulting in a final sample size of 6,449 (1,451 for 2008, 1,723 for 2011, 1,699 for 2014, and 1,576 for 2017) that was used to examine changes in three Baby-Friendly hospital practices. To examine the association between the number of Baby-Friendly hospital practices met and breastfeeding outcomes in 2017, the sample was further restricted to respondents without missing information on any potential confounders (n = 1,544).
Study variables
A child was considered to receive any breastfeeding if the mother had ever breastfed the child. Any breastfeeding duration (at 1, 3, and 6 months) was calculated by using the child's age at which the mother stopped breastfeeding her child. Exclusive breastfeeding was defined as the child consuming only human milk without any supplemental food or drink. Exclusive breastfeeding duration (at 1, 3, and 6 months) was determined by the age at which the child was given anything besides human milk.
In all four survey years, mothers were asked about three hospital practices related to the Ten Steps to Successful Breastfeeding—whether the child was “fed only [human milk] at the hospital” (Step 6), “the hospital staff gave … formula to take home” (Step 6), and “the hospital [gave] a telephone number to call for help with breastfeeding” (Step 10). According to the Ten Steps, mothers should feed their infants only breast milk at the birthing hospital unless there are medical justifications for formula use; hospital staff should not give mothers formula to take home; and hospitals should refer mothers to breastfeeding support groups on discharge (such as providing a phone number to a breastfeeding helpline). Mothers’ binary responses to these three Baby-Friendly hospital practices were used to evaluate changes by survey year, and test whether breastfeeding outcomes differed by these three practices. For the multivariate logistic regression analyses, the main independent variable was the number of Baby-Friendly hospital practices successfully met by mothers, calculated for each mother by adding up her responses to the three questions about Baby-Friendly hospital practices. For any breastfeeding outcomes, the number of Baby-Friendly hospital practices successfully met ranged from 0 to 3 (0 = did not meet any of the three Baby-Friendly hospital practices evaluated and 3 = met all three). Mothers who were not given a formula pack to take home were considered to have met the Baby-Friendly hospital practice. Since exclusive breastfeeding meant the child only consumed human milk, for exclusive breastfeeding outcomes, we did not include “fed her child only human milk at hospital” into the calculation. Therefore, for exclusive breastfeeding outcomes, the number of Baby-Friendly hospital practices successfully met by mothers ranged from 0 to 2.
Baby-Friendly designation status of LAC hospitals where WIC infants were born and the date of designation, if applicable, were obtained from the BreastfeedLA website. 16 Infants born in a hospital at or after the time of Baby-Friendly designation were considered to have been born in a Baby-Friendly designated hospital. Infants born in a hospital that became Baby-Friendly since the infant's birth were considered to have been born in a Baby-Friendly in-process hospital. Hospitals that did not receive designation as of December 2018 were considered non-Baby-Friendly.
Sociodemographic characteristics used in regression analyses included the child's gender and age, along with the mother's age, education, and Hispanic ethnicity. Other variables included were the child's preterm birth status (≤36 weeks of pregnancy), the mother's breastfeeding intent, and whether the father lived in the household, since these can influence breastfeeding.6,20,21
Data analysis
Chi-square tests were used for the first four sets of analyses: (1) changes in the percent of births in Baby-Friendly hospitals and in breastfeeding outcomes between 2014 and 2017; (2) changes in three Baby-Friendly hospital practices between 2008 and 2017; (3) differences in three Baby-Friendly hospital practices by Baby-Friendly hospital status in 2017; and (4) differences in breastfeeding outcomes by three Baby-Friendly hospital practices in 2017. Using survey data from 2017, multivariate logistic regression was used to examine associations between the number of Baby-Friendly hospital practices that mothers received and each breastfeeding outcome, adjusting for possible confounders. Since breastfeeding outcomes were examined at various ages (1, 3, and 6 months), infants had to be at least the age of interest to be included in the subsample. All analyses were conducted using R version 3.5.1. 22
Results
At the time of the 2017 survey, children's mean (standard deviation) age was 14.2 (6.4) months and 50% were female. About three-quarters of children had mothers who were Hispanic (74%), 67% had mothers with at least a high school education, and 68% lived with both parents.
Birthing hospitals and breastfeeding outcomes: 2014–2017
Table 1 shows that the percentage of WIC infants born in Baby-Friendly hospitals (designated or in-process) significantly increased from 63.6% in 2014 to 75.4% in 2017. Between 2014 and 2017, the percentage of infants who received any breastfeeding at 1 month significantly increased from 84% to 93.8%. The percentage of infants exclusively breastfed at 1 month also significantly increased from 30.9% in 2014 to 41.5% in 2017. Though it is recommended that infants be exclusively breastfed for the first 6 months of life, only 8.2% and 9.3% of children in the sample met this recommendation in 2014 and 2017, respectively.
Prevalence of Births in Baby-Friendly Hospitals and Breastfeeding Outcomes Among WIC-Participating Children ≤2 Years in Los Angeles County Between 2014 and 2017
Chi-square test of differences: *p < 0.05; **p < 0.01; ***p < 0.001.
In-process hospitals are those that obtained Baby-Friendly designation after the child's birth.
Baby-Friendly hospital practices: 2008–2017
The percentage of mothers who reported participating in Baby-Friendly hospital practices continued to increase between 2008 and 2017 (Fig. 1). The percentage of infants exclusively fed human milk at the hospital almost doubled from 31.2% in 2008 to 59.3% in 2017. Hospitals in LAC significantly cut down the practice of giving mothers formula to take home, becoming more compliant with Baby-Friendly hospital practices. In 2008, only 13.9% of mothers were not given a formula pack to take home compared with 54.7% in 2017. Between 2008 and 2017, the majority of mothers surveyed consistently reported that they were given a phone number to a breastfeeding helpline.
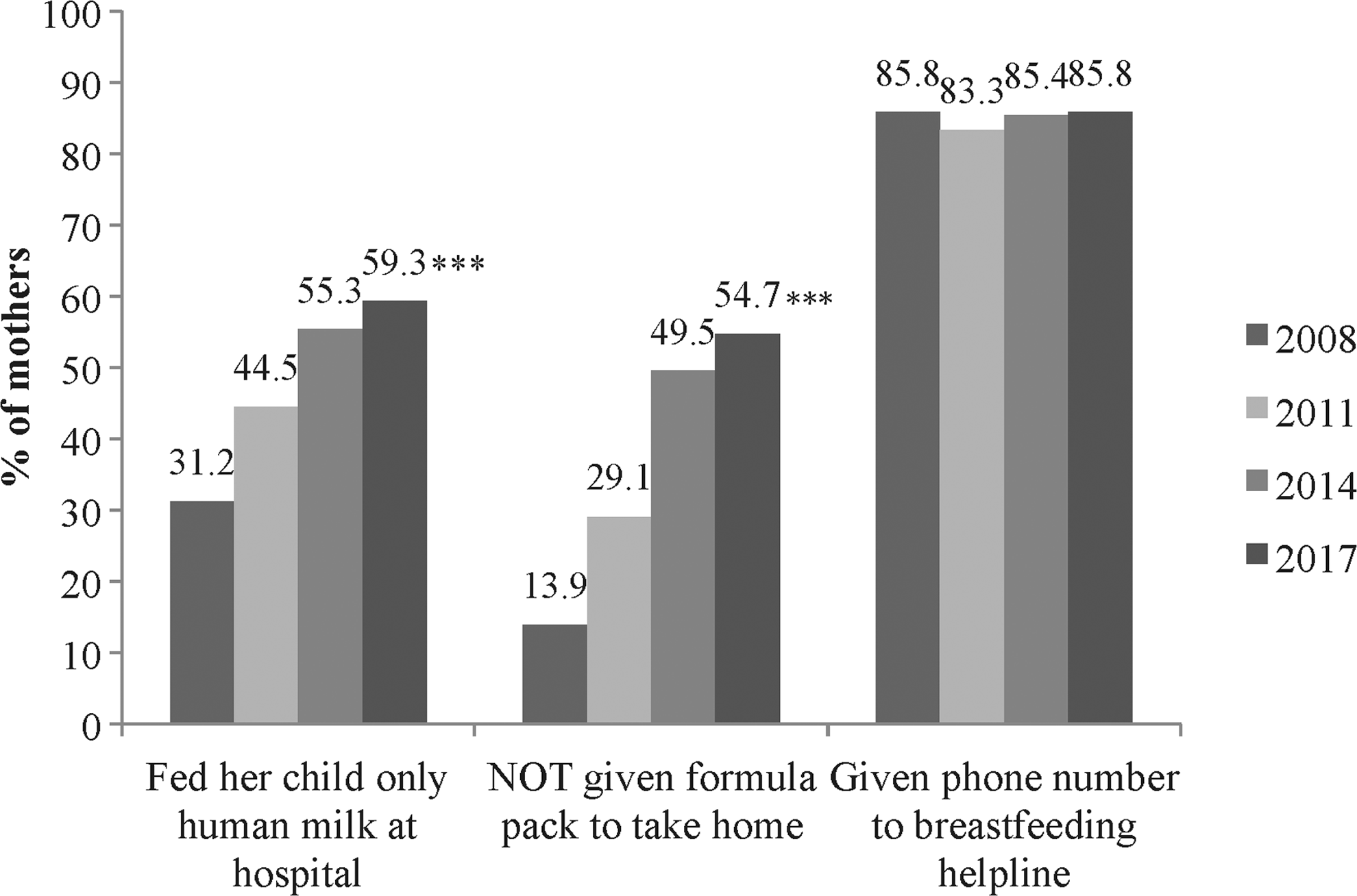
Baby-Friendly hospital practices reported by mothers of WIC-participating children ≤2 years in Los Angeles County who gave birth at any hospital in Los Angeles County: 2008–2017. Chi-square test of differences: ***p < 0.001. WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Baby-Friendly hospital practices and Baby-Friendly hospital status in 2017
Hospitals need to demonstrate successful implementation of the Ten Steps to become designated as Baby-Friendly. Figure 2 shows that two of three hospital practices related to the Ten Steps were significantly met by more mothers who gave birth in in-process or designated Baby-Friendly hospitals than mothers who gave birth in non-Baby-Friendly designated hospitals. The percentage of infants fed only human milk at the hospital was 6–8% lower in non-Baby-Friendly hospitals compared with infants born in Baby-Friendly in-process or designated hospitals. In compliance with the Ten Steps, the distribution of formula gift packs was significantly less prevalent in Baby-Friendly in-process or designated hospitals than in non-Baby-Friendly hospitals (about 60% did not receive formula packs on discharge versus 40%). The vast majority of mothers reported receiving a phone number to a breastfeeding helpline at the hospital where she gave birth, regardless of the hospital's Baby-Friendly status.
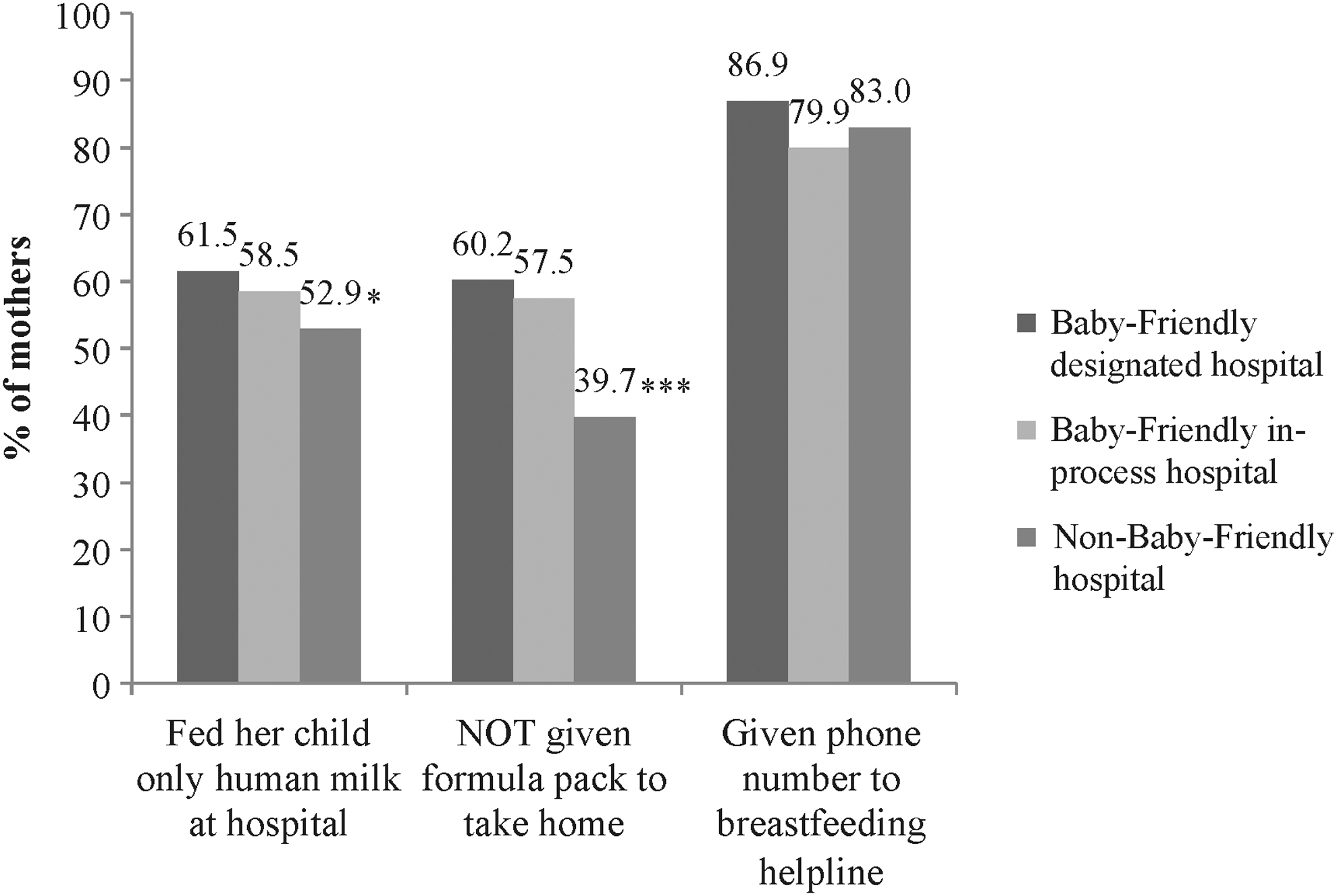
Baby-Friendly hospital practices reported by mothers of WIC-participating children ≤2 years in Los Angeles County by hospital's Baby-Friendly status: 2017. Chi-square test of differences: *p < 0.05; ***p < 0.001.
Breastfeeding outcomes and Baby-Friendly hospital practices in 2017
There were significant differences in the proportion of mothers meeting various breastfeeding outcomes by compliance with Baby-Friendly hospital practices (Table 2). The proportion of mothers who breastfed at 6 months and exclusively breastfed at 1, 3, and 6 months was significantly higher for mothers who exclusively breastfed their infants at the birthing hospital compared with mothers who did not. Mothers who were not given formula to take home were significantly likelier to breastfeed at 1 month and exclusively breastfeed at 1, 3, and 6 months compared with mothers who were given formula on discharge. Finally, the proportion of mothers who breastfed at 1, 3, and 6 months and exclusively breastfed at 1 and 3 months was significantly higher for mothers who received a phone number for breastfeeding helplines compared with mothers who did not.
Proportion of Mothers Meeting Various Breastfeeding Outcomes by Compliance with Baby-Friendly Hospital Practices As Reported by Mothers of WIC-Participating Children ≤2 Years in Los Angeles County: 2017
Chi-square test of differences for each breastfeeding outcome: *p < 0.05; **p < 0.01; ***p < 0.001.
Exclusive breastfeeding was defined as the child consuming only human milk without any supplemental food or drink, including only being fed human milk in the hospital.
All children in this subsample were breastfed at 1 month.
WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Number of Baby-Friendly hospital practices successfully met by mothers and breastfeeding outcomes
To examine the impact of Baby-Friendly hospital practices on breastfeeding duration, we ran multivariate logistic regressions, controlling for factors known to be associated with breastfeeding duration. Table 3 shows that for any and exclusive breastfeeding outcomes, the odds of an infant being breastfed were significantly higher when the infant's mother received at least two Baby-Friendly hospital practices that we evaluated. The mother's intention to breastfeed was another strong, significant predictor of any breastfeeding duration and exclusive breastfeeding at 1 month. Having a father living in the household was significantly associated with any and exclusive breastfeeding at 1 month. Children born preterm were significantly less likely to receive any breastfeeding at 1 month, and less likely to be exclusively breastfed at 1 and 3 months compared with children who were not born preterm.
Logistic Regression Models of Breastfeeding Outcomes Among WIC Participating Children ≤2 Years: 2017
Data are given as odds ratio [95% confidence interval]. Statistically significant odds ratios are in bold.
Two or more practices for “any breastfeeding” outcomes/two practices for “exclusive breastfeeding” outcomes.
ref, reference; HS, high school.
Discussion
Consistent with the increase in the number of Baby-Friendly hospitals in LAC, about three-quarters of WIC children born in LAC were born in a Baby-Friendly hospital based on the 2017 survey. Baby-Friendly hospital practices in the county have also dramatically increased since 2008. The increased number of Baby-Friendly hospitals’ uptake of Baby-Friendly hospital practices coincides with significant increases in any and exclusive breastfeeding outcomes among WIC infants in LAC.
Previous research suggests that mothers of low socioeconomic status may be more likely to experience barriers to duration of breastfeeding, such as insufficient social support and role modeling, and issues with lactation.6,23 These barriers may be addressed by the Ten Steps implemented in Baby-Friendly hospitals. Steps such as helping mothers breastfeed in the first hour, exclusive breastfeeding in the hospital, and putting mothers in touch with support groups have been found to increase breastfeeding duration.11,24 In our study, an infant had significantly better breastfeeding outcomes when the infant's mother successfully met any of the three Baby-Friendly hospital practices we evaluated. We also found that the more Baby-Friendly hospital practices mothers met, the better the infant's breastfeeding outcomes. Our findings are consistent with studies that show that the number of Baby-Friendly hospital practices experienced by mothers has a positive effect on short-term breastfeeding.24–26
Of the Ten Steps, several studies reported that lack of adherence to Step 6 (exclusive breastfeeding during hospital stay), in particular, is a major risk factor for poor breastfeeding outcomes, serving as an indicator of how well the other steps are executed.11,27–29 Our study found that WIC infants born in LAC Baby-Friendly hospitals were significantly more likely to have been exclusively breastfed at the hospital, and less likely to have been given formula when leaving compared with children born in non-Baby-Friendly hospitals—the two Baby-Friendly hospital practices related to Step 6 that we evaluated. Regardless of Baby-Friendly designation, we also found that children receiving any breastfeeding at 6 months and exclusive breastfeeding at 1, 3, and 6 months were significantly more likely to have been fed only human milk at the birthing hospital, further demonstrating Step 6 as an important predictor of breastfeeding outcomes.
In our sample, the majority of mothers who gave birth in Baby-Friendly hospitals reported complying with Baby-Friendly hospital practices. Though the practices are better implemented in Baby-Friendly than in non-Baby-Friendly hospitals, compliance with Baby-Friendly hospital practices can be improved. Merewood et al. found that hospitals find Step 6 (exclusive breastfeeding during hospital stay), Step 2 (train health care staff to implement written breastfeeding policy), and Step 7 (allow mothers and infants to remain together 24 hours a day) the most difficult to meet. 30 The suboptimal uptake of the hospital practices we evaluated may be due to barriers faced by both hospital staff and new mothers. For example, barriers to staff support of Baby-Friendly hospital practices include fear of infants becoming dehydrated or hypoglycemic and lack of time to educate and support breastfeeding mothers. 31 Mothers may lack interest in breastfeeding at the hospital due to fears that they are not providing “enough milk,” sore nipples, their desire to feed both breast and bottle due to plans to return to work, along with concerns that if they do not begin a bottle right away, the baby will not take the bottle later. 31 Knowledge, education, and good training are paramount. Addressing barriers early on, forming a dedicated multidisciplinary team, obtaining administrative support, and investing time have been identified as key components to the success of BFHI. 31
In our study, the majority of mothers (60%) reported receiving formula gift packs in non-Baby-Friendly hospitals. Though Baby-Friendly hospitals should not be sending any formula packs home with mothers, about 40% of mothers who delivered at a Baby-Friendly hospital reported receiving one. It is possible that mothers may have reported that they received a formula pack when, in reality, they were given a gift bag (without formula). However, we found it encouraging that a large proportion of mothers who gave birth in non-Baby-Friendly hospitals still reported complying with the other Baby-Friendly hospital practices we evaluated. More than half of all mothers who gave birth in non-Baby-Friendly hospitals fed their infants only breast milk in the hospital. Breastfeeding support phone numbers are also shared with a large majority of women, regardless of Baby-Friendly hospital status. Further research is needed to determine how Baby-Friendly hospital practices can be incorporated into hospital protocols in non-Baby-Friendly hospitals.
A strength of our study is the examination of any and exclusive breastfeeding over three different periods. Few studies in the United States have examined exclusive breastfeeding beyond a month. 10 We also used information from BreastfeedLA to determine hospitals’ Baby-Friendly designation status. Since a mother's report of exposure to Baby-Friendly hospital practices may be susceptible to both poor recall and recall bias, 24 we restricted our sample to children younger than 2 years. Though other studies often consider participation in WIC as a confounder,24,32 our sample consisted of only WIC-participating children, which we view as a strength. However, it is possible that survey respondents were more likely to be women who breastfed or gave birth in a Baby-Friendly hospital, which could affect the representativeness of our sample. Another limitation is our evaluation of only three Baby-Friendly hospital practices related to Steps 6 and 10—studies show that the greater number of steps met can influence breastfeeding duration.24,27 Our study did not look at justification for formula use, which could have caused some misclassification since newborns with acceptable medical reasons for receiving breast milk substitutes are considered to be adherent to Step 6. 33 Step 10 states that mothers should be referred to breastfeeding support groups on discharge, which we measured as hospital provision of a phone number to a breastfeeding helpline. However, these referrals can be provided through other means such as websites, printed material, or linkages to lactation support groups. Our study would, therefore, likely underestimate adherence to Steps 6 and 10. Finally, since WIC participants receive breastfeeding education and support, and may receive supplemental infant formula, these findings may not be generalizable to low-income populations not served by WIC.
Conclusion
In our study, three-quarters of WIC children were born in Baby-Friendly hospitals in LAC. Since 2008, mothers, regardless of their birthing hospital's Baby-Friendly designation, are significantly more likely to engage in Baby-Friendly hospital practices. The increase in both Baby-Friendly hospitals and engagement of Baby-Friendly hospital practices coincides with significant increases in any and exclusive breastfeeding outcomes at 1 and 3 months since 2014. Breastfed infants were more likely to have mothers who participated in Baby-Friendly hospital practices, and the more Baby-Friendly hospital practices mothers met, the better the infant's breastfeeding outcomes. However, the uptake of Baby-Friendly hospital practices in Baby-Friendly hospitals could be improved. Since our findings suggest that Baby-Friendly hospital practices beneficially influence breastfeeding outcomes, continued effort is needed to ensure that Baby-Friendly hospitals have support to continuously comply with all Ten Steps to maintain their Baby-Friendly designation. In non-Baby-Friendly hospitals, Baby-Friendly hospital practices are already being practiced, though at lower rates. Support for hospitals not currently on the path to Baby-Friendly status may be able to use results such as these to support the uptake of these practices, and work toward achieving Baby-Friendly designation.
Footnotes
Acknowledgments
The authors gratefully acknowledge Catherine Martinez for her contributions to this work. They would also like to thank Daniel Yoo for all of his valuable feedback and the WIC participants for their willingness to complete the survey. Analysis of WIC data has been supported since 2002 through a Research Partnership with First 5 LA, a child advocacy and grant-making organization created by California voters to invest Proposition 10 tobacco taxes to improve the lives of children from prenatal to age 5 in Los Angeles County. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.
Disclosure Statement
No competing financial interests exist.