
Abstract
Background:
Expressing human milk using commercially available pumps has increased. Most women use mechanical means to transfer their milk at some point during lactation. Yet, there is very little quantification of any breast tissue changes that occur when using mechanical devices to facilitate milk transfer.
Objective:
Women comfortable with breastfeeding were recruited to participate in a study to measure physical changes of the breast with a variety of human milk transfer modalities under close observation.
Materials and Methods:
Direct breastfeeding with their infant, hand expression, and mechanical milk transfer using two commonly available breast pumps were utilized over four milk transfer sessions with each participant. Each participant directly breastfed on the first milk transfer session and the remaining modalities were randomized. Measurements were taken before and after each modality using digital calipers. Participants completed a modified pain scale after each observation. Measurements taken after breastfeeding were used as the control for data interpretation for each participant. After a 20-minute rest period, breast tissue was again examined, and tissue appearance was recorded. Within-subject modality differences were calculated, and paired analysis mean difference and standard error of the mean are presented.
Results:
Fifty eligible women were approached with 92% participating. The “before” measurements were not significant for all the modalities. The “after” measurements were significantly different at p < 0.003 for breast pumps but not for breastfeeding or hand expressing. Many participants indicated pain with pumping.
Conclusion:
Mechanical pump use correlated with significantly increased length and diameter of the nipple compared with the post-breastfeeding and hand expressing dimensions. Pump use correlated with significant pain scores and resulted in localized inflammatory changes. Understanding how pumps affect breast tissue is helpful in improving experiences with breast pumps and may improve breastfeeding outcomes. Additional research is needed to better understand ramifications of long-term use of breast pumps.
Introduction
The use of mechanical devices for human milk transfer is increasingly common, yet clear guidelines are lacking for when and why to begin pumping. 1 Data from studies in the Unites States suggest that at least once during lactation between 68% and 92% of lactating women use hand or mechanical methods of expressing their milk from the breast.2–6 One study reported that 80% of women mechanically express their breast during the first 4 months postpartum. 7 Another study reported that 40% of the participants were expressing their breasts several times each day, 8 while one in five women noted adverse effects from using a breast pump. 9 Similarly, a survey of postpartum women using pumps reported pumping was unpleasant compared with breastfeeding. 10
From these and other surveys, the most commonly reported adverse events by women associated with using a breast pump have been pain, soreness, and the need for medical intervention. 11 However, objective data on the impact to local mammary tissue via breast pump devices are lacking. 12 While a variety of pumps have been studied for effects of vacuum level and cycle differences on milk transfer, there is a distinct lack of data examining the physical effects of these devices, particularly the impact such devices have on the nipple and areolar tissue. Filling this gap in knowledge could provide improved understanding of mechanical milk transfer.
To gain knowledge about any physical changes to breast tissue with milk transfer, breast tissue of women using various milk transfer modalities was observed, measured, and clinically assessed before and after each transfer session. The purpose of this study was to document and compare any breast tissue changes after the milk transfer modalities of breastfeeding, hand expressing, and the use of two common breast pumps. The meaning of the term “breastfeeding” in this study refers to the infant transferring milk directly “at-the-breast.” 13
The questions addressed were as follows: (1) Are there measurable differences in nipple diameter and length between different milk transfer modalities? (2) Based on milk transfer modality, are there corresponding visible changes to the nipple, areola, or the breast tissue under standard clinical examination? (3) Does maternal pain relate to any physiologic changes?
Materials and Methods
Design and participants
The study protocol was a randomized crossover design approved by the local hospital institutional review board. The participants were recruited through a private practice lactation center located in the western United States via researcher face-to-face interaction, flyers, and social media announcements. Participants were recruited as a convenience sample based on the availability of the participants who met the inclusion criteria.
Inclusion criteria for participants were as follows: (1) breastfeeding women ≥18 years of age, (2) have no history of breast tissue damage, including whether surgical or traumatic in source, (3) able to speak, read, and write in English, (4) be breastfeeding an infant between 2 and 3 months of age, growing well, and at appropriate weight for age based on standard pediatric growth chart recommendations, and (5) had some experience but had not regularly used a breast pump. Potential participants were provided with a consent form for their review. Upon agreement to participate, the informed consent form was reviewed with and signed in the presence of the research study coordinator.
The first observation was breastfeeding (BF), with the order of the remaining modalities randomized. The hand expression (HE) and two pumps were used in a random order based on a computer randomization program. The order of the modalities was as follows: Participant 1 ([BF], Pump In Style® [P2], HE, Purely Yours® [P1]), Participant 2 (BF, HE, P2, P1), Participant 3 (BF, P1, HE, P2), Participant 4 (BF, P2, P1, HE), and so on, based on the randomization table that was computer generated.
Data collection took place in a private examination room at the lactation center to ensure each participant's privacy. The observations were scheduled 1 to 3 days apart (as the participants' schedule dictated) and occurred between 7 a.m. and 11 a.m., within 2 hours of the previous observation time and within 2 to 3 hours after the last breastfeeding. At the beginning and end of each milk transfer session, each participant had nipple length and diameter measured using digital analytic calipers. The measurements collected from BF sessions were used as the baseline values to compare all other values.
Instruments
The four modalities of milk transfer used in the study were as follows: direct BF; HE (using the Jane Morton method) 14 ; P1, a Purely Yours® pump made by Ameda (vacuum range from 75 to 200 mm Hg and cycle range from 30 to 60 cycles/minute); and P2, Pump In Style® made by Medela (vacuum range from 100 to 250 mm Hg and cycle range from 54 to 78 cycles/minute). Each pump was set to median levels for vacuum and cycle ranges, which equated to P1 set at 137.5 mm Hg and 45 cycles/minute, and P2 at 175 mm Hg and 66 cycles/minute for the observations. Each pump flange was fitted to each participant individually to ensure that the nipple moved freely with little space around the nipple in the breast flange tunnel, without areolar tissue moving into the flange tunnel, and with no discomfort at the onset of pumping.
Mitutoyo Absolute IIP66 digital calipers were used for all nipple diameter and length measurements, with accuracy to 0.01 mm. Calipers were calibrated weekly to assure accuracy and researchers were trained on proper and accurate use of all the equipment using Abbe's principle of alignment that “a linear reading should be taken either inline or sideways of the object,” 15 inline for length and sideways for diameter. Researchers were validated on the use of the calipers by repeating a series of measurements until there was no statistical difference between researchers' measurements. Each measurement was recorded in millimeters to two decimal points (such as 8.57 mm) and repeated three times. The average of the three measurements was recorded as the number to be used for analysis.
As there are structural differences between right and left breasts, 16 only the right breast evaluation was recorded at each session for standardization purposes. Each milk transfer session was observed by the researcher with measurements taken immediately at the end of the 15-minute milk transfer session. BF was the first modality observed and used as the “gold standard” for purposes of comparison with each participant as her own control.
At the BF observation, at the end of 15 minutes, the mother removed the infant from the breast for measurements and the infant was returned to the breast if desired by the mother or infant. If the infant was fed before 15 minutes, measurements were taken at the time. Fifteen to 20 minutes was the manufacturer-recommended amount of pump use time. The lesser amount of 15 minutes was used for the amount of pumping time, to standardize the procedure for all participants. The recorded value of nipple diameter and length was the mean of three measurements rounded to two decimal points. The researcher documented any visible physical changes such as erythema and swelling of the nipple, areola, or breast tissue texture immediately after the milk transfer session and then again after a 20-minute rest period.
Visible changes were specifically noted in each case with particular care in describing inflammation using the traditional signs of pain, calor (increased heat), rubor (reddening), and swelling. Swelling was defined by tissue changes causing edematous, boggy appearance to the nipple and areola with associated calor, rubor, and an irregular contour to the affected breast tissue. Pain was recorded using a slightly modified Wong–Baker FACES Pain Scale, 17 used by the participants to assess their pain level at the end of each milk transfer session (Fig. 1). The researcher documented the participant's stated score at the end of each milk transfer session. After a 20-minute rest period, the nipples were observed for any changes at which time the session was concluded.
A modified Wong–Baker Pain Scale was used to evaluate the participants' perceived pain.
Data analyses
Descriptive statistics were used for demographic data. For each participant, t-tests were used to compare milk transfer modalities for changes in nipple diameter and length measurements. Within-subject modality differences and pairwise comparisons were done with Bonferroni adjustment used for multiple comparisons. Statistical significance was set at p < 0.05.
Results
Sample characteristics
Fifty eligible women were identified, and 46 women agreed to participate in the study. The women ranged in age from 23 to 38 years of age with a mean age of 26.5 years. The infants ranged in age from 2 to 3 months, with a mean age of 2.4 months. Complete data were collected for 41 of the participants. Five of the 46 women did not hand express but completed all other aspects of the study with one breastfeeding session and the two pumping sessions in randomized order. The five who did not hand express had HE as the last randomized modality and chose to opt out of the study before that modality. The data collected from these five were used in the data analysis for the other modalities for an n = 46.
The “before” measurements for all modalities were not significantly different, with the mean values shown in Table 1 indicating that the nipples had returned to premodality measurements before the following modality.
Mean Values with Standard Deviation for “Before” Nipple Diameter (mm) and Length (mm) Were Not Significantly Different
BF, breastfeeding; HE, hand expression; P1, Purely Yours®; P2, Pump In Style®.
Nipple diameter and length
For milk transfer via BF and HE, the mean values of “before” and “after” measurements for nipple diameter and length had no statistical significant difference, as shown in Figure 2. The after values for P1 and P2 for nipple diameter were significantly different from their respective before values and when compared to the BF and HE measurements at p ≤ 0.003.
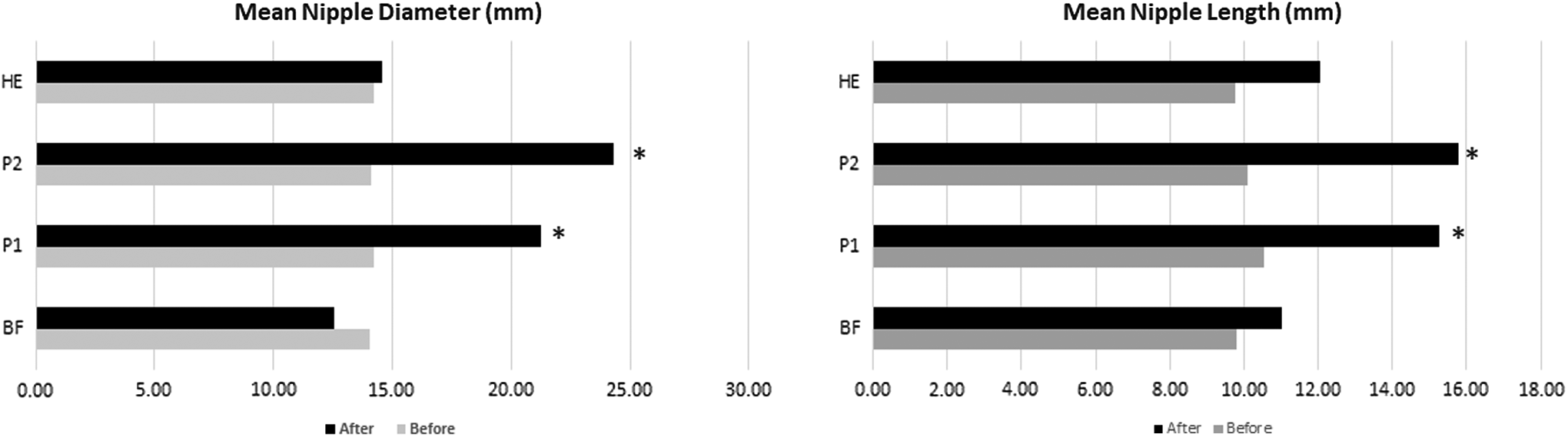
Mean values for nipple diameter (mm) and length (mm) before and after milk transfer. The “before” means for diameter and length were not statistically significant for any of the milk transfer sessions. *The “after” means were significant for P1 and P2 with p < 0.003. P1, Purely Yours; P2, Pump In Style.
The mean values for P1 and P2 were significantly different from the BF after mean for length and diameter with p < 0.000, as shown in Figures 3 and 4. Overall, for BF, the mean nipple diameter was 14.06 mm (±2.52) before breastfeeding and 12.55 mm (±2.67) after milk transfer. Nipple length was 9.80 mm (±2.76) before BF and 11.01 mm (±2.92) after BF. The descriptive statistics for pairwise comparisons for within participants are shown in Table 2, with the mean differences for pairwise comparisons for within-subjects nipple diameter and length, shown in Tables 3 and 4.
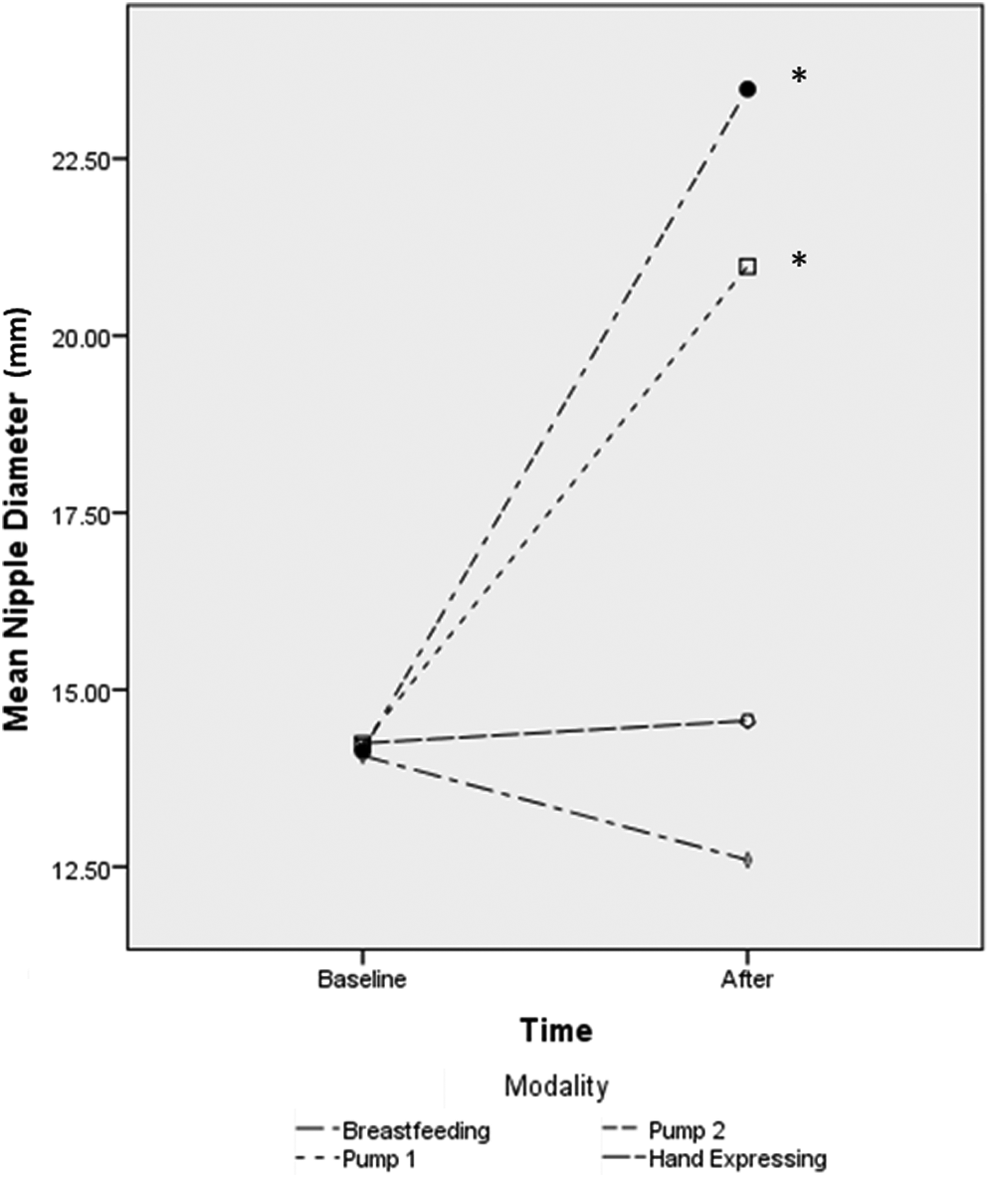
Mean values for nipple diameter and length before and after milk transfer. The “before” means for diameter were not statistically significant for any of the milk transfer sessions. *The “after” means were different from the breastfeeding “after” mean for P1 and P2 with p < 0.0002.
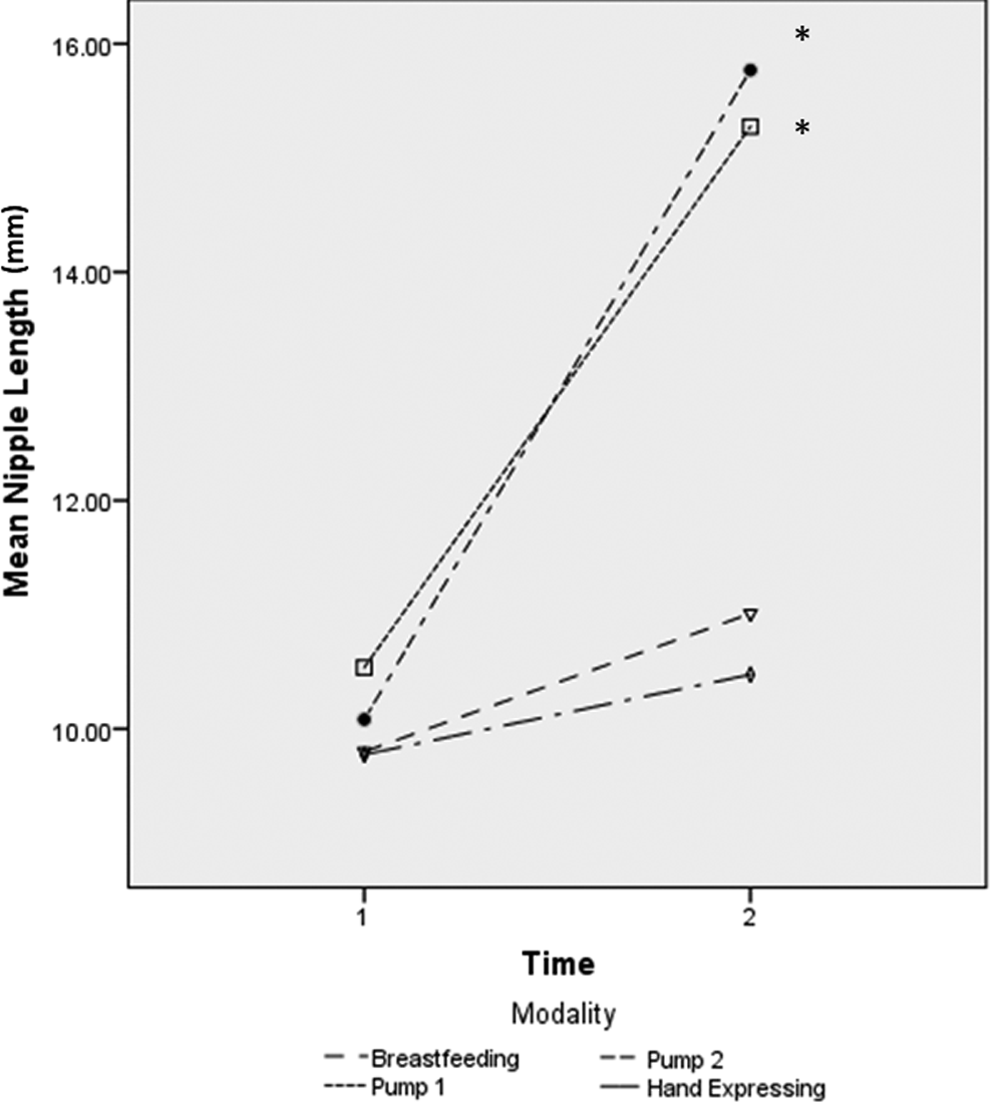
Mean values for nipple length before and after milk transfer. The “before” means for diameter were not statistically significant for any of the milk transfer sessions. *The “after” means were different from the breastfeeding “after” mean for P1 and P2 with p < 0.0002.
Diameter and Length Descriptive Statistics in Millimeters
Pairwise Comparisons of Nipple Diameter in Millimeters
Based on estimated marginal means.
Adjustment for multiple comparisons: Bonferroni.
The mean difference is significant at the 0.05 level.
Pairwise Comparisons of Nipple Length in Millimeters
Based on estimated marginal means.
Adjustment for multiple comparisons: Bonferroni.
The mean difference is significant at the 0.05 level.
Visible changes
Visible changes of nipple, areola, or the breast tissue were noted after BF for only one participant upon disengaging the infant from the breast. The infant had compressed the nipple into a point on the upper rim of the nipple (often referred to as a “lipstick shape”).
Visible changes of the nipple, areola, or the breast tissue were noted by the researcher for all but one of the women (n = 45) using P1 at the end of each milk transfer session; 20 (44.4%) had only swelling, while 25 (55.6%) had erythema and swelling. For the P2, visible changes of the nipple, areola, or the breast tissue were noted by the researcher for all 46 of the women at the end of the milk transfer session with 18 (39.1%) exhibiting swelling only, while 28 (60.9%) also had erythema.
No erythema or swelling was noted for HE. The visible changes noted after P1 and P2 remained unchanged after the final evaluation at the completion of the 20-minute rest period. The nipple diameter and length had not returned to prepumping modality measurements at the end of the 20-minute resting period when the participants completed that observation and were released to leave.
Pain
On the pain scale for BF, none of the participants experienced greater than 3 on the pain scale with a mean of 0.6, indicating little if any pain, as shown in Table 2. The participant who had the lipstick-shaped nipple reported a 3 on the pain scale. For the P1, the mean pain score was 3.3, indicating that “it hurts,” while for the P2, the mean pain score was 5.5, indicating between “hurts a little more” and “hurts even more.” After pumping with P1, 36.9% (n = 17) of participants had erythema and swelling corresponding with a pain score of >3 with milk transfer. For P2, 73.9% (n = 34) of participants had erythema and swelling accompanying a pain score of >3 after milk transfer. Overall, across pump use, 91.3% (n = 42) of mothers had a pain score >3, with a total mean of 4.9 indicating pain midway on the pain scale. Comparatively, for HE, none of the participants reported >3.
Our study has some limitations. The sample was a convenience sample and many of the participants had received lactation guidance from an international board-certified lactation consultant early in their lactation, which may have improved their baseline breastfeeding experience. Only one episode of each method of milk transfer was observed, leaving the effect of repeated pumping episodes unknown. As an observational study, the researchers attempted to interfere as little as possible during pumping sessions.
Although each participant in this study had the pump flange sized correctly before pumping and the vacuum setting remained the same throughout the pumping session, this criterion allows for error in fitting as some participants may have needed a change in flange size midpumping session to accommodate changes in nipple size. Another limitation was pumping time. The amount of time spent pumping was set at 15 minutes as per the manufacturers' recommendation rather than stopping the pump when milk stopped flowing. This may have caused “dry” pumping if the breast was completely emptied in less than 15 minutes and increased the risk of discomfort.
Discussion
Our study concurs with Geddes et al. 18 that nipple lengthening, which can be seen on ultrasound during breastfeeding, is a normal phenomenon. However, while there was some nipple lengthening during breastfeeding, there is no significant increase in length of the nipple once the baby disconnects from the breast, ending the latch. The lengthening and the decrease in diameter of the nipple for the BF and HE modalities were transitory and may be explained by the contraction of the muscle cells surrounding the nipple itself as occurs when the nipples are exposed to cold or are stimulated becoming firmly evert.
Our study found erythema, swelling, and pain in many of the participants with use of mechanical device for milk transfer. The participants who had more than one visible change also had higher scores on the pain scale. The abnormal enlargement of nipple diameter and length seen after some of the mechanical milk transfer sessions, we argue, is soft tissue injury. In clinical terms, swelling is defined as the gross anatomic result of the inflammatory process. Additively, soft tissue injury is defined by the presence of swelling accompanied by pain and possibly discoloration. 19 When repetitive friction, pulling, twisting, or compression of tissue occurs, an “overuse” injury can occur from inappropriately directed, and often increased, force on the tissues. 19 Based on these definitions, we believe that women experiencing pain, erythema, and swelling of the breast tissue when using breast pumps to transfer milk are experiencing soft tissue injury.
This work revealed that, for some, there are changes in breast tissue when using a mechanical pump that warrant the study of possible biomechanical causative factors and long-term impact to breast health. Although these data were taken from a relatively small sample size, they raise concerns about the underlying damage that may be occurring when the participants were experiencing breast tissue changes accompanied by pain. In this study, when the participants experienced pain using P1 and P2, they had significantly greater diameter and length of nipple tissue as well as swelling and discoloration. Contrastingly, during BF, if present, elongation of the nipple did not persist past 5 minutes nor was there discoloration of the tissue.
Pain is a common complaint 20 and although we have recently identified and improved our abilities to define several pathologic presentations such as torticollis or tethered oral tissues, many mothers and infants go without resolution to lactation difficulties. Many do not have access to lactation care professionals. In our experience, even when having challenges with breastfeeding, mothers often do not seek professional help.
The access to lactation support in this study may have correlated to the average pain score in this study, being 0.60, indicating no pain with BF. In contrast, for the breast pumps, the participants on average reported pain >3 (“it hurts”). If women routinely experience pain during pumping, this puts them at-risk for breastfeeding cessation.21,22 Even though the reported prevalence of transitory nipple discomfort is as high as 96% during the first week of lactation, and perceived by some as clinically normal, pain is a risk factor for breastfeeding cessation.23,24 Pain is considered an indicator of tissue damage. 25
Any discomfort during breastfeeding should not be dismissed, as there is evidence reported in the medical literature as far back as 1948 that women experiencing pain during breastfeeding had an infant with decreased milk intake. 22 Pain during direct breastfeeding has been discussed as leading to premature weaning.25,26 Women, who experience pain during breastfeeding, may choose to provide their infant with milk from a bottle, and practically speaking, those who experience pain with the use of a breast pump may discontinue providing their milk for their infant.
Previous literature has identified that pain may also be caused by improper use of a pump, which can lead to swelling as well as nipple and breast tissue damage. 27 It is incumbent upon all lactation care providers to understand and fit breast pumps properly with their patients before and during a pumping session. Addressing pain with pump use is of increasing importance in a society filled with working mothers who want to provide their milk for their infant. Pang et al. 28 summarize the clinical implications as follows: “Mothers who fed their infants EBM (expressed breast milk) exclusively, but not those who practiced mixed feeding, were at a higher risk of terminating breastfeeding earlier than those who fed their infants directly at the breast.” Optimally, every person who uses a breast pump would have a lactation professional to assist in fitting, determining the most effective vacuum settings, and the amount of pumping time to minimize the risk of any tissue damage.
Conclusions for Practice
In this study, although the use of the pumps was correct and done under the supervision of highly lactation-experienced professionals, many of the participants still reported pain with erythema and/or swelling evident for 20 minutes or more after the use of pumps. The implications of these findings suggest that well-trained lactation professionals need to evaluate and educate lactating women throughout their pumping session to attenuate risk of nipple trauma in real-time evaluation of maternal skin sensitivity, pain, response to pressure, and volume of milk transfer.
We concur with Flaherman et al. 29 who encouraged clinicians to assess milk transfer shortly after initiating pumping to better assist the lactating woman. In addition, better designed breast pumps and flanges improved knowledge of flange fitting, and better directions from manufactures may decrease the risk of nipple, areolar, and breast trauma. Further study is needed to fully understand pumping efficacy in relation to breast emptying with no distortion of the tissue. It is unknown whether there is a lasting negative impact to the nipple, areola, or breast tissue with the use of electric breast pumps. Additional research is needed to clarify long-term ramifications for women who experience pain, swelling, and erythema when using breast pumps over a period of weeks and months.
Footnotes
Acknowledgment
The authors thank the mother/infant dyads who participated in this study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.