
Abstract
Abstract
Background:
MotherSafe is a free telephone-based counseling service for Australian consumers and health care providers concerned about drug exposures during pregnancy and breastfeeding. Calls relating to breastfeeding are relatively common and a source of significant distress to the breastfeeding mother, particularly if there is a lack of clarity regarding possible adverse effects of drug exposure on the infant. This study seeks to identify the medication exposures of concern for breastfeeding mothers and the information available to address these concerns.
Aims:
To review calls to MotherSafe about breastfeeding drug exposures during the 19-year period from 2000 to 2018 and to highlight drugs of concern and counseling issues.
Materials and Methods:
A retrospective descriptive assessment of a prospectively collected Access database was undertaken. Phone counseling records identified the medication (and other) exposures of concern regarding breastfeeding. The information about medication exposures via breastfeeding provided in consumer and product information (PI) was also reviewed.
Results:
Of a total of 315,158 calls received at MotherSafe between 2000 and 2018, 116,876 (37.1%) were regarding drug exposure via breastfeeding; 30% of these calls related to nonsteroidal anti-inflammatory drugs, antihistamines, antidepressants, simple analgesics, and antibiotics, and 5% were regarding an exposure specifically contraindicated when breastfeeding.
Conclusions:
Queries about medication exposures via breastfeeding represent a significant proportion of all the counseling calls to MotherSafe. This study demonstrates the inconsistent and often misleading information about breastfeeding exposures found in consumer and PI sheets and online and highlights the important role of Teratogen Information Services like MotherSafe in providing evidence-based information to both consumers and health care providers.
Introduction
MotherSafe was established in Australia in January 2000 as the New South Wales (NSW) Statewide Teratogen Information Service (TIS). 1 Modeled on similar services around the world, it is a free-of-charge telephone-based service, staffed by trained health care professionals (HCPs), providing evidence-based counseling to both consumers and HCPs about drug exposures during pregnancy and breastfeeding.
Breastfeeding women take fewer medications and tend to be more reluctant to take medications compared with nonbreastfeeding women.2–4 Although available human data for infant drug exposures via breast milk are generally lacking, pharmacokinetics-based computer modeling of infant drug exposure levels predicts for levels that are <1% of initial maternal exposure, the risks of adverse effects in the offspring are low.5,6
Calls to the TIS and patient surveys about exposures during breastfeeding suggest that there are concerns and widespread unease regarding the safety of prescription medication, over-the-counter (OTC) medication, and complementary medicines (CAMs) to breastfed infants.7,8 Moreover, product information (PI) and consumer medicine information (CMI) rarely provide information specifically related to breastfeeding (“No lactation data available”).
Paucity of information creates anxiety and means that HCPs (e.g., general practitioners [GPs], pharmacists) are unable to provide definitive consistent information.8–12 Unprecedented access by consumers to vast amounts of online information that is being used to make medical decisions is a well-recognized problem.13,14 Data quality is highly variable, and consumers can have difficulty in contextualizing the large quantity of complex and often conflicting information for their own personal situation.
All these factors create significant anxiety for the breastfeeding mother concerned about the effects of medications on her infant and may result in women taking an “over-cautious” approach and terminating breastfeeding or medication, thereby unnecessarily depriving both infant and nursing mother of the known benefits of breastfeeding. 15
In Australia, the National Health and Medical Research Council (NHMRC) recommends exclusive breastfeeding for 6 months, continued alongside complementary food until at least 12 months. 16 The rates of breastfeeding in Australia are currently below these recommended guidelines. 17 It is thus important for services like MotherSafe to exist to give evidence-based counseling and general reassurance, as well as discussing rational medication use for breastfeeding women.
These studies report calls made to MotherSafe about breastfeeding drug exposures over a 19-year period and highlight some of the counseling issues and medications of concern.18,19
Materials and Methods
A retrospective descriptive study was conducted to examine MotherSafe call data for the 19-year period from January 2000 to December 2018.
Data from calls made to MotherSafe were entered into the MotherSafe database on a daily basis. Minimum data collected include the following: caller name, type of caller (consumer or HCP), how the service was found (repeat caller, referred by HCP), maternal age, postcode and telephone number, reason for call (i.e., pregnant, planning pregnancy, or breastfeeding), and the exposure of concern.
An exposure was defined as contact, ingestion, inhalation, or injection of a prescribed or OTC medication, radiation, chemical, substance, infection, or food. Exposures are grouped into one of 40 categories based on its general class. If callers mentioned several potential exposures during a call, these were each listed separately. The following was excluded: “General inquiry with no specific named exposure.”
Aggregate data for the number of calls received by MotherSafe were extracted for the 19-year period from 2000 to 2018 and examined in a retrospective, descriptive, and nonidentifiable manner for calls from consumers and HCP concerning breastfeeding.
Information from the MotherSafe database was reviewed for any spelling mistakes and omitted details during data entry. Subsequently, data analysis was performed manually using Microsoft Excel for reason for call and exposure type. Data were analyzed for demographic factors, type of exposure, and reason for inquiry by date of call and type of caller (consumer or HCP). Descriptive statistics were calculated.
Data were further analyzed using Hale's Medications and Mothers' Milk 2019. 20 In this textbook, data on medications are evaluated and then classified into five categories of lactation risk: L1: safe drugs at the highest level, L2: safe drugs, L3: moderately safe drugs, L4: possibly dangerous drugs, L5: contraindicated drugs. Monthly Index of Medical Specialties (MIMS), a compiler of medical information available in Australia, was searched for drugs specifically contraindicated in breastfeeding using the terms “lactation” and “breastfeeding.”
The study was approved by South East Sydney Illawarra Area Health Service's Human Research Ethics Committee, reference number 10/197 (2011).
Results
In total, MotherSafe received 315,158 telephone inquiries during the period 2000–2018. Of these, 116,876 calls (37.1%) were regarding exposures during breastfeeding. Figure 1 illustrates the number of inquiries regarding breastfeeding exposures by year. Consumers (breastfeeding mothers or their family/friends) accounted for 73.0% of all calls, whereas HCPs (GPs, genetic counselors, clinical geneticists, pharmacists, midwives, early childhood nurses, lactation consultants, obstetricians, psychiatrists, pediatricians, and mental health teams) comprised the remainder of callers.
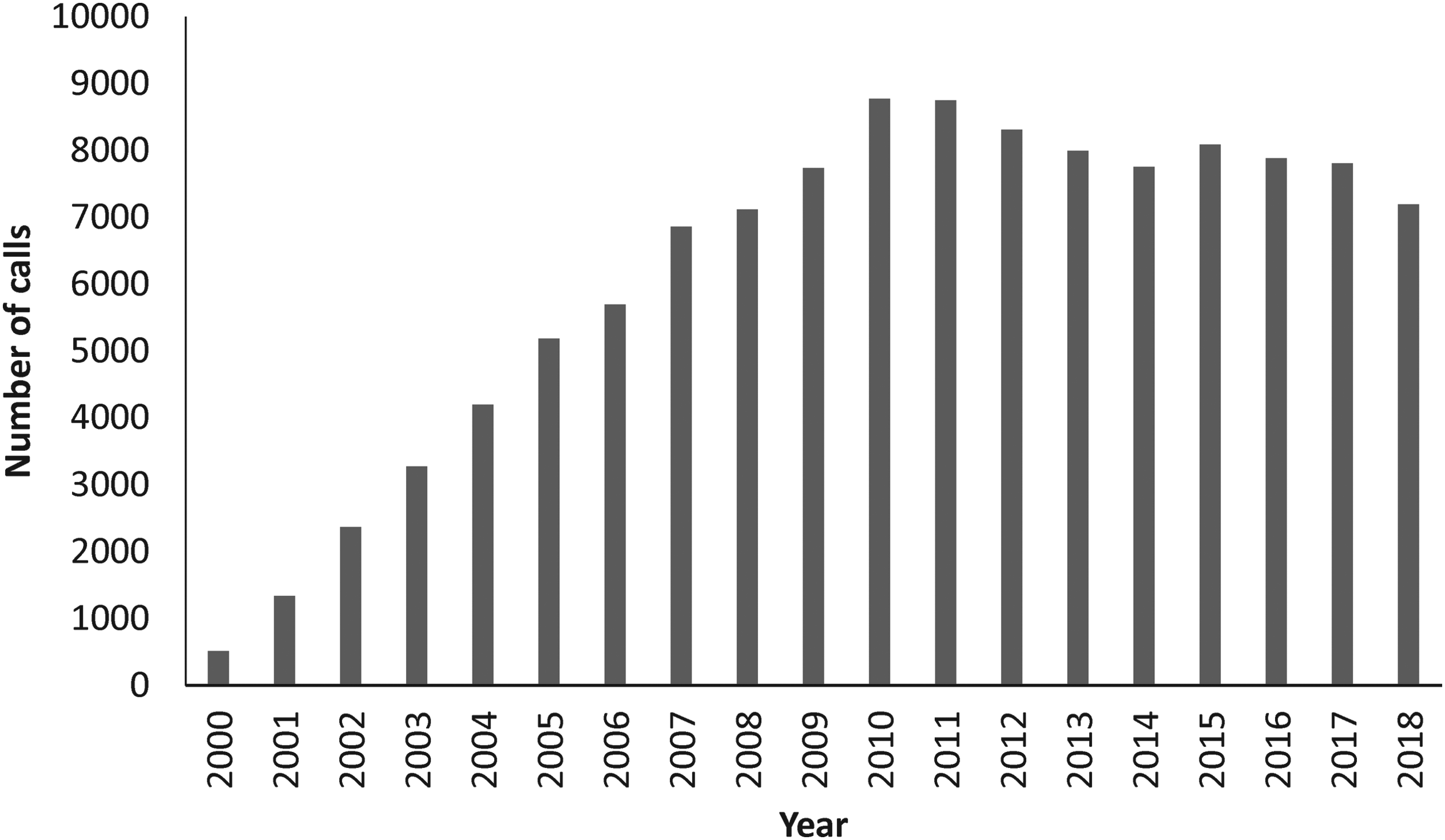
Number of breastfeeding inquiry calls to MotherSafe from 2000 to 2018.
More than 50% of calls (53.0%) were prompted by the patient's own initiative, with the vast majority repeat callers. The remaining consumers were recommended to call MotherSafe by health care providers, notably early childhood consultants (7.6%), GPs (6.1%), midwives (4.1%), and hospitals (8.4%).
Queries by consumers related to more than one exposure of concern in 65.7% of calls, whereas calls from HCP (GPs, midwives, early childhood consultants, and pharmacists) tended to focus on one specific query (58%).
Exposure to pharmaceuticals accounted for 90% of all queries, with an additional 4.4% related to CAMs, 1.5% to alcohol and substances of abuse, and 1.2% to imaging. The most common pharmaceutical exposures from consumers related to nonsteroidal anti-inflammatory drugs (NSAIDs), antihistamines, antidepressants, simple analgesics, and antibiotics comprising ∼30% of all calls. Calls from HCPs specifically also related to antibiotics and antidepressants and also included central nervous system (CNS) agents, cardiovascular drugs, and other prescription medications (46%).
The most frequent calls to MotherSafe from all callers (>2,000) regarding individual medications included ibuprofen, paracetamol (known in the United States as acetaminophen), loratadine, diclofenac, and sertraline (Table 1). In the last 5 years, the proportion of queries regarding antipsychotics, CNS active drugs (including general anesthesia, oxycodone, diazepam, and temazepam), topical medicines, CAMs, and vitamin/minerals has consistently increased (Fig. 2).
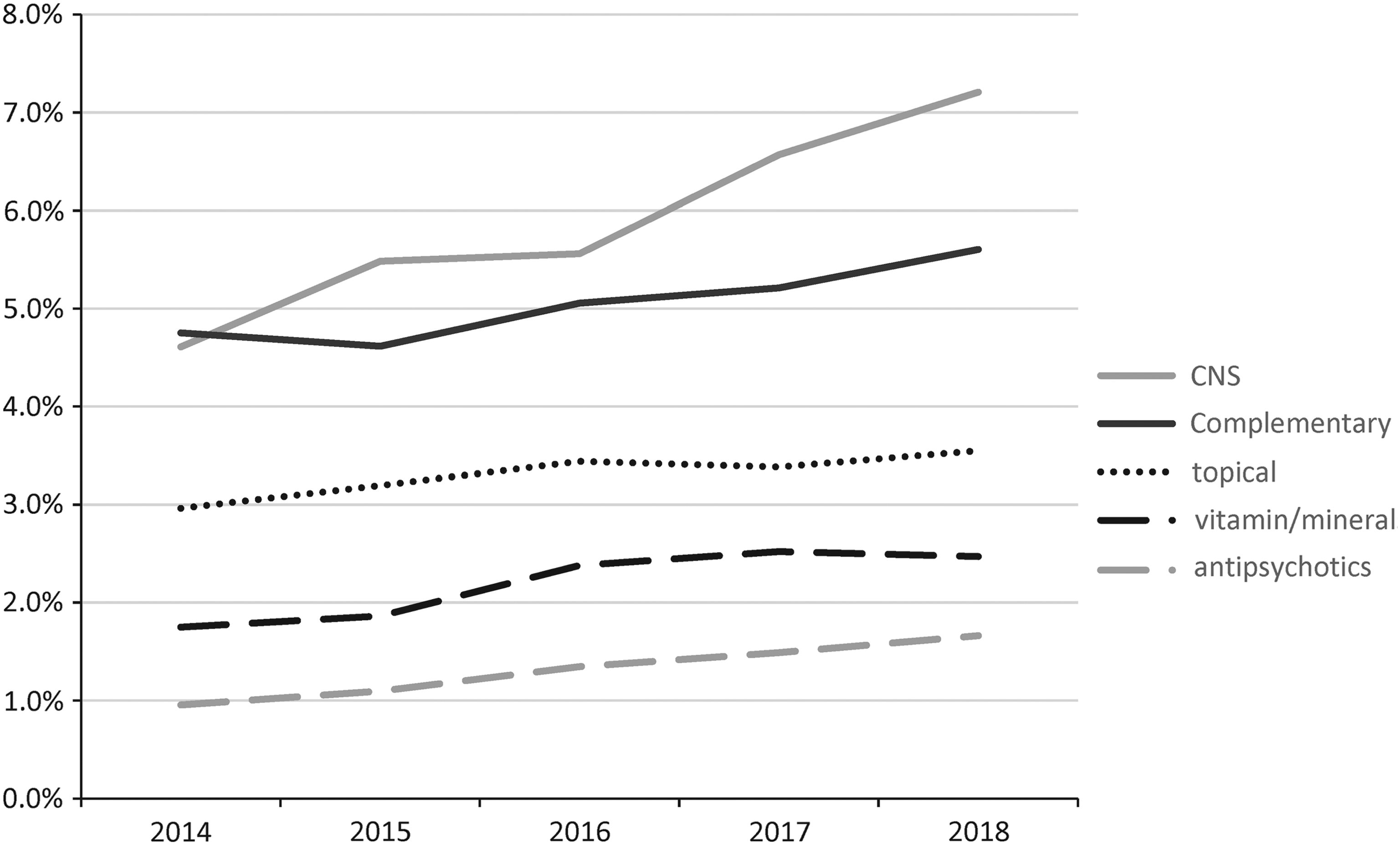
Frequency of calls to MotherSafe by medication class over time.
Most Common Inquiries to MotherSafe Concerning Breastfeeding (>2,000 Calls)
NSAID, nonsteroidal anti-inflammatory drug.
There were calls (4.4%) regarding nearly 200 different CAM products as well as generic questions (15%) regarding CAMs. The most common specific inquiries were regarding Echinacea (10.6%), fenugreek (7.1%), St John's Wort (6.1%), lysine (5.8%), melatonin (4.3%), and valerian (4.2%).
A search of drugs specifically contraindicated during breastfeeding by MIMS yielded conflicting results. For example, three of eight doxycycline preparations are specifically contraindicated, whereas ibuprofen, metoclopramide, propofol, and glyceryl trinitrate (known in the United States as nitroglycerin) are all contraindicated in at least one (but not all) listed preparation. Only 5% of all queries were regarding an exposure specifically contraindicated by MIMS or categorized as L5 (i.e., hazardous) or L4 (i.e., possibly hazardous) in Medications and Mothers' Milk 2019. 20 The most common calls included codeine (only L5 in mothers who are ultra-rapid metabolizers), amitriptyline, nifedipine, and metformin (Table 2). Although categorized as L2 (i.e., probably compatible), a large number of calls (n = 1,631) were regarding aspirin, which according to Medications and Mothers' Milk 2019 20 should be “avoid[ed] … at high doses in lactation when the infant has a viral syndrome,” due to the risk of Reye's syndrome in the infant.
The 10 Most Common Calls Relating to Exposures Contraindicated in Breastfeeding
L5: hazardous; L4: possibly hazardous. 20
MIMS, Monthly Index of Medical Specialties.
Discussion
This study examined almost 300,000 calls to the NSW Statewide TIS, MotherSafe. Approximately 37% of the calls concerned exposures during breastfeeding, which is similar to those reported by another TIS (34.2%), MotherToBaby, a service provided by the North American Organization of Teratology Information Specialists. 8 Numerous studies have noted the high prevalence of drug exposures during breastfeeding. The majority of breastfeeding women need to take at least one medicine, either for acute illnesses such as infections or chronic conditions such as epilepsy. 21 Exposures including prescription (68%), OTC medication (93%), or homeopathic medication, including herbs (36%), have been reported, 22 with high rates of self-administration (66%). 21 A recent systematic review suggests that at least 50% of women took at least some form of medication during the postpartum period, increasing to 100% if vitamins/minerals were included. 23
Over the past 19 years, antibiotics, NSAIDs, antihistamines, simple analgesics, and antidepressants have been the most common breastfeeding exposure calls to MotherSafe. The most common individual agents were ibuprofen, paracetamol (acetaminophen), loratadine, diclofenac, sertraline, and cephalexin. Most of these medications treat either chronic conditions (depression, anxiety, and asthma) or common acute symptoms (pain, constipation, cold and flu, allergies, and infections) or were specific to breastfeeding (i.e., the galactagogue domperidone). This is consistent with other studies of drug exposures during breastfeeding,2,21,22 suggesting that the MotherSafe calls reflect general population breastfeeding exposures.
Calls to MotherSafe regarding galactagogues were recently reviewed, 18 with domperidone being one of the most common exposures by individual drug. In this context, it is assumed that domperidone was being taken for its purported galactagogic effect rather than to treat nausea and vomiting or gastroparesis. In the current study, the most common herbal galactagogue inquiries were those regarding fenugreek (7.1% of calls). Traditionally, fenugreek is used to increase milk supply, although there is limited supporting evidence.
CAMs are therapeutic goods that have one or more designated active ingredients, each of which has an established identity and traditional use. 24 They include vitamins, minerals, herbs, nutritional supplements, aromatherapy, and homoeopathic products, often taken to treat the same conditions as traditional medicines, that is, cold and flu, depression, and low milk supply. Exposure to CAMs during breastfeeding comprises 4.4% of all calls to MotherSafe, with the most common inquiries regarding Echinacea (10.6%), fenugreek (7.1%), St John's Wort (6.1%), lysine (5.8%), melatonin (4.3%), and valerian (4.2%).
Most CAMs contain multiple compounds, and differences are often found between labeled and actual ingredients or their amounts. In some cases, the compound thought to responsible for the CAMs biologic activity is known and can be traced in maternal serum and breast milk. However, for most CAMs, this information is not available, so drug levels and potential effects on breastfed infants are unknown. In general, MotherSafe would advise that regulated medications have better safety and efficacy data available than the CAMs, and thus, the recommendation would be to use one of these in preference to a CAM while breastfeeding.
The high number of calls to MotherSafe and the frequency of medication exposure in breastfeeding women suggest that issues regarding medications during breastfeeding are common concerns for breastfeeding women. Some women report that they stopped breastfeeding to avoid exposing their infant, did not use medications because of breastfeeding, or did not breastfeed because of medication use. 2 In another study, 38.2% of nonlactating women chose not to initiate lactation due to medication and 16.5% of lactating participants took measures such as stopping medication during breastfeeding or temporarily feeding infant formula to their infants. 22 Worryingly, many women also delayed or refused needed medication to breastfeed.2,25 A recent Italian study found that some women used CAMs rather than a prescribed medicine as CAMs were perceived as safer. 26
In the last 5 years, there has been an increasing trend in frequency of queries regarding CNS active drugs, including oxycodone, diazepam, and temazepam. All are excreted into human breast milk in low quantities,27–29 and because of the potential to cause sedation in the newborn, they are generally not recommended for use in breastfeeding in PI provided by the manufacturer.
However, these recommendations tend to be oversimplistic, not considering dose or duration of exposure. For example, infant sedation is observed following oxycodone exposure but generally only at high doses, 30 diazepam has a long half-life, but single use is unlikely to result in significant accumulation, whereas temazepam is relatively water soluble and partitions poorly into breast milk. 31 Data relate to a single agent; however, polytherapy is common and risk to the infant is likely to increase as a result of possible additive toxicity or specific drug interactions.
In this study, only 5% of queries concerned exposures contraindicated while breastfeeding in Medications and Mothers' Milk 2019 20 or MIMS. This included codeine that is only contraindicated in ultra-rapid metabolizers. Nifedipine use in breastfeeding is contraindicated by MIMS, but this recommendation appears to be based on insufficient information and passage into breast milk; there are no reported adverse findings in infants so exposed.
There are relatively few drugs absolutely contraindicated during breastfeeding. These include isotretinoin, amiodarone, cytotoxic chemotherapy, gold salts, iodine, and certain radiopharmaceuticals such as iodide (131I).3,31 Recreational drugs such as cocaine, methamphetamine, and ecstasy are often also included in this list. 31 Exposure to cytotoxic drugs has been associated with infant bone marrow suppression, whereas iodine and amiodarone can affect thyroid function and gold salts are associated with hematological abnormalities. High-dose methotrexate used in cancer therapy is contraindicated by MIMS during breastfeeding; however, a recent study has demonstrated no adverse affects in the breastfed infant of a mother with rheumatoid arthritis taking low intermittent doses of methotrexate. 32
Around 1.2% of all calls related to radiocontrast or imaging. If used only when essential for a diagnosis, the benefits from the use of ionizing radiation exceed the risks to the breastfed infant, and the use of all contrast agents is considered safe during breastfeeding. 33
The main reasons women may be anxious and decide not to breastfeed or cease medication include lack of data and receiving conflicting advice. In MIMS, PI provided by different manufacturers of the same drug gave conflicting advice, with some specifically contraindicated during breastfeeding. Common examples of differing advice during breastfeeding included doxycycline, ibuprofen, metoclopramide, propofol, and glyceryl trinitrate (nitroglycerin). This is similar to the discordance found by Brown et al. 34 when they compared breastfeeding statements within Australian PI and CMI with other resources such as the Drugs and Lactation Database (LactMed) and the Australian Medicines Handbook. Women require adequate and consistent data to enable them to make informed choices.
Breastfeeding advice in PI and CMI usually does not take pharmacokinetic considerations, such as concentration of drug in milk, protein binding, molecular weight, oral bioavailability, or absorption from the infant's gut into account when advising against breastfeeding. Genetic differences will also affect the metabolism of drugs, such as ultra-rapid metabolizers of codeine. While many drugs do in fact enter human milk, most are at concentrations that would rarely cause serious adverse events in the newborn.35–37 Many current guidelines use a categorical system of three to five levels of risk, 38 with the most restrictive being contraindicated use due to significant and documented risk to the human infant with a clearly negative risk–benefit ratio.
A further source of confusion is in the misperception that pregnancy drug categorization is applicable to breastfeeding. In a Norwegian survey of drug use in breastfeeding women, Matheson et al. 39 found that more than half of the women believed that the risk of drug use during breastfeeding was similar or higher than use of the same drugs during pregnancy.
One of the strengths of this study was the large amount of data, including demographic data, the drug exposure of concern, and reason for inquiry for example, breastfeeding, collected from ∼300,000 callers to the MotherSafe database. One of the limitations of the study was the reliability of data entry into the original database, although steps were taken to account for this such as checking for spelling and standardization of drug categories. Other limitations are that the study was not able to capture information seeking of people who did not call, and it is not known if callers to MotherSafe followed the advice given.
Conclusions
Approximately 300,000 calls to MotherSafe over a 19-year period demonstrated high levels of drug exposure by breastfeeding women, including drugs specifically contraindicated while breastfeeding. It also demonstrated the concern of consumers regarding the exposure of nursing infants to prescription medications, CAMs, and other drugs. Unfortunately, most consumer and PI sheets and online information sources continue to provide inconsistent and often misleading information, which may result in some women stopping breastfeeding unnecessarily, not taking needed medications, or not starting breastfeeding at all. The study indicates the important role of TIS like MotherSafe in providing evidence-based information to both consumers and health care providers.
Footnotes
Disclosure Statement
No competing financial interests exist.