
Abstract
Abstract
Objective:
This study explores the congenital diaphragmatic hernia (CDH) infant–mother dyad with regard to maternal lactation outcomes and infant exposure to a human milk diet.
Study Design:
This was a retrospective descriptive cohort study conducted at Children's Hospital of Philadelphia. A total of 149 infants born with CDH and admitted to the Newborn/Infant Intensive Care Unit (N/IICU) were included in the study.
Results:
Of 149 mothers, 141 (95%) initiated pumping for their CDH infants. At discharge from the N/IICU, 79% (n = 118) of infants were being fed human milk. Among those discharged on human milk, 55% (n = 65) were discharged being fed unfortified human milk with 9% (n = 11) being fed unfortified maternal hind milk.
Conclusion:
This research demonstrates that mothers of CDH infants can effectively establish and maintain a complete milk supply and that the majority of infants with CDH can receive a human milk diet for the entire hospital stay.
Introduction
The diagnosis of congenital diaphragmatic hernia (CDH), a malformation of the diaphragm that allows the abdominal viscera to herniate into the chest, is associated with an incidence of 1.7–5.7 per 10,000 births. 1 In a recent study, Balayla and Abenhaim described the incidence, predictors, and outcomes of CDH in the United States with an incidence of 1.93 per 10,000 births and a 1 year mortality rate of 46%. 1 Infants with CDH are at an increased risk of malnutrition postoperatively.2–4 The reasons are likely multifactorial, including increased energy expenditure while weaning respiratory support, pulmonary hypertension, lung hypoplasia, and increased incidence of gastroesophageal reflux/disease. 5 It has been established that human milk is the ideal feeding for all infants, including those with CDH. 6
Infants with CDH may particularly benefit from a human milk diet. 7 Human milk feedings are associated with improved feeding tolerance and decreased number of days on total parental nutrition in other surgical populations. 8 Human milk is important to protect the developing infant's brain especially because CDH infants are at risk for developmental delays. 9 Infants with CDH are also at increased risk for respiratory infections including respiratory syncytial virus (RSV). Human milk/breastfeeding decreases the risk of both upper and lower respiratory infections as well as RSV.1,6,7 However, practitioners may be concerned about infants with CDH receiving an exclusive human milk diet because of poor growth related to increased metabolic demands. 10 Infants with CHD may also have enteral feeding volume restrictions, secondary to pulmonary hypertension or ventricular dysfunction. 10 Both metabolic demands and volume restrictions often result in increasing the caloric density of human milk or formula to achieve appropriate growth. 10
This study is an exploration of the CDH infant–mother dyad with regard to breastfeeding, lactation, and infant exposure to a human milk diet. Research from other centers demonstrates that not all women receive evidence-based lactation care 11 despite the fact that there are well-established models of care with proven outcomes to support human milk feedings in vulnerable infants. 12 Some providers may believe human milk and breastfeeding is not possible for the infant with CDH. Given the literature on the benefits of human milk for all infants and our work in developing innovative approaches for human milk and breastfeeding for vulnerable infants, we sought to understand the lactation experiences of one of the vulnerable mother–infant dyad relationships in a large cohort over multiple years. Recent qualitative studies have highlighted the experiences of breastfeeding among the mother–CDH infant dyad.13,14 Mothers report that expressing milk for their infant with CDH was an important part of them providing care for their infants and that by participating in human milk oral care they felt bonded to their infant and allowed them to participate in their infants' care.13,14 In addition, mothers reported having the goal of direct breastfeeding their infants but also were realistic about their infants' ability to orally feed and were happy as long as their infants received their milk. 14 Clearly mothers report that the provision of human milk and breastfeeding is an important component of having a critically ill child.13,14
Materials and Methods
The study team sought to understand the lactation experiences of mothers with CDH infants including maternal pumping initiation and the ability to effectively establish and maintain a complete milk supply during their infants' stay in the Children's Hospital of Philadelphia's (CHOP) Newborn/Infant Intensive Care Unit (N/IICU). In addition, we wanted to understand the influence of a prenatal lactation intervention on maternal pumping initiation and milk supply at the time of infant discharge, the impact of the location of infant delivery (at CHOP or at outside hospital) on maternal pumping initiation, and the CDH infants' exposure to human milk during the hospital stay and at discharge from the N/IICU. This study was approved by CHOP Institutional Review Board.
Setting
CHOP is located in Philadelphia, PA. CHOP is a free-standing children's hospital that includes the Center for Fetal Diagnosis and Treatment (CFDT) and the Garbose Family Special Delivery Unit (SDU). The CHOP SDU is the world's first birth facility within a pediatric hospital specifically designed for mothers with prenatally diagnosed birth defects, including CDH. The CFDT is an international referral center for mothers carrying a fetus with a CDH. When a mother makes the decision to transfer care to the CFDT at CHOP, she is cared for by an interdisciplinary team of maternal fetal medicine physicians, surgeons, neonatologists, advanced practice nurses, social work, psychologists, child life specialists, and lactation specialists.
When families transfer care to the CFDT, they are provided with a comprehensive packet of information tailored to their infant's diagnosis and a DVD entitled “The Power of Pumping.” This DVD was developed at CHOP, specifically to address the maternal lactation interventions necessary when maternal infant separation will occur at birth, as well as a plan for transition to direct breastfeeding if that is the mother's goal. The DVD focuses on (1) the science of human milk as a medical intervention, (2) the importance of pumping early and often to establish milk supply, (3), human milk oral care as a medical intervention, (4) skin to skin contact, and (5) transition to direct breastfeeding. All families are given this DVD and asked to watch it before their prenatal lactation consult.
As part of standard care at CHOP, all families have the opportunity to receive a personalized 1:1 prenatal nutrition consult with a PhD Nurse Researcher who is the Director of the Lactation Program at CHOP. The goal of the prenatal consultation was to ensure all families are educated and equipped to make an informed decision regarding infant feeding.15,16 During the prenatal nutrition consultation, the family is provided with evidence of the science of human milk for infants with CDH and specifically how human milk impacts outcomes.7,13,14 The family also received all the supplies they will need for pumping initiation at the time of delivery. These supplies include a sterile pump kit, bottles, labels, dish soap for cleaning their pump pieces, microsteam bag for sanitization of pumping equipment, written instructions, and an education sheet for how family members can support the mother in expressing milk. They are shown how to assemble the pump and use the equipment, and are encouraged to practice assembling the hospital grade breast pump and ask any questions they may have during the process. The family is instructed on the critical nature of early initiation of lactation (to pump within 1 hour of delivery and to pump every 2–3 hours for a goal of eight or more pumping sessions per 24-hour period). The family learns of the critical window of opportunity to establish milk supply and come to a full milk volume. We emphasize for the first 2 weeks the mother's most important job is to eat, sleep, visit her infant, and express milk for her infant. This emphasis on the first 2 weeks gives the mothers the necessary knowledge to pump frequently to establish a full milk supply for their child. The family also learns labeling and storage of milk, cleaning and sanitizing of pump equipment, and starting human milk oral care with the infant as soon as feasible after the infant is born.
The hospital aims to facilitate consultations with all families before delivery; however, some families are not seen because of late prenatal diagnosis, late transfer of care to CHOP's CFDT, preterm delivery of the infant, or rarely, refusal of the family to meet with lactation. After delivery of the infant with CDH, the mother receives lactation care, education, and technical support from all members of the health care team. At the time of the study, CHOP had four international board-certified lactation consultants (IBCLCs) with two IBCLCs being dedicated to the N/IICU. At the time of the study CHOP also had a PhD prepared nurse researcher as director of the lactation program and a PhD prepared clinical supervisor for the program. It is the expectation that all families receive evidence-based lactation education, care, and support during the hospital stay. This is accomplished through a systematic approach to training and education for bedside nurses within the main hospital and a presence of >800 trained Breastfeeding Resource Nurses.17,18 CHOP's lactation-based policies, procedures, and standards are easily accessible 24 hours per day on the hospital's internal website and all are based on the Spatz 10 step model for human milk and breastfeeding in vulnerable infants and the “Transition to Breast Pathway” for surgical infants.15,19,20 The “Transition to Breast Pathway” was evaluated through a continuous quality improvement project that found that mothers of surgical infants (n = 80) can establish a normal milk supply (603 mL/day) and that 100% of eligible infants (58/58) were able to transition to direct (at breast) feedings before discharge. 20
Participants
The participants in the study were infants admitted to CHOP with a diagnosis of CDH. Infants admitted to CHOP N/IICU with a diagnosis of CDH between August 1, 2012 and March 31, 2017 were included; infants who died or were withdrawn from care before initiating enteral feeds were excluded from the study.
Methods
This study is a retrospective descriptive cohort study. The electronic patient health record was used to complete chart reviews to abstract the following elements: demographic data, location of infant delivery, maternal breastfeeding goals (from the prenatal consultation), maternal lactation and pumping data, maternal exposure to lactation support (prenatally and during the infant N/IICU stay), maternal milk supply (documented during inpatient lactation visits), and the infant's daily enteral feeding exposure. All data were entered into a Redcaps database by the study team members. Analyses of categorical variables were completed using descriptive statistics.
Results
A total of 149 infants born with CDH and admitted to the CHOP N/IICU were included in the study. Of them, 126 (84.6%) infants were born in the CHOP SDU with the remaining 23 infants born at outside hospitals and transferred to CHOP N/IICU. The mean day of life of admission to the CHOP N/IICU was 2.03 (median 1, range 0–63). Further demographics are described in Table 1.
Demographics
IQR, interquartile range; SD, standard deviation.
Of 126 mothers, 120 (95%) who delivered their infants at CHOP initiated pumping and 21 of 23 (91%) of mothers who delivered at an outside hospital initiated pumping.
For infants born at CHOP (n = 126), 60.3% (n = 76) had documented prenatal nutritional consultations completed in the electronic health record. The majority of mothers, 86.8% (n = 66), expressed a prenatal intention to initiate lactation and provide human milk for their infants. The remaining 10 mothers (13.2%) reported no intention or undecided intention to initiate lactation.
Among the mothers with a documented prenatal intention to provide human milk for their infants, 100% (n = 66) initiated lactation and the average documented milk supply at the final lactation visit was 716.2 mL/day. Similarly, among the mothers with no intention or undecided intention to initiate lactation, 100% (n = 10) of the mothers initiated lactation. In this group, the average milk supply documented at the final lactation visit was 568.5 mL/day (Fig. 1).
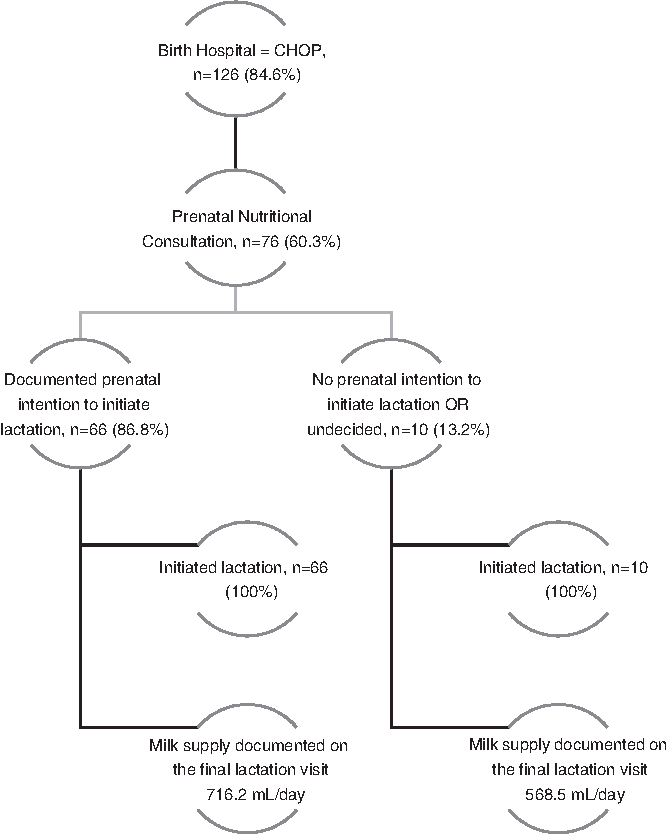
Schematic of maternal lactation experience.
For the overall study sample, 79% (n = 118) were being fed human milk at the time of discharge from the N/IICU. And among those discharged on human milk, 55% (n = 65) were discharged being fed unfortified human milk with 9% (n = 11) being fed unfortified maternal hind milk.
Discussion
A personalized prenatal nutritional consultation intervention influenced those mothers of CDH infants without established lactation goals/intent to both initiate and sustain milk production through the infants' discharge from the N/IICU. This research demonstrates that infants born with CDH are able to receive a predominant human milk diet during the N/IICU stay. Despite a mean length of stay of 69 days (range: 6–343 days), the majority of infants in the study were discharged from the N/IICU on a human milk diet. In addition, the average milk supply of the mothers at the time of discharge was >500 mL/day.
This research dispels common myths that mothers of critically ill infants are not able to achieve a normal milk supply or maintain milk supply through discharge. Mothers in our study were able to provide a 100% milk diet to their infants despite long hospitalizations of their children with one mother having an infant in the NI/ICU for almost 1 full year. Outside the scope of this research, we also know that many of our mothers not only have enough milk for their infants, but many of them donate their excess milk to the milk bank at CHOP.
We also have demonstrated that infants with CDH can receive a predominant human milk diet through discharge. We do this by close monitoring of maternal milk supply and by optimizing the feeding of milk to the infants. Our nurses are all educated on the diurnal variation of milk production and of caloric density of mothers' own milk. For example, our nurses understand that the first milk expression of the day when the breasts are most full is the milk that is lowest in calories, so this milk is routinely frozen and not used to feed the infant. Our nurses and IBCLCs monitor milk production closely and work with the registered dietitians and health care provider team to make decisions regarding optimization of human milk. We often have mothers fractionate their milk to collect higher calorie milk to feed to the infant with CDH.
This research is the first study to document the lactation outcomes of mothers with infants with CDH and the infant feeding outcomes. Future research should examine the experiences of CDH mother–infant dyads at other institutions. It will also be important to examine the long-term impact of a human milk diet on the long-term health outcomes of infants with CDH.
Footnotes
Acknowledgments
The authors gratefully acknowledge the contributions of the study's research assistants from The University of Pennsylvania School of Nursing and CHOP.
Disclosure Statement
The authors report no conflicts of interest related to this research.