
Abstract
Abstract
Introduction:
The aim of this study was to determine the quality of lactation studies investigating antidepressants in breast milk according to the Food and Drug Administration (FDA) draft guidelines and the article by Begg et al., 2002, published in the official journal of the International Lactation Consultant Association (ILCA).
Materials and Methods:
We used PubMed and LactMed® for the literature search. Furthermore, cross references were searched for additional studies.
Results:
A total number of 60 articles were included for review. For selective serotonin reuptake inhibitors and venlafaxine, only two studies correctly assessed the absolute infant dose and milk to plasma ratio; one sertraline and one fluoxetine study. Of all tricyclic antidepressants, one study for amitriptyline and one for nortriptyline assessed these endpoints correctly. We found a lack of information on breast milk sampling methods in many studies. Concentrations needed for the calculations were based on single measurements instead of at least five measurements during one dose interval, and the relative infant dose was not normalized by maternal weight, or an average maternal weight of 70 kg was used as a standard.
Discussion:
We conclude that the quality of the current literature on this topic does not meet the standards of the FDA. Studies of higher quality are needed to determine the extent of drug transfer to breast milk for antidepressants, so an adequate recommendation about use of these drugs during lactation can be given.
Introduction
The percentage of mothers who breastfeed their child has increased the last years up to 75%. 1 Human milk provides essential nutrients for the infant and provides health benefits for both mother and child. Breast milk increases the mother–child bonding, strengthens the immune system and stimulates the gastrointestinal function of the newborn.2,3 Because of these health benefits and the low costs of breastfeeding, the World Health Organization recommends exclusive breastfeeding during the first 6 months of life and up to 2 years as supplement. 4
The prevalence of depression is 10–15% in pregnant women,5–7 5–29% in the postpartum period,8–10 and 2.9–5.5% of nursing mothers use antidepressants.11,12 Reported side effects in the neonate due to possible exposure of antidepressant medication through breast milk are somnolence, lethargy, fever, reduced postnatal growth, and excessive infant crying.13–15 On the contrary, discontinuing antidepressants during breastfeeding, which seems to overcome adverse drug reactions in the suckling infant, may lead to bonding problems, adverse child development, excessive infant crying, and a possible relapse of maternal depression.16,17 Investigating the risks of antidepressant use while breastfeeding is difficult because it is unethical to conduct randomized, placebo-controlled, double-blind trials in pregnant and lactating women treated with antidepressants.
The guidelines of the Food and Drug Administration (FDA) and the European Medicine Agency (EMA), introduced four major elements for risk assessment of using medication during breastfeeding, which consist of the estimated infant dose, the infant plasma concentration, the observed adverse effects of the infant, and the follow-up of breast-fed infants.18,19 This review will focus on the first element, the estimated infant dose. Therefore, we use the article of Begg et al., 20 published in the official journal of the International Lactation Consultant Association (ILCA) and also the FDA guidelines as we did in our previous studies on anticonvulsants, 21 antipsychotics, 22 and antibiotics. 23
To assess the safety of antidepressants, it is of great importance to distinguish between direct pharmacological effects of antidepressants and possible developmental disorders in the suckling infants because of the psychiatric condition of the mother. Therefore, it is highly important to assess the infant dose of antidepressants in breast milk. Both FDA guidelines and the article of Begg state which parameters should be considered when studying the transfer of medication from breast milk to the suckling infant. An important parameter for estimating the risk of the dose of the drug is the absolute infant dose (AID), which is the concentration of the drug multiplied by the volume of milk (150 mL/kg per day). Furthermore, when the AID is known, the relative infant dose (RID) can be determined by dividing the infant dose by the maternal dose. In the literature, a RID of less than 10% is considered generally safe. 20 Another parameter used in the guidelines for lactation is the milk to plasma ratio (M:P ratio), which determines the ratio between drug concentrations in milk and plasma. Because this ratio is not directly related to the infant safety, it is considered less relevant in clinical practice. 24
We searched for lactation studies that reported concentrations of antidepressants in breast milk and checked whether these studies met the criteria of the article of Begg and FDA guidelines on lactation studies. This systematic review provides an overview of which antidepressants need further research.
Materials and Methods
Antidepressants of interest
All registered (in the Netherlands) selective serotonin reuptake inhibitors (SSRIs: fluvoxamine, paroxetine, sertraline, citalopram, escitalopram, and fluoxetine), serotonin-norepinephrine reuptake inhibitors (SNRIs: venlafaxine), and tricyclic antidepressants (TCAs: amitriptyline, clomipramine, dothiepin, imipramine, nortriptyline and doxepin) were taken into consideration for this review.
Inclusion of studies
We used the same inclusion criteria as we reported in our previous studies.21–23 In brief, we used the records of the LactMed® database with an additional PubMed search until November 2018. PubMed was searched additionally using: “Milk, Human” in the MeSH terms or “Breast Milk” or “Human Milk” in the title or abstract combined with the antidepressant of interest in [all] fields. Studies that did not mention breast milk concentrations or any antidepressant of interest or written in languages other than English, German, or Dutch were excluded.
Criteria for quality review
The quality review of all studies was based on the article of Begg et al. and the FDA guideline.18,20 The article and the FDA guideline containing information about guidelines on lactation studies, topics on study design, the amount of drugs in breast milk and determination of kinetics were merged to create a checklist (Table 1). Each original article was checked using this list.
Quality Checklist Based on the Food and Drug Administration Guideline and the Article by Begg et al., 2002
U.S. Department of Health and Human Services: Food and Drug Administration section CP, 2005. 18
Begg et al., 2002. 20
AUC, area under the curve; M:P ratio, milk to plasma ratio.
Results
A total number of 60 articles were included for review (Figure 1). We found 52 studies using the LactMed database, and added eight studies using PubMed. The results have been presented in Tables 2 and 3 for SSRIs and TCAs.
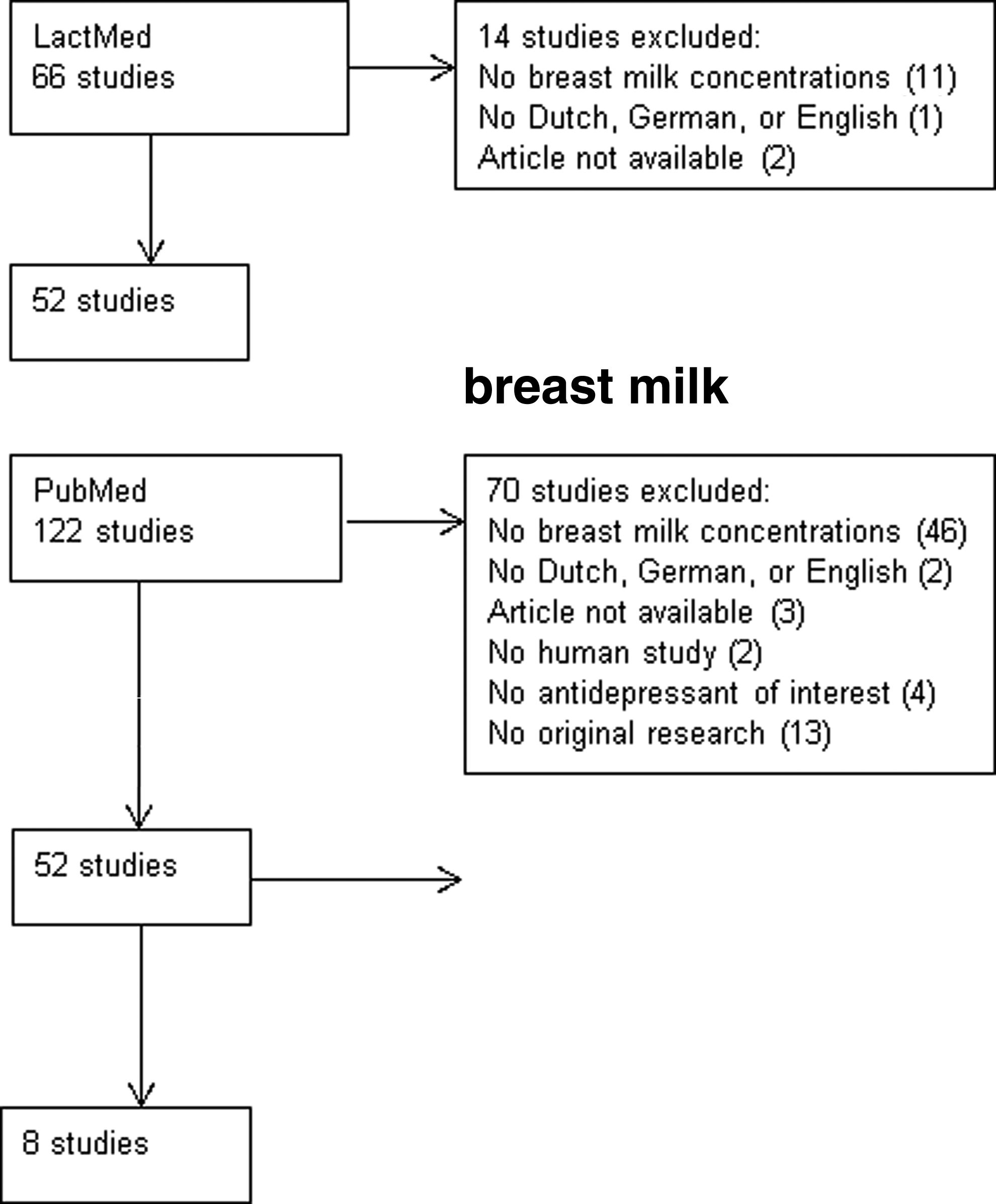
Results of study inclusion using LactMed® and PubMed.
Results of Quality Review for the Selective Serotonin Reuptake Inhibitor/Serotonin-Norepinephrine Reuptake Inhibitor
All numbers represent the number of articles that matches the corresponding criteria in Table 1.
AID, absolute infant dose; N/A, not applicable; SNRI, serotonin-norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor.
Results of Quality Review for the Tricyclic Antidepressants
All numbers represent the number of articles that matches corresponding criterion in Table 1.
AID, absolute infant dose.
For SSRIs and venlafaxine, only two studies correctly assessed the AID and M:P ratio; one sertraline and one fluoxetine study.25,26 Of all studies on TCAs, only one study for amitriptyline and one for nortriptyline assessed the endpoints correctly.27,28
Discussion
Our review found that of the 60 included studies, only four studies had both correctly assessed the M:P and AID, two studies for the SSRIs and SNRIs and two for the TCAs. For 10 studies, one of the two endpoints was correctly assessed, either the M:P or the AID. Despite the fact that TCAs are on the market for a long time compared to SSRIs and venlafaxine, the number of studies published on this class of drugs is very low compared to SSRIs and venlafaxine. An explanation could be that information of drug transfer to breast milk became of more importance after these drugs were no longer extensively used. Most studies on TCAs were published before the year 2000, before the article of Begg and the FDA guideline became available.
Most studies were published as a case report or a letter to the editor. The quality criteria could not be determined due to the brief character of these reports. The low number of patients in most studies makes it doubtful whether these studies represent lactating women as a whole. However, neither guideline sets a minimum of patients included. This means that interindividual variations may act as possible confounding factors in interpreting those studies, such as pharmacogenomics, 83 age, weight, and race. Therefore, the guidelines should mention a set of possible confounders which should be properly addressed in lactation studies.
Many studies do not state the method of breast milk collection. It is therefore not clear whether foremilk, hind milk, or both were used, as we know that hind milk has higher lipid content than foremilk, resulting in a higher concentration of lipophilic drugs at the end of breastfeeding. 84 Studies that analyzed pre- and postfeed samples separately showed that the drug concentrations of paroxetine and dothiepin were two times as high in hind milk compared with foremilk samples.40,76 For other antidepressants, we assume that this also may be the case, which underline that sampling time is of importance in performing lactation studies.
Longitudinal data are important to minimize intraindividual variations, because the composition (pH, lipid concentration) of breast milk changes over time, which may influence the extent of drug transfer into breast milk. 85 Ideally samples should be taken over time; however, it is hard to motivate breastfeeding women for such studies.
Another point in interpreting lactation studies is the analytical assay for drug measurements. Reporting concentrations without knowing the limit of quantification of the assay or variations of the assay over time are of less value, especially when low concentrations are to be expected in infant's plasma or breast milk.
For imipramine, fluvoxamine, and fluoxetine more than half of the studies used a nonvalidated assay, or the necessary validation parameters were not presented. Validation is necessary to prove at least reproducibility, which makes those studies harder to interpret.
Almost none of the studies for the TCAs—except one study for both nortriptyline and amitriptyline—used multiple breast milk and plasma levels to determine the M:P ratio.27,28 In these studies, single paired milk and plasma concentrations were used to calculate the M:P ratio. However, studies have shown that the M:P ratio can vary over a two- to threefold range at different time points.39,46,86 To avoid this problem, the article of Begg recommends measuring the M:P ratio using the area under the curve of the maternal plasma and milk concentration time curves. Without multiple breast milk levels, the AID cannot be determined correctly. The article of Begg states that the AID needs to be calculated with an average milk concentration of at least five levels or with the concentration of the total milk collection in 24 hours.
Dose regimen is not reported in 27 of the 60 included studies, which makes it impossible to calculate the RID.
Most studies measured infant plasma concentrations, which quantifies the absolute exposure of the antidepressants in the suckling infant and is, beside the infant dose, another major element in the risk assessment according to the EMA. 19 Although this review only includes studies in which breast milk concentrations were measured, studies with infant serum concentrations but without measuring breast milk concentration were also found.87–96
For the SSRIs and SNRIs, infant serum concentrations are published for fluvoxamine, paroxetine, sertraline, fluoxetine, and venlafaxine. For the TCAs, infant studies are published for amitriptyline, clomipramine, imipramine, and nortriptyline. In all studies a single plasma concentration was determined.
Sertraline and nortriptyline each has four studies that reported serum concentrations, resulting in a total of 84 patients for sertraline and 63 patients for nortriptyline.
In 8 out of the 10 infant studies, the dosage of the mother was reported, in the studies of Mammen et al. and Wisner et al.92,94 The maternal dosage was not specified. It is difficult to interpret the reported infant serum concentrations without knowing the ingested infant dosage. Therefore, measuring infant serum concentrations should be accompanied by measuring breast milk concentrations. The results of these infant studies are nevertheless useful, because most studies include large number of patients, and it is therefore easier to detect possible adverse effects.
Conclusion
The FDA guideline states that the AID is one of the major elements for a risk assessment of using antidepressants during breastfeeding. Quantitative studies that assess the AID or M:P correctly are of clinical importance to relate possible side effects in the suckling infant to the concentration of drugs in breast milk. We showed that most lactation studies with antidepressants did not provide an AID or M:P assessed according to the article of Begg and FDA guidelines, especially for the older TCAs.
We conclude that the quality of the current literature about this topic does not meet the standards of these guidelines. Studies of higher quality are needed to determine the extent of drug transfer to breast milk or M:P ratio for antidepressants, so adequate recommendation about use of these drugs during lactation can be given.
Footnotes
Authors’ Contributions
D.B.-B., D.H.M., and P.G.J.H. designed the review and wrote the article. All authors contributed to and have approved the final article.
Disclosure Statement
No competing financial interests exist.