
Abstract
Abstract
Objective:
Breastfeeding can be challenging for new mothers. Women with high breastfeeding self-efficacy are more likely to breastfeed with confidence and are more likely to succeed in breastfeeding. The aim of this prospective longitudinal study was to test whether breastfeeding self-efficacy and breastfeeding experiences were related to trajectories of self-efficacy in the parenting domain during the transition to parenthood.
Materials and Methods:
A group of 1,091 primiparous women completed questionnaires at 32 weeks of gestation (maternal self-efficacy) and 3 months after giving birth (maternal self-efficacy, breastfeeding self-efficacy, and breastfeeding experiences). Only the women who started breastfeeding and completed questionnaires at both time points were included in the analyses (N = 817).
Results:
High breastfeeding self-efficacy significantly predicted increased maternal self-efficacy through the transition to parenthood. A successful breastfeeding experience fully explained this effect.
Conclusion:
The mediating effect of positive breastfeeding experiences on the relationship of breastfeeding self-efficacy and the change of maternal self-efficacy during the transition to parenthood implies breastfeeding to be an early target to enhance maternal self-efficacy. By pointing out breastfeeding as a genuine challenge during prenatal maternity courses, it might prepare mothers for one of their first experiences of parenthood. As a result, successful breastfeeding could be a steppingstone from positive prenatal expectations to growing confidence as a parent.
Introduction
Breastfeeding is one of the first skills many new mothers try to master. 1 The World Health Organization promotes breast milk as the best source of nourishment for infants. Exclusive breastfeeding is recommended up to 6 months of age, 2 but worldwide only 40% of children under this age are exclusively breastfed. 3 Negative breastfeeding experiences (e.g., pain, problems with latch) may undermine a mother's wish to breastfeed, and force some mothers to stop breastfeeding earlier than desired (e.g., ref. 4 ). Longitudinal studies have shown that breastfeeding self-efficacy, or mothers' beliefs regarding their ability to breastfeed, is one of the most important predictors of prolonged exclusive breastfeeding (e.g., ref. 5 ). Successful breastfeeding further strengthens breastfeeding self-efficacy 5 and has an impact on maternal wellbeing 6 ; the success of breastfeeding may also contribute to a positive general sense of maternal self-efficacy.
Maternal self-efficacy refers to the expectations mothers hold about their ability to parent successfully. The concept of self-efficacy is derived from Bandura who stated that efficacy expectations are influenced by several sources of information, of which personal performance accomplishment is the most important one. 7 Successful experiences support higher efficacy, whereas failures may lower self-efficacy. In contrast to people with high self-efficacy, who are more likely to face challenges positively, people with low self-efficacy tend to avoid difficult situations or give up easily. 7 Moreover, Bandura asserted that enhanced self-efficacy in one domain generalizes self-efficacy in other domains. Because breastfeeding is one of the first experiences in parenthood, it deserves attention as a potential source of maternal self-efficacy that can be observed among most new mothers. 8
Maternal self-efficacy is an important predictor of a wide range of maternal outcomes, including parental competence and sensitivity, 9 as well as child outcomes, including child behavior and socio-emotional functioning (e.g., ref. 10 ). Already before childbirth, first-time mothers imagine themselves as parents and develop expectations of their competence and effectiveness as a parent. 8 Previous studies have shown that higher maternal self-efficacy is predicted by higher prenatal self-efficacy expectations 11 as well as positive early experiences, such as a positive childbirth experience. 12 In addition, positive breastfeeding experiences were found to be associated with breastfeeding self-efficacy. 5 Although breastfeeding support guidelines recommend strengthening self-efficacy to support and foster breastfeeding, 13 it has not been studied previously how breastfeeding experiences and breastfeeding self-efficacy are related to self-efficacy in the parenting domain.
The aim of this study was to test whether breastfeeding self-efficacy and breastfeeding experiences were related to trajectories of maternal self-efficacy during the transition to parenthood. It was hypothesized that high breastfeeding self-efficacy would predict increased maternal self-efficacy across the transition of parenthood. Additionally, because women with higher breastfeeding self-efficacy would be more likely to overcome difficulties with breastfeeding, it was hypothesized that a positive breastfeeding experience (mastery experiences) mediated the link between breastfeeding self-efficacy and increased maternal self-efficacy.
Materials and Methods
Design
The present prospective longitudinal study was approved by the Medical Ethics Committee of the VU University Medical Center, Amsterdam, The Netherlands (#2008/196).
Setting
Participants were recruited between 2009 and 2012 as part of the Generations 2 study, an ongoing longitudinal study in first-time mothers on the development of parenting and mental health with measurements from early pregnancy into middle childhood. Women were mainly recruited through midwifery practices in the vicinity of Amsterdam.
Sample
Participants were 1,091 primiparous women. Of these women, 931 (85.3%) started breastfeeding. Because of additional challenges that may influence the variables under study (breastfeeding experiences and the change of maternal self-efficacy), women who were expecting twins were excluded from the present study. Due to missing data or too late submitted questionnaires, participants were excluded. Finally, 813 respondents were included in the study group. Supplementary Figure S1 gives an overview of the inclusion.
The study group did not differ from women with incomplete data on age, marital status, education, and ethnic background. Women who started breastfeeding (the study group) did not differ from the women who never breastfed (excluded in the present study) on ethnic background and marital status. However, the two groups differed in age (p < 0.001) and education (p < 0.001). Women who initiated breastfeeding were older and had a higher education level than those who did not start breastfeeding. The characteristics of the study group are presented in Table 1. This table also presents the characteristics and the differences between the women who stopped breastfeeding and those who were still breastfeeding 3 months after childbirth.
Sample Characteristics
Ethnicity is defined by the Statistics Netherlands (CBS): Non-Western immigrants are individuals originating from Africa, Latin America, Asia (Indonesia and Japan excluded), or Turkey. Western immigrants are individuals originating from Europe (Turkey excluded), North America, Oceania, Indonesia, and Japan.
CBS, Centraal Bureau voor de Statistiek; NS, not significant; SD, standard deviation.
Measurements
Maternal self-efficacy was measured when women were 32 weeks pregnant and 3 months after birth, respectively, using the prenatal and postnatal version of the Maternal Self-Efficacy in the Nurturing Role Questionnaire (SENR). 14 The SENR contains 16 items rated on seven-point Likert-type scales assessing the mothers' perception of their competence as a parent (e.g., “I expect to be able to soothe my baby easily when he or she is crying or fussing”/“I can soothe my baby easily when he or she is crying or fussing”). The Likert-type scale ranged from 1 = “not at all representative of me” to 7 = “strongly representative of me.” Scores were summed to produce a final score from 16 to 112, with higher scores indicating higher levels of maternal self-efficacy. Porter and Hsu calculated the internal consistency of the prenatal and postnatal assessment of this questionnaire and found Cronbach's alpha coefficients of 0.91 and 0.78, respectively. 15 Cronbach's alpha in the current study was 0.87 for the prenatal version and 0.84 for the postnatal version of the SENR.
Breastfeeding self-efficacy was measured 3 months postpartum using the Breastfeeding Self-Efficacy Scale Short Form (BSES-SF). 16 The BSES-SF presents 14 items rated on a five-point Likert-type scale (e.g., “I can always manage the breastfeeding situation to my satisfaction”). The Likert scale ranged from 1 = “not at all confident” to 5 = “always confident.” Sum scores were calculated with a range from 14 to 70, with higher scores indicating higher levels of breastfeeding self-efficacy. The Cronbach's alpha coefficient of this short form is 0.94 for the original English version. 16 The Cronbach's alpha coefficient for the translated BSES-SF in the current study was 0.95.
Breastfeeding experience was measured 3 months postpartum using questions on the mother's subjective feelings regarding breastfeeding. Seven assumptions were given (Supplementary Table S1), starting with the phrase “I think breastfeeding is…” (e.g., “I think breastfeeding is very difficult”). Each individual item was scored separately on a five-point scale. Scores were summed to produce a range from 7 to 35. Higher levels corresponded to more positive experiences and attitudes to breastfeeding. The Cronbach's alpha coefficient for this questionnaire was 0.80.
Data collection
After receiving written informed consent, questionnaires were sent by mail to pregnant women at 32 weeks of gestation (M = 33 weeks; standard deviation [SD] = 1.32) and 3 months after childbirth (M = 95 days; SD = 13.87). The women were asked to return these questionnaires within 1 week by mail. Reminder calls and emails were sent after 1 week. Participants were excluded if the questionnaire of prenatal measurement was completed after childbirth (n = 1), if the second measurement was completed later than 6 months after childbirth (n = 28), if questionnaires were missing (n = 39), or when >20% items on a questionnaire (n = 26) were unanswered. If individual questionnaires missed <20% items, 17 missing scores were replaced by the mean value of the participant's own remainder item scores on that questionnaire.
Data analysis
The data were analysed using the Statistical Package for the Social Science, version 24. An alpha level of p < 0.05 was used for all analyses. Preliminary analyses were performed to test for associations between demographic characteristics (age of mother, education level, marital status, and ethnicity) and study variables (breastfeeding self-efficacy, breastfeeding experiences, and maternal self-efficacy) with Pearson correlations and one-way analysis of variances. Demographic variables significantly related to independent and dependent variables under study were included as covariates. Furthermore, the mean difference between prenatal and postnatal maternal self-efficacy was analyzed with a paired sample t-test. To test whether the BSES-SF, the postnatal SENR, and breastfeeding experiences are overlapping variables, a principal components analysis was conducted.
A multiple regression analysis was performed to examine whether breastfeeding self-efficacy at 3 months (independent variable) predicted maternal self-efficacy (dependent variable) at 3 months after delivery. To examine the change of maternal self-efficacy during the transition to parenthood, prenatal maternal self-efficacy was included in the first step.
The second research question, which focused on mediation by breastfeeding experience, was tested using the four criteria of Baron and Kenny. 18 (1) The independent variable (breastfeeding self-efficacy) was a significant predictor of the possible mediator (breastfeeding experience), (2) the independent variable was significantly associated with the dependent variable (postnatal maternal self-efficacy), (3) the mediator significantly predicted the dependent variable, (4) when the mediator was included in the model, the association between the predictor and the dependent variable was no longer statistically significant. 18 Multiple regression analyses were performed to examine these four criteria. Covariates were included in each regression analysis in step 1. Because the change in maternal self-efficacy from pregnancy to early parenthood was examined, prenatal maternal self-efficacy was incorporated in the first step as well. Furthermore, the Sobel test statistic was calculated to determine whether the mediation effect was significant.
An overview of the study variables, the time points of measurements, and the analyses are given in Table 2.
Overview of Study Variables, Measurement Time Points, and Analyses
Results
Preliminary analyses
Means and SDs for breastfeeding self-efficacy, breastfeeding experience, prenatal maternal self-efficacy, postnatal maternal self-efficacy, and age as well as the correlations between study variables are also shown in Table 3. Maternal age was significantly associated with maternal self-efficacy at both time points (prenatal: r = −0.11, p < 0.01; postnatal: r = −0.156, p < 0.001). Education was significantly associated with both breastfeeding self-efficacy, the independent variable, [F(3,809) = 2.68, p < 0.05] and postnatal maternal self-efficacy, the dependent variable [F(3,809) = 3.71, p < 0.05]. Ethnicity was associated with breastfeeding self-efficacy [F(2,810) = 4.29, p < 0.05], but not with prenatal [F(2,810) = 2.74, p > 0.05] or postnatal maternal self-efficacy [F(3,809) 0.29, p > 0.10]. Marital status was not associated with the dependent variable [F(3,809) = 0.69, p > 0.05] or the independent variable [F(3,809) = 0.97, p > 0.05]. Maternal age and education were included as covariates in the analyses.
Descriptive Statistics and Correlations Among Breastfeeding Self-Efficacy, Breastfeeding Experience, Prenatal Parenting Self-Efficacy, Postnatal Self-Efficacy, and Age
p < 0.05, **p < 0.001.
MSE, maternal self-efficacy; BFSE, breastfeeding self-efficacy; BF-exp, breastfeeding experience; SD, standard deviation.
The mean difference between prenatal and postnatal maternal self-efficacy, 3.66 (SD = 9.72), was statistically significant [t(812) = 10.74; 95% confidence interval = 2.99–4.33], and indicated that maternal self-efficacy increased through the transition to parenthood.
Factor analysis
To establish whether the SENR, BSES-SF, and breastfeeding experience measured different aspects of self-efficacy and breastfeeding, a factor analysis was performed. A principal axis factor analysis with oblique rotation was performed on the combined set of items from the BSES-SF and SENR (30 items) questionnaires. Sampling adequacy was verified with the Kaiser–Meyer–Olkin (KMO) measure, KMO = 0.93. Six factors had eigenvalues over Kaiser's criterion of 1. The loadings after rotation on these six factors are shown in Supplementary Table S2. Items with a factor loading >0.4 contributed substantially to a specific component. The squaring of loading gives an estimate of the amount of variance in a factor explained for by an item. The items of the SENR clustered (significantly) on separate factors. However, one item of the BSES-SF and two items of the breastfeeding experience questionnaire showed some overlap in factor loadings. Therefore, additional analyses were done to test the study hypotheses without these three overlapping items (see analyses below).
Breastfeeding self-efficacy predicted maternal self-efficacy
Breastfeeding self-efficacy predicted a small but statistically significant portion of change in maternal self-efficacy (R2 = 0.30, ΔR2 = 0.01, p < 0.001). Higher breastfeeding self-efficacy was positively associated with an enhancement in maternal self-efficacy, indicating that women with high breastfeeding self-efficacy showed an increase in maternal self-efficacy (p < 0.01) from the 32nd week of pregnancy to 3 months postpartum.
Breastfeeding experience as a mediator
Positive breastfeeding experience was significantly associated with an increase in maternal self-efficacy (R2 = 0.31, p < 0.001). Regression analysis showed that breastfeeding self-efficacy was significantly associated with both breastfeeding experience (R2 = 0.49, p < 0.001) and maternal self-efficacy (R2 = 0.30, p < 0.001). Therefore, the first three conditions as applied by Baron and Kenny for the mediation hypothesis were met. 18 When breastfeeding experience was added to the model predicting postnatal maternal self-efficacy (step 4 of the mediation model; Table 4) (R2 = 0.31, ΔR2 = 0.01, p < 0.001), breastfeeding self-efficacy was no longer significantly associated with maternal self-efficacy (Fig. 1).
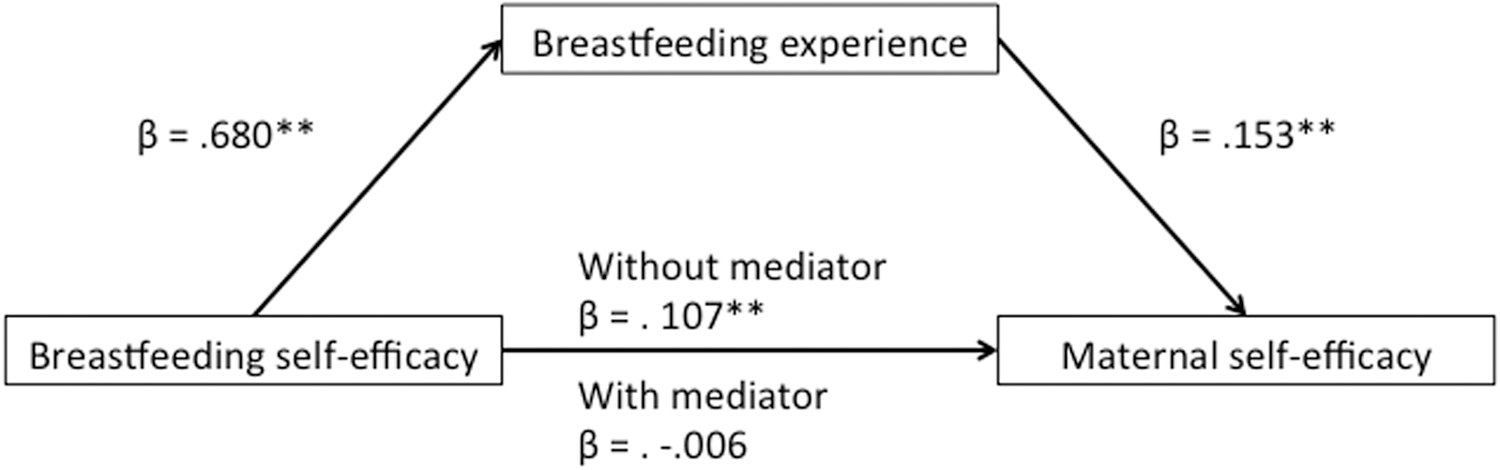
Results of the mediation model. **p < 0.001.
Summary of Multiple Regression Analysis Predicting Postnatal Maternal Self-Efficacy from Breastfeeding Self-Efficacy and Breastfeeding Experience
p < 0.05, **p < 0.001.
The Sobel test showed statistical significance (Sobel test statistic = 5.06, p < 0.001), indicating that the association between breastfeeding self-efficacy and change in maternal self-efficacy in the transition to parenthood was fully mediated by individual differences in breastfeeding experiences. These findings remain the same when the three overlapping items of the BSES-SF and the breastfeeding experience questionnaire were taken out.
Discussion
This study showed that women with high breastfeeding self-efficacy have more positive change in maternal self-efficacy from the prenatal to the postnatal period. In line with previous studies (e.g., ref. 15 ), maternal self-efficacy increased in the transition to parenthood. Furthermore, higher breastfeeding self-efficacy predicted higher maternal self-efficacy through this transition. This result is consistent with one of the principles of the social cognitive theory of Bandura, that is, enhanced efficacy in one domain can enhance efficacy in other related domains. 7 Other experiences related to early parenthood, such as childbirth experience, have been found to be related to maternal self-efficacy,9,12,15 but the finding that breastfeeding self-efficacy predicts changes in maternal self-efficacy is new.
According to self-efficacy theory, the most important factor that influences self-efficacy refers to personal mastery experiences. 7 In the current study, mothers' experience with breastfeeding fully mediated the association between breastfeeding self-efficacy and change in maternal self-efficacy. Thus, high breastfeeding self-efficacy was associated with a more positive breastfeeding experience, which explained why general maternal self-efficacy increased more strongly through the transition to parenthood for mothers who had a higher self-efficacy with regard to breastfeeding.
The results of the preconditions of mediation analysis point out that about 45% of the variance in breastfeeding experience can be explained by breastfeeding self-efficacy. Previous research showed associations between breastfeeding experiences and breastfeeding self-efficacy as well; for example, women who had negative experiences, such as pain, had lower levels of breastfeeding self-efficacy compared with women who did not experience pain during breastfeeding. 19 Because breastfeeding experience and self-efficacy are measured at one time point, bidirectional effects of breastfeeding experience and self-efficacy cannot be excluded. Moreover, these bidirectional associations would be consistent with Bandura's assumption that higher self-efficacy may help people to persevere during challenges and, therefore, increase the chance of success, which may further bolster self-efficacy beliefs. In line with previous studies as well as Bandura's theoretical work, the results of the current study suggest a cascade of breastfeeding experiences affecting breastfeeding self-efficacy, and breastfeeding self-efficacy affecting a woman's experience with breastfeeding.
Because of the correlational nature, the present findings are in need of follow-up studies with an experimental design. As breastfeeding self-efficacy and breastfeeding experience are prone to intervention, 20 the potential interaction between breastfeeding self-efficacy and experiences could, for instance, be a target for parenting courses, especially for women experiencing breastfeeding difficulties, to improve maternal functioning in early parenthood.
Problems in the early phase of breastfeeding are a frequently cited reason to end breastfeeding prematurely (e.g., ref. 1 ), though not all women facing breastfeeding problems stop breastfeeding their child. 21 Possibly, these mothers persist in their desire to breastfeed their child, despite negative experiences. Continuation with breastfeeding after social pressure, in spite of dissatisfaction with feeding practice, has been found to contribute to a less satisfying breastfeeding experience. 22 The current study showed that less positive breastfeeding experiences and attitudes toward breastfeeding may impact women's confidence in parenting in general. So, even though new mothers did as recommended in the best interests of their child, it did not automatically enhance their maternal self-efficacy. By pointing out breastfeeding as a potentially challenging task during prenatal courses, this might not only prepare mothers for these encounters but also prevent them from labeling difficulties as failure experiences, which may reflect not only on their confidence in breastfeeding but also on their own parenting skills in general.
With regard to the measurement of (breastfeeding) self-efficacy and its clinical implications, it is important to note that a cut-off point between low self-efficacy and high self-efficacy does not exist, and may not be as relevant as the change in self-efficacy. Previous experimental work on efficacy beliefs suggests that unrealistic expectations concerning your own capacities as a parent are easy to be undermined in the context of caregiving demands (e.g., ref. 23 ). This is in line with Bandura's theoretical notions on the strength of self-efficacy. 7 It assumes that strong efficacy beliefs may be upheld for a while, even when a person is experiencing failure, while weak efficacy beliefs are easy to extinguish in the context of challenges. Change in self-efficacy beliefs as a response to caregiving demands may, therefore, be a better indicator of the impact of these demands on a parent than the actual level of maternal self-efficacy. Professionals within primary care should be aware of the impact that negative caregiving experiences, such as breastfeeding difficulties, may have on efficacy beliefs and may help women to establish new positive experiences to let them grow their self-efficacy.
It is important to weigh the conclusions against the study limitations. One possible limitation is the overrepresentation of highly educated women in the current sample. Women who initiated breastfeeding were more educated than the excluded women in this study who did not start breastfeeding. Subsequently, women in the current study who were still breastfeeding at the postnatal measurement were more educated compared with those who stopped breastfeeding. These associations between educational level and breastfeeding initiation and duration are in line with previous studies,24,25 suggesting different pathways underlying breastfeeding decisions for women with different educational backgrounds. Future studies should examine whether the findings of the current study concerning the relationship between breastfeeding and maternal self-efficacy can be replicated in lower educated groups of parents.
One might debate that breastfeeding self-efficacy and maternal parenting self-efficacy are overlapping variables. As would be expected, breastfeeding self-efficacy and maternal parenting self-efficacy are indeed slightly related (see correlations). However, the principal components analysis pointed out that the items of these two questionnaires cluster on different components, which indicate that separate self-efficacy constructs may underlie these variables. On the contrary, the principal components analysis did show some overlap between items of breastfeeding self-efficacy and breastfeeding experience questionnaires. However, our analyses without these three overlapping items confirmed the initial findings, indicating that breastfeeding experience fully mediated the association between breastfeeding self-efficacy and change in maternal self-efficacy.
A source of bias in this study might be the lack of a prenatal measurement of breastfeeding self-efficacy. Because the most important predictor of postnatal maternal self-efficacy is prenatal maternal self-efficacy, 15 it could be argued that prenatal breastfeeding self-efficacy is an important predictor of postnatal breastfeeding self-efficacy. The measurement of expectations of one's breastfeeding capabilities can be done using a prenatal breastfeeding self-efficacy questionnaire. 26
Another source of bias might be the absence of measurement of very early breastfeeding experiences in the current study. At 3 months after childbirth, the attitudes concerning breastfeeding might be blurred through succeeding or not succeeding breastfeeding. One might expect that mothers who had problems starting breastfeeding, but nevertheless succeeded, might have more positive memories of their experiences with breastfeeding compared with mothers who did not succeed. Future studies should measure attitudes toward breastfeeding and breastfeeding self-efficacy earlier to test the supposed strengthening effect of mastery experience on maternal self-efficacy. Moreover, further investigation is needed to examine the causality of prediction found in the current study as well as the robustness of the effects in the longer term.
Conclusion
The current study indicated that breastfeeding might impact the general sense of parenting of new mothers. The results suggest that a more positive breastfeeding experience might positively impact women's confidence in parenting in general. This is important because higher maternal self-efficacy is associated with more favorable behavioral and socio-emotional child outcomes. More explicit attention to breastfeeding challenges as well as breastfeeding self-efficacy in primary care support programs 20 for pregnant women and new parents may help boost maternal self-efficacy. In sum, promoting positive breastfeeding experiences might be a steppingstone from positive expectations of motherhood to growing confidence as a new parent.
Footnotes
Acknowledgments
The authors would like to thank Professor Carlo Schuengel for his comments and critical review of the article. M.A.H. is supported by Fonds Nutsohra (project 1001-066). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the article. The funder accepts no responsibility for the contents of the present study.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.