
Abstract

Beyond its nutritional value, human milk is also involved in a complex host–microbe interaction by promoting the colonization of a healthy gut microbiota in the infant. The initial gut microbiome can be influenced by a variety of factors, such as mode of delivery or use of antibiotics. Human milk introduces additional bacterial species and also supplies other components that can influence the composition of the infant gut microbiome. Human milk contains a variety of bacterial species, yet there is low diversity in the infant gut (Fig. 1). High diversity of the infant gut microbiota can increase the risk of dysbiosis, which may lead to poor health outcomes, such as food allergies and obesity. Although it is unclear exactly how the human milk microbiome is established, potential mechanisms include retrograde flow from the infant mouth to the mammary gland during feedings, or active migration of immune cells carrying bacteria from the maternal gut to the mammary gland. 1
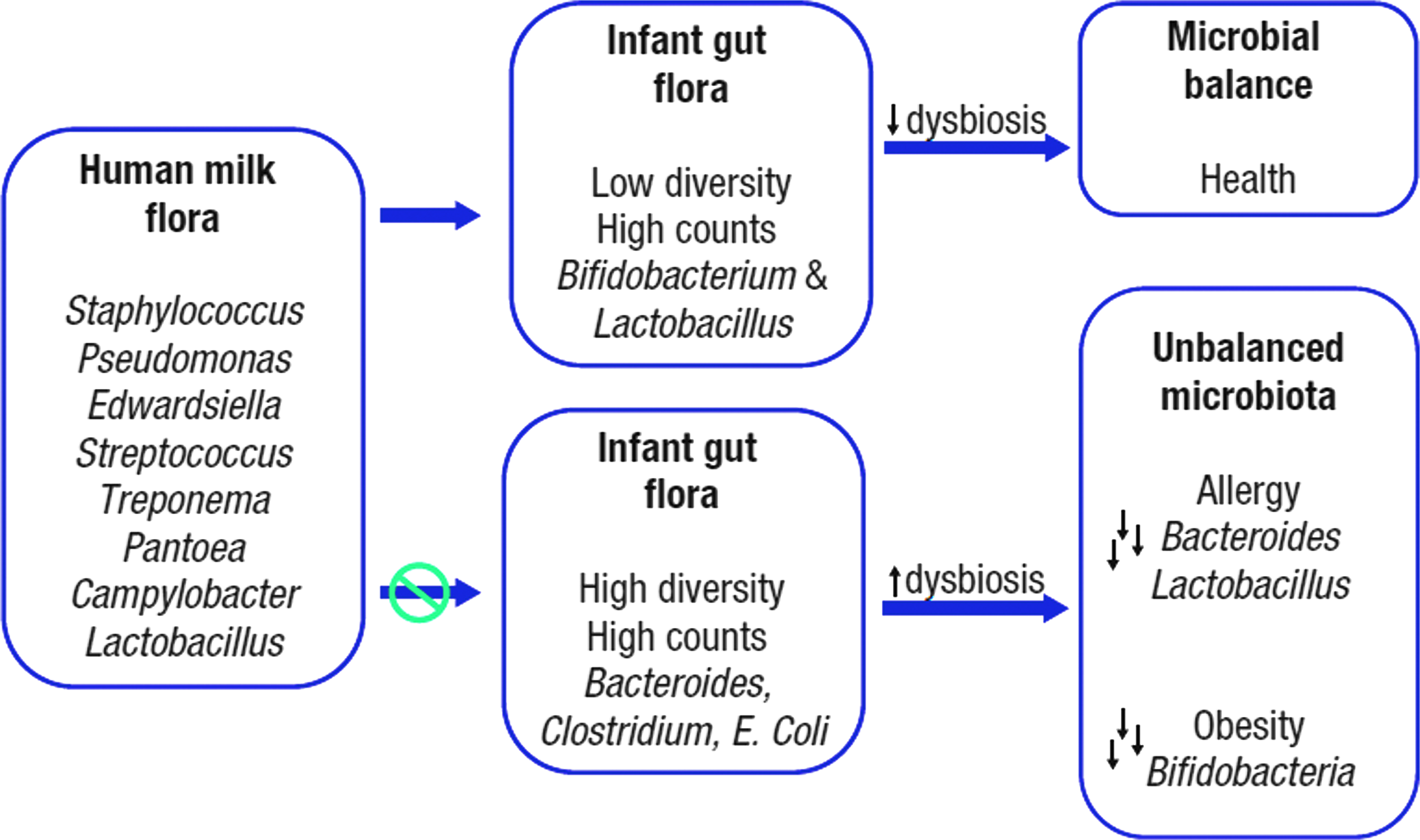
The pediatric microbiome.
Human milk oligosaccharides (HMOs) are a group of complex and diverse sugars found in breast milk. 2 They are the third most abundant component of breast milk, after fat and lactose, yet are not metabolized. Approximately 200 HMO structures have been observed, with composition varying from mother to mother and over the course of lactation. HMOs act as prebiotics to promote the growth of beneficial bacteria in the infant gut and have been proposed to act as antiadhesive antimicrobial agents. 3 Recent studies have shown that HMOs isolated from donor human milk samples demonstrated antimicrobial and antibiofilm activity against different strains of Group B Streptococcus (GBS), a leading cause of neonatal infection.4,5 In these studies, HMOs inhibited the growth of GBS up to 89% and biofilm formation up to 90%. 5 Some HMOs also produced structural alterations in GBS biofilms, resulting in more densely packed biofilms with less prominent nutrient channels (Fig. 2). 4 Growth and biofilm assays in other bacterial species showed that HMOs possessed antibiofilm activity against methicillin-resistant Staphylococcus aureus (up to 60% inhibition) and antimicrobial activity against Acinetobacter baumannii (up to 11% inhibition).4,5

HMOs can alter GBS biofilm structure. 4 GBS, Group B Streptococcus; HMOs, human milk oligosaccharides.
HMOs have also been shown to potentiate antibiotic activity, specifically HMOs targeting the ribosome to inhibit bacterial protein synthesis (aminoglycosides, lincosamides, macrolides, and tetracyclines). 6 However, HMOs did not potentiate the function of antibiotics that inhibit cell wall synthesis (β-lactams and glycopeptides), suggesting that HMOs may help to permeabilize the cell membrane. Furthermore, mechanistic analyses showed that HMOs increased membrane permeability of the GBS strain GB590 to propidium iodide, a membrane-impermeable fluorescent dye that binds to nucleic acids. This work aims to identify which specific HMOs are the most effective antimicrobial agents and to determine their specific cellular targets. A recent study demonstrated that several single sialylated HMOs (e.g., disialyllacto-N-tetraose) possess antimicrobial activity against GBS. 7 Advances in carbohydrate synthesis will enable the synthesis of larger more complex HMOs and the ability to manipulate specific residues. HMOs could potentially be used as novel therapeutics to treat or prevent infectious disease, which is particularly important given the rapid emergence of drug-resistant bacteria.
Footnotes
Disclosure Statement
No competing financial interests exist.