
Abstract
Abstract
Background:
Breastfeeding promotion and support are not universally accepted in the United States as a strategy to reduce infant mortality. We investigated associations between breastfeeding and infant mortality in an urban population with high infant mortality and low breastfeeding rates.
Methods:
A retrospective epidemiologic study linked birth–infant death data for 148,679 live births in Shelby County, Tennessee from January 2004 to December 2014. Births <500 g, deaths ≤7 days, deaths because of congenital anomalies or malignant neoplasms, and records with missing breastfeeding status were excluded. Main outcomes were infant death before the first birthday, neonatal death <28 days, and postneonatal death ≥28 days by ever or never breastfed. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for breastfeeding initiation were adjusted for maternal factors and infant factors.
Results:
Initiation of breastfeeding was associated with a significant reduction in total infant mortality (OR = 0.81, 95% CI = 0.68–0.97, p = 0.023). Neonatal mortality was also significantly reduced with any breastfeeding (OR = 0.49, 95% CI = 0.34–0.72, p = 0.001). Postneonatal mortality was not significantly associated with breastfeeding initiation in the overall population (OR = 0.95, 95% CI = 0.78–1.17, p = 0.65), but was significant in the nonblack population (OR = 0.63, 95% CI = 0.41–0.98, p = 0.039). An association was observed between breastfeeding initiation and infant mortality from infectious disease (OR = 0.49, 95% CI = 0.32–0.77, p = 0.002).
Conclusions:
In an urban area with high infant mortality and low breastfeeding rates, initiation of breastfeeding was significantly associated with reductions in overall infant mortality, neonatal mortality, and infection-related deaths. Breastfeeding promotion, protection, and support should be an integral strategy of infant mortality reduction initiatives.
Introduction
Infant mortality, defined as death before the first birthday, remains a significant health problem for babies born in the United States and around the world. With ∼5.8 infant deaths per 1,000 live births, the United States ranks unfavorably among the world's countries for infant mortality, 1 tallying over 22,000 infant deaths during 2017. 2 Within the United States, the burden of infant mortality is disproportionally greater in many Southern and Midwestern states with mothers characterized by lower income and education, greater poverty, a higher African American population, and low breastfeeding rates.3,4 Racial disparities in infant mortality are well known and documented, and have persisted over the 100 years that data have been collected. 5
Breastfeeding, as the biological norm for infant feeding, can improve infant and maternal health and lower infant mortality. Many risk reductions have been associated with breastfeeding in developed countries around the world, including reduced rates of many infectious diseases and chronic health conditions, and protection against sudden infant death syndrome (SIDS) and necrotizing enterocolitis (NEC). 6 In accordance, breastfeeding is increasingly accepted as an effective global intervention to lower infant and child mortality. 7 WHO estimated that 1.5 million lives younger than age 5 years would be saved if mothers exclusively breastfed for the first 6 months of life, and then continued to breastfeed through age 2 years with complementary foods. 8
A recent meta-analysis comparing optimal breastfeeding rates and infant mortality worldwide found a higher rate of all-cause mortality from 0 to 23 months in infants who were not exclusively breastfed. 9 Compared with exclusively breastfed infants, relative risk for mortality was nearly threefold greater in partially breastfed infants, and 14-fold greater in infants not breastfed. The increased mortality risk extended to age 2 years. 9 Although these studies may not be applicable to the U.S. population because of higher standards of hygiene and control of infectious disease, recent studies of breastfeeding and infant mortality in the United States are sparse. However, in the United States, any breastfeeding has been associated with a reduction in SIDS. 10 A recent meta-analysis in the United States examined duration of breastfeeding and SIDS, and also found a protective effect. 11 Chen and Rogan analyzed a large sample of U.S. infants to calculate the odds of postneonatal death (deaths ≥28 days) for those “ever breastfeeding” and reported an odds ratio (OR) = 0.79 with 95% confidence interval (CI) = 0.67–0.93, compared with never breastfed infants. They also found a duration effect, with postneonatal death OR = 0.62 with 95% CI = 0.46–0.82 for infants with any breastfeeding through 3 months. 12 To date, however, no other studies in the United States have reported analyses of breastfeeding and all-cause infant mortality.
Infant mortality reduction is currently a key focus of public health efforts in the United States, and U.S. Healthy People 2020 goals include the reduction in the rates of neonatal deaths (deaths <28 days) and postneonatal deaths. 13 Infant mortality rates are decreasing in all racial and ethnic groups, 3 although racial differences in infant mortality continue and remain pervasive. 14 Positive results in the reduction of infant mortality have been observed in the United States with targeted interventions including the enhancement of prenatal care programs. 15 Some states and local communities have added the promotion, protection, and support of breastfeeding to their infant mortality reduction initiatives,16–18 but this is not the norm in all communities.
Shelby County, Tennessee, with Memphis as its largest city, is geographically located in the Mississippi Delta region, and has historically had a very high infant mortality rate (12.8 deaths/1,000 live births in 2004 overall and 17.4 deaths/1,000 live births in the black population) 19 that is well above the United States and Tennessee averages, in addition to having a high rate of poverty, a large black population, and very low breastfeeding rates.19–21 Shelby County has a black population of 53.4%, compared with 16.8% in Tennessee and 12.7% in the United States. 21 A black infant in Shelby County, Tennessee is almost three times as likely to die before its first birthday as a white infant. 19 Many initiatives have been developed in Shelby County to address the high infant mortality problem, which together have resulted in an overall reduction in infant mortality over the last several years. Among these initiatives was an intentional and widespread effort to increase breastfeeding rates, especially among African American women. This analysis examined associations between breastfeeding initiation rates and infant mortality in Shelby County for babies born between January 2004 and December 2014.
Methods
Overview
The objective of this epidemiologic analysis was to investigate the associations between breastfeeding initiation and infant mortality, neonatal mortality, and postneonatal mortality in an urban population with high infant mortality and historically low breastfeeding rates. Longitudinal trends have shown decreasing infant mortality rates with increasing breastfeeding initiation rates of the entire population. This retrospective study was performed using a public health database available through the Shelby County Department of Health, analyzing data obtained from birth certificates on live births linked to death certificate data.
Data source
Shelby County receives resident vital statistics including breastfeeding initiation and infant mortality as part of larger birth and death certificate data sets from the Tennessee Department of Health. Longitudinal rates of breastfeeding initiation and infant mortality are collected and reported by the Shelby County Health Department. These data include all births and deaths without exclusions. Information about breastfeeding is collected on the birth certificate with the question “Is the infant being breastfed?” with a “Yes” or “No” response option. 22
Study design
Data from babies born between 2004 and 2014 were analyzed as a linked birth–death cohort study after data cleaning. Deaths were categorized as follows: infant death (defined as death occurring before the first birthday), neonatal death (defined as death <28 days), or postneonatal death (defined as death ≥28 days of life but before the first birthday). Infant mortality was calculated and reported as deaths per 1,000 live births. Infants with birth weight <500 g were excluded from the analysis, as were deaths ≤7 days, and deaths because of congenital anomalies or malignant neoplasms, as deaths in these categories have a substantial impact on overall infant mortality rates and their inclusion might incur reverse causality as previously described. 12 Also excluded were infants without breastfeeding status recorded.
Data analysis
Breastfeeding data were collected from the birth certificate, with a positive result defined as any breastfeeding recorded at hospital discharge. For this analysis, breastfeeding initiation was scored as “Ever” versus “Never” with no information available on the birth certificate regarding breastfeeding duration or exclusivity.
Univariate analyses of maternal and infant factors associated with infant mortality and breastfeeding were conducted. Logistic regression analysis included adjustments for covariates commonly associated with both increased infant mortality and lower breastfeeding rates including maternal factors (race, age, education, Medicaid/ Special Supplemental Nutrition Program for Women, Infants, and Children [WIC] status as a proxy for poverty, marital status, body mass index, smoking during pregnancy, prenatal care, type of delivery, and birth plurality) and infant factors (birthweight, sex, and birth order). Maternal race was self-reported and grouped into the following: black, white, or other (ethnicity was not analyzed). Race, birthweight, and gestational age are strongly related to breastfeeding and infant mortality, and therefore stratified logistic regression analyses were also performed.
Statistics
SAS Version 9.4 (Cary, NC) was used for data analysis including the calculation of mortality rates, OR, and 95% CI. Values of p < 0.05 were considered statisically significant.
IRB oversight
These data are part of an existing public health database analyzed at the Shelby County Department of Health. Per consultation with the Cincinnati Children's Hospital IRB Chair, formal IRB protocol submission and approval were not required because all data were de-identified.
Results
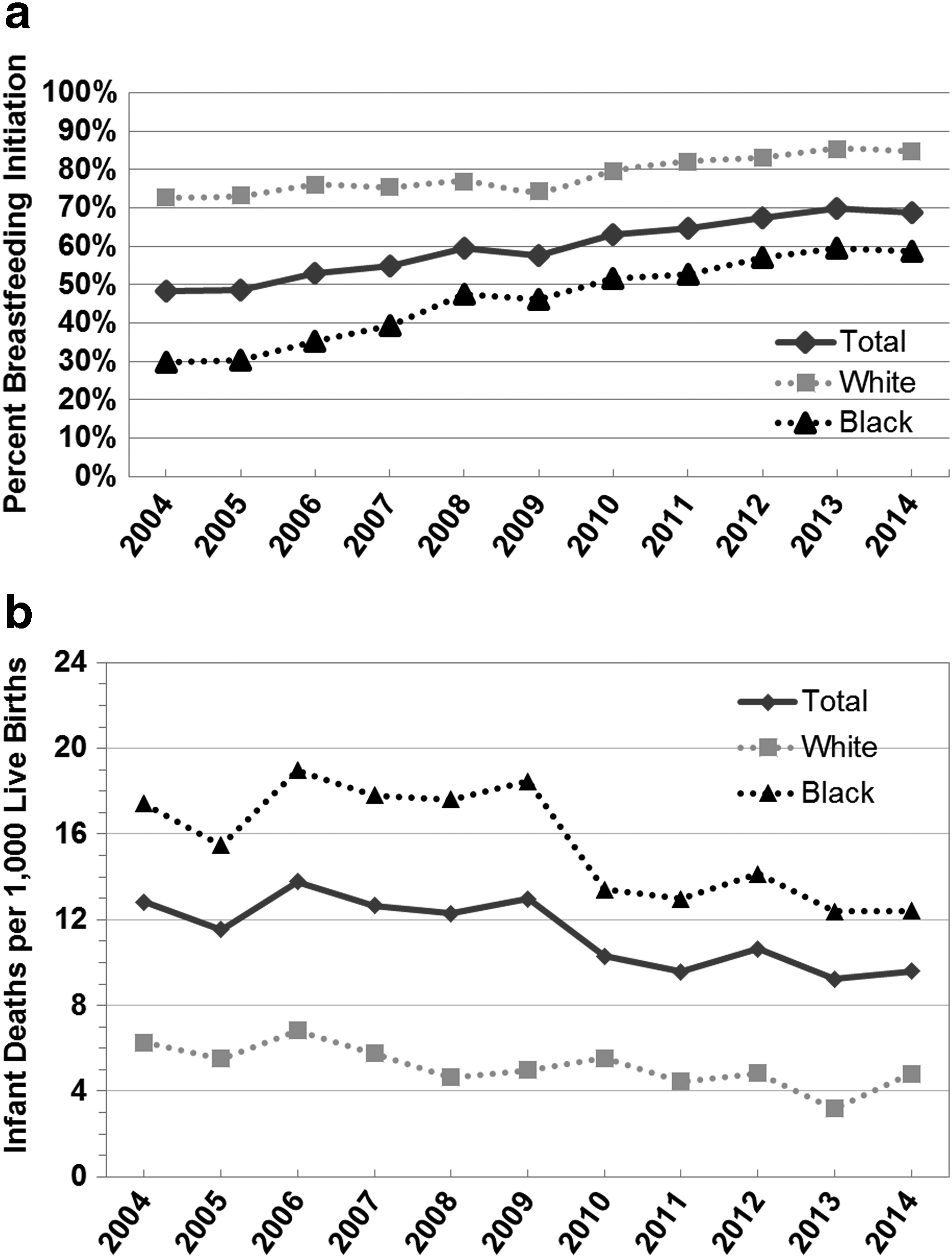
Overall longitudinal breastfeeding initiation rates (ever breastfed) are presented for the entire cohort (without exclusions used in the birth–death linked analysis), as recorded on the birth certificate, rising from 48.5% in 2004 to 68.7% in 2014 (Fig. 1A). The increase was more pronounced in the black population, from 29.9% to 58.6%. During that same interval, overall infant mortality rate in the entire cohort without exclusions, decreased from 12.8 per 1,000 in 2004 to 9.6 in 2014, and this decrease was also more pronounced among blacks, from 17.4 to 12.4 (Fig. 1B). Of note, the black infant mortality rate was still almost three times the white infant mortality rate of 4.8 in 2014. These data prompted the in-depth analysis undertaken here to identify possible associations between breastfeeding and infant mortality.
A total of 157,875 live births occurred in Shelby County during the 11-year time period with 1,762 deaths; after appropriate exclusions a total of 148,679 live births comprised the analysis cohort with 598 deaths (Fig. 2). A majority of the mothers were self-reported as black (59.1%) with the remainder white (37.4%), or other (3.4%). Maternal age was most frequently between 20 and 24 or 25–29 years (56.1%), and most had at least a high school education (73.8%). Most mothers (60.2%) were unmarried and living in poverty (68.6%), based on use of WIC and/or Medicaid status as a proxy. Almost all mothers sought prenatal care (91.8%). Only a small proportion of mothers smoked during the pregnancy (7.2%), but almost half (48.1%) were classified as either overweight or obese, based on their body mass index calculated from self reported prepregnancy height and weight. About one-third of the mothers (33%) had a Cesarean section delivery. Data abstracted for the infants included 12.3% classified as preterm (<37 weeks gestation), 10.6% with low birth weight (<2,500 g), and 7.9% requiring admission to the neonatal intensive care unit (Table 1).

CONSORT Diagram.
Shelby County, Tennessee Birth Cohort from 2004 to 2014
Selected maternal and infant factors were analyzed for total live births, overall infant deaths, neonatal deaths, and postneonatal deaths after exclusions.
WIC, Special Supplemental Nutrition Program for Women, Infants, and Children Supplemental Nutrition Program.
After excluding infant deaths <7 days, infants <500 g, congenital anomalies, and unknown breastfeeding status, there were 598 infant deaths recorded (153 neonatal deaths and 445 postneonatal deaths) for an overall infant mortality rate of 4.0 deaths per 1,000 live births. Within this cohort, the infant mortality rate among black infants was 5.4 per 1,000 births, almost three times the white infant mortality rate of 2.0 per 1,000 births. Univariate analyses of factors associated with infant mortality revealed statistically significant differences in all categories except for infant sex (Table 1). Breastfeeding initiation was recorded in 59.9% of the entire cohort, and statistically significant differences were noted between breastfed and nonbreastfed infants for each characteristic and overall, neonatal, postneonatal infant mortality (Table 2).
Shelby County, Tennessee Birth Cohort from 2004 to 2014 Breastfeeding Data
Selected maternal and infant factors were analyzed for total live births, overall infant deaths, and neonatal deaths, and postneonatal deaths. Breastfeeding n = total number of breastfed babies in each category, and % breastfeeding (of total) in each category. Statistical analysis by Cochran–Mantel–Haenszel method.
Multivariate logistic regression analysis was performed on 89,053 breastfed infants and 59,626 nonbreastfed infants, adjusting for covariates of race, maternal age, maternal education, Medicaid/WIC status, marital status, BMI, smoking during pregnancy, prenatal care, Cesarean delivery, birth plurality, sex, birth order, and birth weight (Table 3). If data were missing for the covariate, the record was excluded, except for BMI and prenatal care, where “Missing” was included as a category because of a high percentage of missing data for these factors. This analysis revealed an adjusted OR = 0.81 (95% CI = 0.68–0.97, p = 0.023) for overall infant mortality in ever breastfed babies. For neonatal mortality, the adjusted OR was 0.49 (95% CI = 0.34–0.72, p < 0.001), and for postneonatal mortality the adjusted OR was 0.95 (95% CI = 0.78–1.17, p = 0.65). In the stratified models, statistically significant race-specific ORs revealed an adjusted OR = 0.58 (95% CI = 0.39–0.87, p = .009) for black neonatal mortality, and OR = 0.52 (95% CI = 0.35–0.76, p < 0.001) for nonblack overall infant mortality, showing a 42% and 48% respective reduction in risk. Nonblack postneonatal mortality was also significant, OR = 0.630 (95% CI = 0.406–0.976, p = 0.039). Additional statistically significant results were noted for <2,500 g overall infant mortality and neonatal mortality and gestation <37 weeks for neonatal mortality.
Logistic Regression Models and Adjusted Odds Ratios with 95% Confidence Interval
All models were adjusted for maternal race (except for race subgroup analysis), maternal age, maternal education, poverty indicator, marital status, maternal BMI, smoking during pregnancy, prenatal care, type of delivery, birth plurality, birth order, sex, and birth weight <2,500 g (except for birth weight subgroup analysis).
p < 0.05.
Results not available because of small numbers and questionable validity of the model fit.
Causes of death in the analysis cohort were grouped as follows: infections, injuries, SIDS, NEC, and “other” (including circulatory, short gestation, and other causes), and by breastfeeding status (Supplementary Table S1). Statistically significant adjusted OR for overall infant mortality in infection causes of death revealed an adjusted OR = 0.49 (95% CI = 0.32–0.76, p = 0.014). Infectious etiologies coded on the death certificate identified the following organisms: Staphylococcus species; Streptococcus species; Klebsiella, Pseudomonas, and Escherichia coli species; cytomegalovirus; herpes; Candida; “viral”; Meningococcal species; “Whooping Cough”; and unspecified.
Discussion
Breastfeeding is the optimal source of nutrition and immune protection for babies, and a robust source of primary prevention for many infant and maternal conditions. 6 The American Academy of Pediatrics strongly states that infant feeding should no longer be considered a lifestyle choice, but rather a public health imperative because of the many short and long-term benefits to mother and child. 23
It is not surprising that infant mortality would be decreased when more mothers breastfeed. A recent Lancet series on breastfeeding estimated that 823,000 lives younger than 2 years would be saved if breastfeeding was “scaled up” to near universal levels, and highlights that deaths in high-income countries may also be prevented with increased breastfeeding, citing meta-analyses examining breastfeeding and SIDS and NEC.6,24,25 However, in the United States, breastfeeding promotion, protection, and support are not always considered a key strategy for infant mortality reduction, despite the 20% reduction in U.S. postneonatal mortality previously reported. 12
The population in Shelby County, Tennessee, with high infant mortality rates and low breastfeeding rates, provided the unique opportunity to examine the correlations between reduction in infant mortality along with the increase of breastfeeding initiation rates. Our results add to the medical literature about the importance of breastfeeding promotion as a critical infant mortality reduction strategy in the United States.
The increased breastfeeding initiation rates observed over this 11-year period reflect a strong and intentional effort by local, state, and national advocacy groups. Efforts by the Shelby County Breastfeeding Coalition,26–28 the Shelby County Health Department, Tennessee Breastfeeding Coalition, the statewide quality improvement collaborative TIPQC (Tennessee Initiative for Perinatal Care), 29 the Tennessee Department of Health, and many national breastfeeding initiatives30–34 have strongly promoted breastfeeding.
In the most recent Centers for Disease Control and Prevention (CDC) Breastfeeding Report Card, reporting on babies born in 2015, 83.2% of U.S. babies initiate any breastfeeding, 4 reaching the Healthy People 2020 goals of 81.9%, 35 compared with 73.1% in 2004; in Tennessee, initiation rates are now reaching 75.7%, increase from 66.1% in 2004. 36 However, the Shelby County, Tennessee rates for any breastfeeding have lagged behind both the U.S. and the Tennessee rates, with only 48.5% initiation of any breastfeeding in 2004 (the first year the birth certificate breastfeeding data were collected) to 68.7% in the 2014 birth cohort included in this study. 20 In areas of low breastfeeding like Shelby County, there is an even greater opportunity for improvement; hence a possible greater public health return on investment for breastfeeding promotion and support activities.
In association with these increased breastfeeding rates, infant mortality rates decreased markedly over this same time period. The Shelby County urban safety net hospital, which cares for many vulnerable neonates also boasted an increase in breast milk feeding of very low birth weight babies from a low of 22% to up to 88% of babies receiving some human milk. 37 This contribution of human milk to the most vulnerable of babies at risk for NEC and sepsis cannot be overlooked in the overall improvements in infant mortality that occurred during this time interval.
The main limitation of our study was that breastfeeding data only documented the initiation of any breastfeeding, and no duration or exclusivity data were available. It is possible that babies analyzed as “ever breastfed” could have only nursed briefly in the birth hospital, but this would actually negatively affect the magnitude of the associations noted in this study. Pregnancy Risk Assessment and Monitoring System (PRAMS) and CDC National Immunization Survey (NIS) data indicate that duration and exclusivity of breastfeeding is decreased among black mothers in Tennessee (exclusive breastfeeding <8 weeks = 60.1% non-Hispanic (NH) black and 53.5% NH white; overall breastfeeding <8 weeks = 45.6% NH black and 34.3% NH white 38 ; exclusive breastfeeding at 6 months = 6.8% NH black and 13.2% NH white; any breastfeeding at 1 year = 12.9% NH black and 17.9% NH white). 36 Although this exclusivity and duration data are not available at the county level, one could use Tennessee data as a proxy. Using Tennessee NIS breastfeeding data (2009–2011) 36 and the distribution of births in Shelby County by race and ethnicity, 20 we estimate Shelby County breastfeeding rates to be lower than the rest of the state: ever breastfed would be 60.2% (compared with 67.8% in TN), breastfeeding at 6 months 31.5% (compared with 36.9% in TN), breastfeeding at 12 months 16.2% (compared with 19.5% in TN); exclusive breastfeeding at 3 months would be 23.8% (compared with 31.9% in TN), and exclusive breastfeeding at 6 months 9.3% (compared with 12.2% in TN). However, these data are estimates at the aggregate level and may not be applicable to individual exposure and therefore are insufficient to draw conclusions regarding duration and exclusivity in relation to infant deaths.
The importance of breastfeeding across the first year of life for risk reduction of infant death highlights the need to acknowledge even short durations of any breastfeeding, especially among the black population, where disparities persist and impact adverse health outcomes.39,40 Bartick et al. reported OR = 0.27 for SIDS with exclusive breastfeeding in the month before death, and an OR = 0.29 for any breastfeeding in the month before death. Similarly, they reported OR = 0.72 for NEC with partial breastfeeding before 36 weeks gestation, and OR = 0.083 for exclusive breastfeeding before 36 weeks gestation. 40 Large population studies of the impact of breastfeeding initiation, duration, and exclusivity on infant mortality are urgently needed in the United States.
It is possible that the prevalence of premature babies affected the rates of infant mortality in the study because of reverse causality, that is, these babies were too sick to breastfeed or receive human milk. However, based on the logistic regression analysis that included weight <2,500 g as a covariate, the protective effect of breastfeeding initiation remained (Table 3). With increased breastfeeding rates of more at-risk infants, the salutary effects of breastfeeding could also be blunted because of other factors (such as racism, poverty, stress, or violence). Finally, the sample size after exclusions may have been too small to detect statistically significant differences in postneonatal mortality, although our OR values correlate with previously published work. 12
In summary, in Shelby County, Tennessee, an area of extremely high infant mortality and low breastfeeding rates, the promotion and support of breastfeeding was accompanied by not only increased breastfeeding rates, but also decreased infant mortality, especially in the African American population where the largest disparities exist. Communities and policymakers in the United States should include promotion and support of breastfeeding in efforts to reduce infant mortality, especially in populations least likely to breastfeed. Breastfeeding education should be required of all providers, especially those who interact with vulnerable populations at risk for infant mortality. When evaluating infant mortality statistics, “not breastfeeding” should be included as a risk factor; when documenting and studying infant death and morbidity, infant feeding assessment should always be included in the data collection and analysis.
Footnotes
Acknowledgments
The authors thank the Shelby County Breastfeeding Coalition (SCBC), the Shelby County Health Department, the many Shelby County community partners working on improving child health, and David Sweat, Administrator, Bureau of Epidemiology and Infectious Diseases, Shelby Country Health Department.
Disclosure Statement
Data were accessed from the Tennessee Department of Health (TDH), Office of Policy, Planning and Assessment, Division of Health Statistics, Birth and Death Certificate Data for Shelby County Residents, 2004–2014 and Linked Birth to Infant Death Certificate Data for Shelby County Residents, 2004–2014. Figures and data analyses were prepared by Shelby County Health Department Office of Epidemiology and Infectious Diseases. Use of these data does not imply TDH agrees or disagrees with any presentations, analyses, interpretations or conclusions herein.
The authors have no financial relationships relative to this article to disclose. Dr. Morrow has a research grant from Abbott Health and Nutrition Institute, and is on scientific advisory boards of Biostime Institute, FrieslandCampina, and Glycosyn.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.