
Abstract
Abstract
Background:
Responsive feeding promotes optimal feeding patterns and growth trajectories. Breastfeeding is thought to facilitate responsive feeding, but research to date has been limited to comparing formula-feeding and breastfeeding dyads. Using a within-subject approach, we aimed to assess maternal responsiveness to infant cues during two human milk feeding sessions differing by feeding modality (breastfeeding versus bottle feeding).
Materials and Methods:
Nine mother–infant dyads (infants ≤6 months) were recruited from the Halifax Regional Municipality, Nova Scotia, from April to May 2018. Two human milk-feeding sessions, directly from the breast and from a bottle, were video-recorded in participants' homes, then scored using the validated Nursing Child Assessment Satellite Training (NCAST) Caregiver/Parent-Child Interaction Feeding Scale. The second half of feeding sessions were coded for infant satiation cues.
Results:
All women earned a college degree or higher, and were partnered. Mothers were aged mean ± standard deviation 33.2 ± 4.0 years; infants were 14.6 ± 6.9 weeks old and six (67%) were female. Mothers were more sensitive to infant cues during breastfeeding (NCAST Maternal Sensitivity to Cues sub-scale score, 15.0 ± 1.0) than bottle feeding (13.4 ± 1.6; p = 0.016). There was a significantly longer latency from feeding session midpoint to the first satiation cue during breastfeeding (minutes:seconds; 3:00 ± 1:53 versus 0:45 ± 1:18 bottle feeding, p = 0.038). There was no difference in the number of infant cues by feeding modality.
Conclusions:
Despite the small sample with high socioeconomic status, this pilot study highlights differences in maternal responsiveness to infant cues by feeding modality with human milk, which warrants further investigation.
Introduction
Mothers' responsiveness to infant feeding cues is integral to infants' developing capacities to self-regulate intake in response to internal hunger and fullness cues.1,2 In contrast, nonresponsive feeding, typically characterized by caregivers' use of controlling or pressuring feeding practices, may override these cues and lead to eating behaviors indicative of poor self-regulation, such as eating in the absence of hunger.3,4
Breastfeeding may facilitate responsive feeding, 5 in part because without visual cues to assess the volume of milk consumed, mothers must learn to trust their infants' abilities to self-regulate intake (e.g., Ref. 6 ). This mechanism has been corroborated by a recent experimental study wherein mothers were significantly more responsive to infant feeding cues when using opaque weight-counter-balanced bottles compared with conventional clear bottles.7,8 Breastfeeding is also associated with stronger dyadic communication: breastfeeding dyads have been shown to have more mutual gaze and touch than bottle-feeding dyads, 9 which may be attributed to shorter feeding lengths during bottle feeding limiting opportunity for social exchange.9,10 However, most responsive feeding research is observational, 5 and other potentially influential factors, such as mothers' personalities predisposing them to different feeding modalities, cannot be discounted. 11
Infants' cues also play a key role, as mothers rely on the type and intensity of these cues to respond responsively. 12 A recent analysis indicated that breastfeeding infants exhibited more cues, as well as different signaling patterns, compared with their formula-feeding peers. 13 However, it remains unclear whether an infant who is fed both from the breast and bottle would alter communication by feeding modality.
To date, responsive feeding research has been limited to comparing groups of mother–infant dyads who are breastfeeding human milk versus bottle-feeding formula. A limitation to this between-subject approach is the known sociodemographic differences between these groups. 14 At the same time, expressing human milk is becoming more commonplace due to advances in electronic breast pumps, stigma related to public breastfeeding, and other caregivers' desires to participate in infant feeding.15–17 Feeding expressed human milk has long been equated with breastfeeding 18 ; however, this assumption is being challenged, with recent evidence suggesting that bottle feeding may lead to overfeeding, regardless of whether formula or expressed human milk is in the bottle. 19 For example, compared with infants fed directly from the breast, infants who exclusively consumed human milk from a bottle gained mean (95% confidence interval) 89 g (13, 164 g) more each month. 20 Overfeeding during bottle feeding may have long-term implications such as poor self-regulation of intake later in childhood. 3
The objective of this study was to employ a within-subject design to assess potential differences in maternal responsiveness to infant feeding cues by feeding modality (i.e., breastfeeding versus bottle feeding human milk). Given that infant cues may differ by feeding modality, and satiation cues are more difficult for mothers to recognize than hunger cues,21,22 this study also aimed to quantify infant satiation cues by feeding modality.
Materials and Methods
Study design
This was an exploratory cross-sectional proof-of-concept (pilot) study in which human milk feeding sessions, one breastfeeding and one bottle feeding, were video-recoded for behavioral analysis. We recruited 10 mothers and their infants aged ≤6 months through posters on local parenting Facebook groups. Eligibility criteria included mothers ≥19 years who routinely fed their infants human milk both from breast and bottle, and for pragmatic reasons, who resided in the Halifax Regional Municipality, Nova Scotia, Canada. Data from one dyad were excluded due to excessive infant fussiness and crying during the second feeding session, and inability to reschedule a session within 5 days of first session. The Mount Saint Vincent University Research Ethics Board approved this study (2017-124).
Data collection
Feeding sessions were recorded in the Halifax Regional Municipality between April and May 2018. Two feeding sessions were video-recorded in each participant's home using three tripod-mounted cameras (GoPro Hero 5), one focused on the mother's face, the second on the infant's face, and the third 1 to 2 m in front of the dyad. The two feeding sessions were captured within 48 hours, at the same time of day, except for one dyad (within 96 hours due to sick infant).
Demographic data were collected using an interviewer-administered questionnaire. Feeding sessions were scored using the validated Nursing Child Assessment Satellite Training (NCAST) Caregiver/Parent-Child Interaction Feeding Scale, a 76-item checklist-based coding scheme that provides a measure of the quality of the feeding interaction using six dimensions (subscales; Table 1). 23 We also conducted frame-by-frame analysis of videos using behavioral coding software (ObserverXT v.14; Noldus Information Technology, Netherlands) to code infant satiation cues derived from the literature.13,23–25 The following cues were selected based on age-appropriateness and their ability to be operationalized: becomes distracted or playful, bites/chews nipple, displays a negative facial expression, gags/coughs/chokes, leans back or arches away, turns head/body away from nipple, spits up milk, detaches from/spits out nipple, cries, and closes eyes. We measured the latency between the feeding session midpoint and the first satiation cue, and between the last cue to feeding termination. We also coded the duration of the following behaviors: (1) the nipple/breast was in the infant's mouth (as a marker of feeding time), (2) infant's gross motor activity (gross movement of the limbs, as a marker of overall activity level), and (3) burping the infant. Finally, we counted the number of times mothers offered the breast or bottle during the second half of the feeding session.
Nursing Child Assessment Satellite Training Caregiver/Parent–Child Interaction Feeding Scale Scores, and Feeding Behaviors of Breastfeeding and Bottle-Feeding Sessions of the Same Nine Mother–Infant Dyads ≤6 Months Postnatal from the Halifax Regional Municipality, Nova Scotia, Canada
Two-sided Wilcoxon signed-rank test.
p < 0.05.
NCAST, Nursing Child Assessment Satellite Training; min, minute(s); SD, standard deviation; sec, second(s).
Inter- and intracoder reliability
K.C.W. coded all videos between May 16 and June 4, 2018. K.C.W. and A.K.V. independently coded six common videos (three breast and three bottle) with high reliability (mean ρ = 0.91). High intracoder reliability was also achieved: K.C.W. duplicate-coded four videos (two breast and two bottle) between 7 and 13 days apart (mean ρ = 0.96).
Data analysis
Full feeding sessions were viewed a minimum of three times for NCAST assessment. 23 The midpoint for each feeding session was then calculated, and frame-by-frame assessment of the frequency of infant satiation cues and duration of behaviors was conducted on the second half of all feeding sessions.
Satiation cues and other behaviors were logged, and inter- and intrarater reliability were computed, using the ObserverXT software. All other data analysis was performed using SPSS for Macintosh v.23 (IBM Corp., Foster City, CA) with a significance level of p < 0.05. Descriptive statistics were computed for all variables. A Wilcoxon signed-rank test was used to assess NCAST scores, satiation cues, and other behaviors during the breastfeeding and bottle-feeding sessions because the data were not normally distributed and dyads' data were paired.
Results
Participant characteristics
The mean ± standard deviation (SD) age of mothers was 33.2 ± 4.0 years, eight (89%) self-identified as Caucasian, and all were highly educated (achieved college degree or higher). All women were married or in a common-law relationship, and five (56%) were first-time mothers. Infants were 14.6 ± 6.9 weeks, six (67%) were female, and while five (56%) were still exclusively consuming human milk, three (33%) had previously been fed infant formula, and one (11%) had recently started complementary feeding. Total feeding session duration (minutes:seconds) did not differ by feeding modality: breast, 12:39 (5:56); bottle, 11:15 (4:42) (p = 0.767).
NCAST caregiver/parent–child interaction feeding scale
NCAST scores are shown in Table 1. There was a significant difference in the mean ± SD Maternal Sensitivity to Cues subscale scores between feeding modalities: mothers were more sensitive to infant cues during the breastfeeding sessions (15.0 [1.0]) than during the bottle-feeding (13.4 [1.6]) sessions (p = 0.016).
Feeding behaviors during the second half of the feeding session
There was large, but not significantly different, variation in the number of cues displayed in the second half of the feeding session (Table 1). There was a significantly longer latency (minutes:seconds) from the feeding session midpoint to the first satiation cue during breastfeeding sessions (3:00 [1:53]) than bottle-feeding sessions (0:45 [1:18]; p = 0.038). There were no significant differences in the durations of behaviors, which are shown as a proportion of the second half of the feeding session in Figure 1.
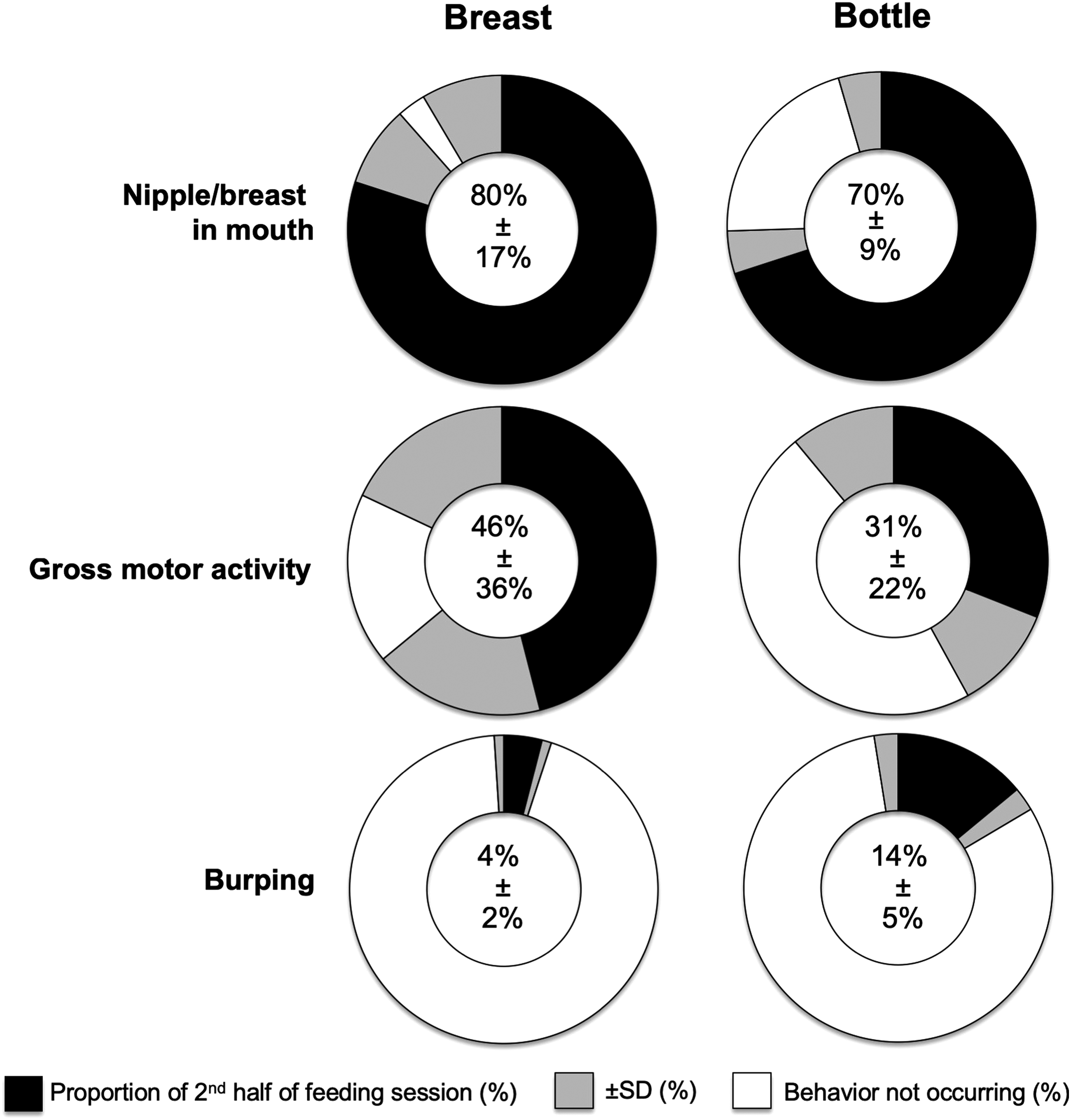
Duration of behaviors displayed as a proportion (%) of the second half of the feeding session, among breastfeeding and bottle-feeding sessions of the same nine mother–infant dyads ≤6 months postnatal from the Halifax Regional Municipality, Nova Scotia, Canada. SD, standard deviation.
Discussion
In this within-subject proof-of-concept study, we found that mothers exhibited greater sensitivity to their infants' cues while breastfeeding than when bottle feeding human milk. This finding supports the prevailing hypothesis that mothers exhibit greater responsiveness during breastfeeding than during bottle feeding, which may be due, in part, to the more active role infants play in the feed and the lack of other cues, such as the amount of milk left in the bottle. 26 Most previous research supporting this hypothesis similarly links breastfeeding to responsive feeding using between-subjects designs wherein breastfeeding and formula-feeding dyads are compared (e.g., Ref. 27 ); however, major limitations of this previous research include the inability to disentangle milk type from feeding modality and to rule out the possibility that mothers choose to breastfeed because they have a more responsive feeding style. 28 Thus, a strength of this study was our ability to control for these confounding factors that complicate associations between infant feeding choices and feeding outcomes to better isolate and understand associations between feeding modality and responsive feeding.
Feeding interactions are dyadic; thus, consideration of both mothers' and infants' contributions is important. In this study, we did not find a significant difference in the number of satiation cues displayed or level of gross motor activity in the second half of the feeding session by feeding modality, suggesting consistent infant signaling across different feeding contexts. This aligns with the results of another within-subject experiment, which illustrated no difference in the number of satiation cues displayed by formula-fed infants (n = 21) when fed under conditions wherein their mothers were asked to feed as they normally would at home (mother-led feeding) versus wherein their mothers were instructed by a research assistant to start and finish the feeding session in response to hunger and satiation cues (infant-led feeding). 29 In contrast, a recent between-subject analysis of infant communication illustrated that breastfed infants (n = 13) displayed more engagement and disengagement cues, indicative of hunger and satiation onset, respectively, compared with their formula-fed peers (n = 14). 13 Although all of these studies included small samples, the differential findings when comparing the between- and within-subjects studies may suggest that feeding mode does not influence infant communication, per se, rather that certain infants may communicate more than others. Further research is needed to understand how variation in infants' communication during feeding may affect—or be affected by—feeding choices and outcomes.
High maternal socioeconomic status is a limitation of this study, as a previous study indicates increased maternal responsiveness both among partnered and highly educated women. 22 Another limitation is the lack of random assignment to feeding sequence, which may have introduced order effect bias: all women in this study breastfed in the first feeding session, and bottle-fed human milk in the second. Strengths are that we video-recorded feeding sessions rather than relying on maternal self-report, 30 and we captured feeding sessions in a naturalistic setting.
Conclusions
This pilot study was the first to employ a within-subject design to assess maternal feeding responsiveness and describe infant satiation cues among dyads consuming human milk from the breast versus the bottle. Mothers were more sensitive to infant cues while breastfeeding. These pilot study results suggest that there are differences in infant feeding responsiveness by feeding modality even within the same dyad consuming the same food (human milk), which warrants further investigation at a larger scale.
Footnotes
Acknowledgments
We thank all the participants of this study, and Jolene Bianco for her assistance with data collection. This study was supported by the International Society for Research in Human Milk and Lactation (ISRHML)-Family Larsson-Rosenquist Foundation Trainee Expansion Program Trainee Travel Fund. The funder had no role in the design, analysis, or writing of this article.
Disclosure Statement
No competing financial interests exist.