
Abstract
Abstract
Background:
Breast milk Chitotriosidase (Chit 1) shows antifungal effect and has an active role in the natural immune response against certain pathogens. The aim of this study was to compare colostrum Chit 1 levels from mothers of term and preterm infants.
Materials and Methods:
The study included 72 mothers of 32 preterm and 40 term infants (gestational age; 33.7 ± 1.8 vs. 39.1 ± 1.1 weeks, birth weight; 1931.7 ± 539.8 vs. 3350.9 ± 419.7 g). Breast milk samples were taken at postnatal 24–48 hours. Chit 1 level was evaluated with the quantitative calorimetric method.
Results:
No significant difference was determined between the term and preterm groups in terms of maternal age, education level, weight gain in pregnancy, and body mass index (BMI). The median colostrum Chit 1 level was higher in the preterm group, but the difference was not statistically significant between two groups (p = 0.43). There is no association between colostrum Chit 1 level, maternal age, gravida, BMI, infant gender, income level, and pre-eclampsia. The colostrum Chit 1 level of mothers who had weight gain exceeding the recommended limits was significantly lower than mothers with weight gain within the recommended limits in the term group (4346.2 vs. 4914.2, p = 0.021). A negative correlation was determined between the birthweight of term infants and the colostrum Chit 1 levels (p = 0.045, r = −0.319).
Conclusion:
Although the data need to be validated by further investigation, the observations made in this study seem to indicate that colostrum Chit-1 may have role in the protection of preterm infants.
Introduction
The neonatal period for both term and preterm infants is a sensitive period with a high risk of morbidity and mortality. According to World Health Organization (WHO), 2.6 million infants died worldwide in 2016 in the neonatal period. Infections are responsible for one-third of neonatal deaths. 1 Various strategies have been defined to reduce neonatal infections and the associated mortality rates; breast milk is still the most critical factor in the protection against infections for both term and preterm infants.2,3
Breast-fed infants expose to fewer and more mild infections compared to formula-fed infants.4–6 Various components such as secretory IgA, oligosaccharides, lysosomes, lactoferrin, lactoperoxidase, bacterial and maternal-origin cells, glycopeptides, fatty acids, monoglycerides, and leukocytes have an anti-infective effect in the breast milk.7–9 It has been reported that various chemokines and cytokines are found in greater amounts in the breast milk and these substance protect preterm infants against sepsis and necrotizing enterocolitis.10–14 However, investigations on the immunological content of breast milk are still ongoing. Chitotriosidase (Chit 1), which has been determined in breast milk in recent years, has anti-infective effects.15,16
Chitin, which is one of the biopolymers found most abundantly in nature, is an important structural component of fungi, parasites, and various insects.17,18 These pathogens use chitin to protect themselves from harsh conditions in the host cell. Chitinases are a protein family that fragment chitin by binding to it and thereby play a role in the defense against pathogens containing chitin. Although structural chitin is not found in the human body, there is chitinase enzyme activity. Chit 1 is the first discovered and defined mammalian chitinase. 19 Chit 1 is primarily produced from macrophages and neutrophils, and then secreted in response to various stimuli. Although the structural properties of Chit 1 in humans have been determined in detail, the biological functions have still not been fully clarified. It has been reported that Chit 1 is effective in the defense against fungal and parasitic infections. 20 The function of Chit 1 is not limited to chitinolytic activity; it is also thought to have an active role in the natural immune response, which develops against bacteria, fungi, and nonviral pathogens.21,22
There is limited study on the levels of colostrum Chit 1 in mothers of term and preterm infants. The hypothesis of this study was that Chit 1 enzyme, which has an anti-infective property, would be found at greater amounts in the colostrum of the mothers of preterm infants, who are at higher risk of infections. The aim of the study was to compare the levels of Chit 1 in colostrum obtained postnatal 24–48 hours from the mothers of term and preterm infants, and to investigate the factors that could affect the level of Chit 1 in breast milk. This study gives an important opportunity to improve our existing information about the colostrum Chit 1 levels in mothers of preterm and term infants.
Materials and Methods
The study included mothers who gave birth in the Medical Faculty Hospital of Sivas Cumhuriyet University between February 2017 and August 2017. All the mothers were interviewed by the researchers and the medical histories were evaluated. Mothers were excluded from the study if they had any chronic disease or any history indicating suspicion of inflammatory disease, alcohol or drug use, early membrane rupture (>18 hour before delivery), chorioamnionitis, or determined infection. Further exclusions were made of infants with a low birthweight according to gestational week, severe congenital malformation, congenital metabolic disease, sepsis, pathological jaundice, cyanotic congenital heart disease, and perinatal asphyxia and mothers with renal/hepatic failure. Verbal and written informed consent were obtained from all the mothers who participated in the study. Approval for the study was granted by the Ethics Committee of Cumhuriyet University (Ethics committee approval no: 2017-01/23, date: January 1, 2017).
The infants and mothers were separated into two groups as the term group who gave birth after completion of the 37th week of pregnancy according to the date of last menstruation, and the preterm group comprising those who gave birth before the 37th week of pregnancy. The sociodemographic and medical data of the mothers and infants were recorded. Levels of family income were recorded based on the information given by the mothers. Prepregnancy body mass index (BMI) of the mothers was calculated using the following formula: BMI = weight/height 2 . The weight gain in pregnancy was also recorded. BMI was categorized according to the WHO classification. 23 The weight gain recommended in pregnancy according to the prepregnancy BMI values were as follows: for BMI <18.5 kg/m2; 12–18 kg, for BMI 18.5–24.9 kg/m2; 11–16 kg, for BMI 25.0–29.9 kg/m2; 6–11 kg, and for BMI ≥30.0 kg/m2; 4–9 kg, and weight gains within these limits were accepted as normal. 24
The colostrum samples were obtained from the mothers at postnatal 24–48th hours from the first milk expressed by hand or pump in the morning between 06:00 and 10:00. Approximately 2–3 mL colostrum was expressed from the breast into a plastic tube and immediately taken to the hospital laboratory.
Sample analysis
The whole milk samples were centrifuged at 4,000 g for 10 minutes, after which the lipid layer and aqueous fractions were removed. An aliquot of the aqueous fractions was stored at–20°C until assay for Chit 1 levels. A quantitative colorimetric sandwich ELISA kit was used to measure Chit 1 levels (Elabsciences, China). The coefficients of variation for intra-assay and interassay were 3.13% and 4.78%, respectively. The sensitivity of the assay was 46.88 pg/mL.
Statistical analysis
Conformity of the data to normal distribution was evaluated using a histogram, q-q graphs, and the Shapiro–Wilk normality test. The Mann-Whitney U and Student's t-tests were performed for comparisons of nonparametric and parametric variables, respectively. Correlations between quantitative data were assessed using the Spearman test. Figures were obtained using BoxPlotR, a web-tool for the generation of box plots (http://shiny.chemgrid.org/boxplotr). The analyses were conducted using Turcosa Cloud (Turcosa Ltd Co, Turkey) statistical software. A value of p < 0.05 probability level was considered statistically significant.
Results
The study included 72 mothers and infants, comprising 32 preterm and 40 term infants. In the preterm infant group, the reasons for early birth were pre-eclampsia in 18 (56.2%), early labor in 11 (34.4%), placenta anomaly in 2 (6.2%), and oligohydramnios in 1 (3.1%). No significant difference was determined between the mothers of the term and preterm infants in terms of age, education level, weight gain in pregnancy, and BMI. Cigarette smoking in pregnancy was reported in 1 (3.1%) mother in the preterm group and 2 (5.0%) mothers in the term group. Primiparity and delivery by caesarean section rates were higher in the preterm group than in the term group (p < 0.001 and p < 0.001, respectively) (Table 1).
Characteristics of Preterm and Term Groups
Mean ± standard deviation.
Data range (minimum–maximum).
Statistically significant differences are indicated in bold font.
BMI, body mass index; cm, centimeter; g, gram; h, hour; kg, kilogram; NICU, Neonatal Intensive Care Unit; NSVD, Normal spontaneous vaginal delivery.
Colostrum was obtained at mean 38.9 ± 6.4 hours postnatal in the preterm group and at mean 36.9 ± 7.4 hours in the term group. The milk was obtained with a pump in five (15.6%) mothers in the preterm group and in one (2.5%) in the term group. No significant differences were determined between the groups in terms of milk collection time (p = 0.23) and milk obtaining technique (p = 0.08). The colostrum Chit 1 levels were 4834.2 (4396.2–5434.2) and 5186.2 (4660.2–5362.2) pg/mL in the term and preterm groups, respectively (p = 0.43). Results were given as median (first to third quartiles) (Fig. 1).
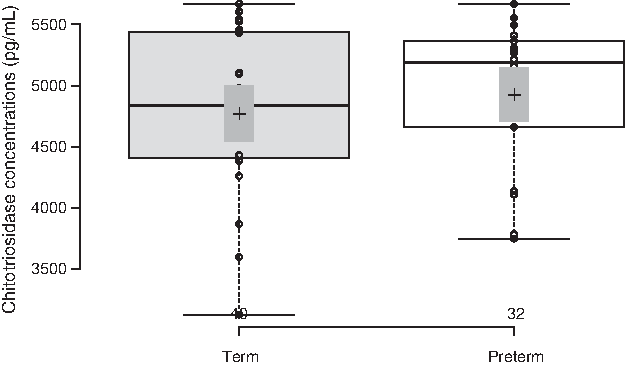
Comparison of chitotriosidase concentrations between term and preterm groups. The center lines show the medians; box limits indicate the 25th and 75th percentiles as determined by R software; whiskers extend 1.5 times the interquartile range from 25th and 75th percentiles, outliers are represented by dots; crosses represent sample means; bars indicate 95% confidence intervals of the means; data points are plotted as open circles. n = 40, 32 sample points.
The Chit 1 levels in the colostrum of all the mothers in the term and preterm groups were evaluated separately with the maternal age, gravida, weight gain in pregnancy, BMI, mode of delivery, family income level, and infant sex, birthweight, and length percentiles. The only parameter determined to have an effect on Chit 1 level was the weight gain in pregnancy of the mothers in the term group. Chit 1 level in the colostrum of mothers with ≥13 kg weight gain in pregnancy was found to be significantly lower compared with mothers having <13 kg weight gain in the term group (p = 0.029). The colostrum Chit 1 level of mothers who had weight gain exceeding the recommended limits was significantly lower than mothers with weight gain within the recommended limits in the term group (p = 0.021) (Table 2).
CHIT-1 Values of the Term and Preterm Group for Different Group Variables
n#, The number of patients in the term group; n¤, the number of patients in the preterm group. The data are expressed as median (25–75 percentile).
Statistically significant differences are indicated in bold font.
C/s, Cesarean section.
The most common reason for early birth in the preterm group was determined to be pre-eclampsia, at the rate of 56.2%. To be able to determine whether or not pre-eclampsia had any effect on the colostrum Chit 1 levels of mothers with pre-eclampsia, the colostrum Chit 1 levels were compared in the preterm group according to the presence or absence of pre-eclampsia. The Chit 1 levels were determined to be 5186.2 (4129.2–5374.2) pg/mL in the mothers with pre-eclampsia and 5220.2 (4768.2–5374.2) pg/mL in the mothers without pre-eclampsia, with no significant difference determined between them (p > 0.05) (Fig. 2).
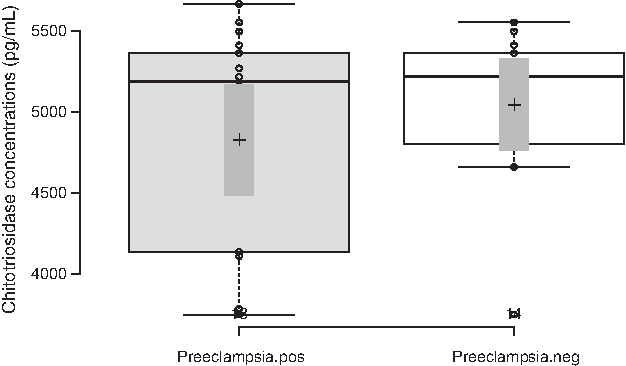
Comparison of chitotriosidase concentrations between pre-eclampsia positive and negative groups. The center lines show the medians; box limits indicate the 25th and 75th percentiles as determined by R software; whiskers extend 1.5 times the interquartile range from the 25th and 75th percentiles, outliers are represented by dots; crosses represent sample means; bars indicate 95% confidence intervals of the means; data points are plotted as open circles. n = 18, 14 sample points.
A weak negative correlation was determined between infant birthweight in the term group and the Chit 1 enzyme level measured in the colostrum (Table 3).
CHIT-1 Correlations with Different Variables in the Term and Preterm Groups
p < 0.05.
Statistical significance correlation is indicated in bold font.
Discussion
Chit 1 in breast milk primarily shows an antifungal effect, but it has been reported that this enzyme may increase in various viral and bacterial infections.25,26 Labadaridis et al. 27 determined a high level of Chit 1 in blood and urine samples of neonates with both fungal and bacterial sepsis. In a study by Tunc et al., 16 Chit 1 enzyme activity was measured in the postnatal third day colostrum of mothers of term and preterm infants. It was determined that Chit 1 enzyme activity was higher in the preterm group, but the difference was not statistically significant, similar to the results of our study.
In another study related to Chit 1 enzyme, the mode of delivery was not seen to have any effect on the enzyme activity in the cord blood. 28 Similarly, in our study, it was not found that the mode of delivery had no significant affect on the Chit 1 levels in colostrum. In another study, Alanbay et al. 29 stated that there was no difference in the plasma Chit 1 enzyme activity of women with BMI <25 kg/m2 and those with BMI ≥25 kg/m2. In this study, we did not find an association between the prepregnancy BMI values and colostrum Chit 1 levels.
Musumeci et al. 15 reported that Chit 1 enzyme activity in colostrum samples taken at postnatal 24, 48, and 72nd hours was higher in African mothers than Italian mothers. Different levels of Chit 1 enzyme activity have been reported in different ethnic groups, and the difference in the above-mentioned study can be explained by different Chit 1 genetic polymorphism in sub-Saharan and Mediterranean regions.15,22
The results of this study demonstrated that the only factor affecting the Chit 1 level in colostrum was the extra weight gain in pregnancy of mothers in the term group (Table 3). The median colostrum Chit 1 level was found to be lower in mothers who had put on more weight than recommended in pregnancy in the term group than the preterm group. Rastogi et al. 30 reported 1.3-fold higher risk of postnatal sepsis in term infants of mothers who had higher than recommended weight gain in pregnancy. We speculate that there may be an association between the increased risk of sepsis in infants of mothers with a greater weight gain in pregnancy and decreased colostrum Chit 1 levels in the term group.
To the best of our knowledge, no study has observed the relationship between birthweight and colostrum Chit 1 levels. In this study, we found negative correlation between birthweight and colostrum Chit 1 levels in the term group. Gunes et al. 31 found the positive correlation between cord blood Chit 1 activity and birthweight in preterm infants. However, it has been reported that there is no significant correlation between serum Chit 1 activity and BMI in obese children. 32 Discordant results between studies may be related with the differences of studied samples and patient groups. Inflammatory cytokines have an important role on the releasing mechanism of Chit 1. 33 Ustundağ et al. 34 found decreased colostrum cytokine levels in term infants compared to preterm infants. Therefore, we think that decreased cytokine levels might be related with negative correlation between Chit 1 levels and birthweight.
In the preterm infant group of this study, the reason for early birth was determined to be pre-eclampsia in 56.2%. In some studies, Chit 1 enzyme activity has been determined to be higher in the serum and cord samples of pre-eclamptic mothers compared to the values of mothers without pre-eclampsia. Increased Chit 1 enzyme expressions have been associated with increased macrophage activation in pre-eclamptic women.35,36 It has been also reported that Chit 1 level could be used as an inflammatory marker in the diagnosis of pre-eclampsia. 34 A previous study found no correlation between Chit 1 enzyme activity in the colostrum and plasma activity, and it was thought that this enzyme is expressed locally from active macrophages in breast tissue. 15 In our study, Chit 1 level was measured only in colostrum and no significant difference was determined between pre-eclamptic and non-pre-eclamptic mothers of preterm infants in terms of colostrum Chit 1 levels. The different results between aforementioned studies and our study may be related with the studied sample type differences. In addition, Chit 1 releasing kinetics may also vary in plasma and colostrum.
Conclusion
Although the results of this study were not statistically significant, the Chit 1 levels in the colostrum of mothers of preterm infants were seen to be higher than mothers of term infants. The increase in Chit 1 level in colostrum of preterm infants suggests that the enzyme could be involved in the protection mechanism of colostrum in preterm infants against fungal colonization. However there is a need for further, more extensive, and large-scale studies on this subject.
Footnotes
Acknowledgments
The authors thank all the mothers who participated in the study for their contributions.
Disclosure Statement
No competing financial interests exist.