
Abstract
Abstract
Introduction:
We described calls to U.S. poison centers (PCs) related to potential exposure to substances through breast milk.
Materials and Methods:
We analyzed National Poison Data System calls between 2001 and 2017 with “Exposure through breast milk” or “Drug use during breastfeeding” as the coded scenario. Data handling and descriptive statistics were carried out using SAS JMP 12.01.
Results:
U.S. PCs received 76,416 information calls and 2,319 exposure calls related to breast milk. Exposure calls were from a residence in 76% (n = 1,758), from health care facilities (HCFs) in 15.5% (n = 360), and from a workplace in 0.6% (n = 15). A total of 466 exposures (20.1%) were subsequently managed at a HCF: 269 were evaluated and released (58%), 38 were admitted to intensive care unit (8.2%), and 53 were admitted to hospital floor (11%). Medical outcomes included 1 death (0.04%), 8 major effect (0.3%), 43 moderate effect (1.9%), 170 minor effect (7.3%), and 390 no effect (16.8%). Exposure calls that reported major effects involved opioids, benzodiazepines, ethanol, cyclobenzaprine, insulin, and amphetamines. Exposure calls most commonly involved antibiotics, antifungals, benzodiazepines, opioids, and selective serotonin reuptake inhibitors (SSRIs). A total of 1,192 exposures (51.4%) had reported signs/symptoms including drowsiness, agitation, rash, and vomiting/diarrhea. Information calls most commonly involved systemic antibiotics, SSRIs, antihistamines, corticosteroids, and benzodiazepines.
Conclusions:
Substances common to both exposure and information calls included antibiotics, benzodiazepines, and SSRIs. Most cases of severe toxicity included potential exposures through breast milk to benzodiazepines and opioids. These data may help inform educational outreach, risk assessment, and bedside care for breastfeeding mothers.
Introduction
Lactating women or other individuals may consult a U.S. poison center (PC) to obtain information about the safety of a medication during lactation, or to report a potential exposure to an infant through breast milk. There is a paucity of published data on the individuals or substances involved in breast milk exposure or information calls to U.S. PCs. We sought to describe the characteristics of patients and the substances involved in such calls.
Available literature on infant exposure to medications and drugs in breast milk suggests that few patients develop severe symptoms, but minor gastroenterological and neurological adverse events may occur and include reactions to maternal use of antibiotics, analgesics, antihistamines, benzodiazepines, antidepressants, and antiepileptics.1–3 Rare severe reactions have been reported, mostly to opioids and benzodiazepines.2,4 Most data consist of case reports and most infants affected are aged 1 to 2 months.3,4 The incidence and characteristics of adverse drug reactions among breastfed infants remain poorly defined and limited by a lack of available data. 3
The National Poison Data System (NPDS), developed and maintained by the American Association of Poison Control Centers, collects data from all calls to U.S. PCs regarding a diverse range of potential poisoning exposures that include exposures to prescribed or over-the-counter medications, foreign bodies, sources of infection, venomous or poisonous organisms, commercial products, chemical agents, and others. 5 In this capacity, NPDS serves as a national exposure and information database, and surveillance tool for potential poisoning. 5 Data are collected on a voluntary basis from members of the public, law enforcement, Emergency Medical Services, or health care professionals, and is done so around the clock, every day of the year, without cost to the caller. 5
Data are collected by PCs using a standardized electronic record with mandatory data elements including demographics, substances involved, reason for the call to the PC, presenting signs and symptoms for exposed individuals, interventions performed or recommended, and outcomes.
We sought to add to the existing literature by describing breast milk exposure and information calls to U.S. PCs for a 17-year period.
Materials and Methods
This study was deemed “nonhuman subjects research” and thus not subject to Institutional Review Board full review.
We used the enterprise report designed to provide case listings to retrieve all closed human exposure cases from January 1, 2001, to December 31, 2017, with scenario = exposure through breast milk (exposure calls) and call subcategory = drug information – drug use during breastfeeding (information calls).
Data handling and descriptive statistics (case counts, means, standard deviation distributions, and analyses of changes over time) for these data including substances involved, effects, and disposition were carried out using SAS JMP 12.01.
Results
For 2001–2017, U.S. PCs received 2,319 exposure calls and 76,416 information calls related to breast milk. Data collection within these categories began in 2001.
Exposure calls
Exposures to substances in breast milk included children who were 51% female (n = 1,184), 41% male (n = 948); gender was not provided in 8% (n = 186). Calls were initiated mostly from the caller's own residence (76%, n = 1,758) with 16% (n = 360) from health care facilities (HCFs) and 0.6% (n = 15) from a workplace. Most of the exposure calls were managed on site (78%, n = 1,802), 297 were en route to a HCF when PC was called (12.8%), and 169 were referred to a HCF (7.3%).
Of the 466 exposures (20.1%) managed at a HCF, 269 were evaluated and released (58%), 38 were admitted to intensive care unit (8.2%), 53 were admitted to a hospital floor (11%), 86 were lost to follow up, or left against medical advice (18%).
Medical outcomes included 1 death (0.04%), 8 major effect (0.3%), 43 moderate effect (1.9%), 170 minor effect (7.3%), and 390 no effect (16.8%). Death occurred in a 4-month-old boy with a possible exposure to benzodiazepines, opioids, and a selective serotonin reuptake inhibitor (SSRI) through breast milk; however, the death was subsequently judged as unrelated to the exposure. The substances associated with major effects among breastfed infants included opioids, benzodiazepines, ethanol, cyclobenzaprine, insulin, and amphetamines (Table 1). Among cases with major effects, two were managed with endotracheal intubation: a 4-month-old infant with reported exposure through breast milk to methadone, benzodiazepine, and SSRI and a 1-month-old infant with reported exposure to methadone. Cases with reported major effects that were managed with naloxone included the 1-month-old infant with reported breast milk exposure to methadone; a 13-month-old infant with reported breast milk exposure to methadone; and a 17-month-old infant with reported breast milk exposure to fentanyl, morphine, oxycodone, and lorazepam.
Infants with Exposures to Substances Through Breast Milk with Medical Outcome of Major Effect or Death Reported to the National Poison Data System 2001–2017
ICU, intensive care unit; SSRI, selective serotonin reuptake inhibitor.
The substances most commonly reported to be involved in exposure calls were antibiotics, antifungals, benzodiazepines, opioids, and SSRIs. Figure 1 shows the substances (by generic code) most commonly reported in exposures. A total of 1,192 exposures (51.4%) had reported signs/symptoms. The most common signs/symptoms were drowsiness, agitation, rash, and vomiting/diarrhea (Fig. 2).

Most common substances involved in exposures to substances through breast milk reported to the NPDS 2001–2017. Exposure calls are listed as percentage of 2,319 total exposures through breast milk reported to NPDS. For comparison, information calls (“Info Calls”) for the same substances are listed as percentage of 76,416 total information calls about exposure through breast milk. NPDS, National Poison Data System.
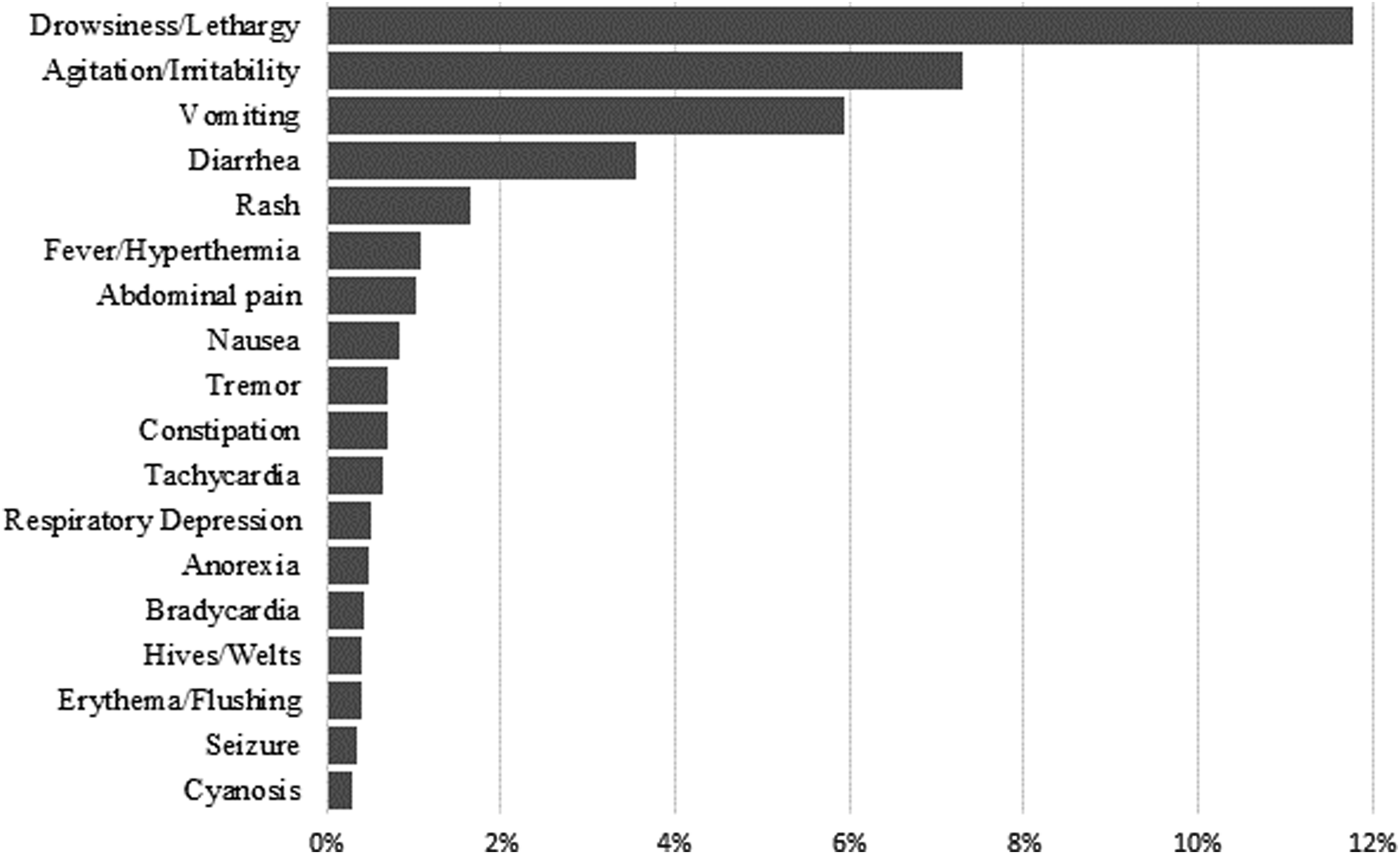
Most common clinical effects reported for exposures to substances through breast milk reported to the NPDS 2001–2017. Clinical effects are reported as a percentage of the 2,319 total exposures through breast milk reported to NPDS during this time period.
Figure 3 shows incidence of calls to PCs regarding potential exposures through breast milk over time.

Exposures to substances through breast milk reported to the NPDS, by year, 2001–2017. Graphed line shows smoothing (spline) fit to the data with λ = 10—associated R2 = 0.602.
Information calls
For comparison, data on information calls for the same substances most commonly reported during exposure calls are included in Figure 1. Information calls were most commonly in reference to systemic antibiotics, SSRIs, antihistamines, corticosteroids, and benzodiazepines.
Discussion
In this study, serious adverse events related to exposures to medications occurring during breastfeeding were rare. Given this rarity, and that only a small proportion of medications are contraindicated during breastfeeding, the risks versus benefits of continuation of beneficial pharmacotherapies while breastfeeding should likely be assessed on an individual basis. 6
The finding in this study that opioids and benzodiazepines were most commonly involved in serious adverse events related to exposures during breastfeeding is consistent with existing literature.2,4 A case of fatal opioid toxicity in a neonate occurred after exposure through breastfeeding of an infant by a mother who was an ultrarapid metabolizer of codeine. 7 Risk factors include higher maternal dose and maternal/infant concordance of central nervous system (CNS) depression. 8 Genetic polymorphisms in drug metabolism were also found to play a significant role in severe outcomes among infants exposed to substances through breast milk. 8 A systematic review of the literature using the Naranjo Adverse Drug Reaction Probability Scale to determine causality found codeine to be a definite cause of CNS depression among breastfed infants, with concerning features associated with breastfeeding during codeine use that included apnea, bradycardia, and cyanosis. 9 Maternal oxycodone use has been associated with higher risk of CNS depression in breastfed children. 10 Several cases of opioid toxicity from exposure to breast milk have been reported and note risk factors of higher maternal dose and opioid-naive child. 4
It is notable that 88% (7/8) of serious effects associated in infants of lactating mothers were associated with opioids. The finding that 50% (4/8) of exposures resulting in serious effects were associated with methadone use is of interest, given that the rate of breastfeeding among women in methadone maintenance is half that of the national average. 11 Existing data suggest there is low transfer of methadone into breast milk, and that the risk of methadone toxicity among breastfed infants is likely outweighed by the potential benefit.11,12 More research is needed to explore risks versus benefits of the use of pharmacotherapies to support recovery from substance use disorder among breastfeeding women. 13 In one study in which serum medication concentrations were obtained from breastfed infants of mothers managed with psychotropic medications, only 26% had detectable parent drug or active metabolites, of which none was associated with any adverse events. 14
A review of the available literature between 1976 and 2017 found that despite no large-scale controlled studies evaluating the safety of psychotropic medications during breastfeeding, reports of serious adverse events were rare, and pharmacokinetic studies predicted low breast milk concentrations of commonly prescribed medications. 15 The benefits of maternal therapy with pharmaceuticals must be weighed against the potential risk to the breastfeeding infant, with consideration of individual variations in response to standard dosing of a drug, the dose–response relationship for particular pharmacotherapies, and the implication of pharmacogenetics in both infant and mother. 16
Limitations to using NPDS data for this study include our inability to confirm either the etiologic agent of exposure or the definitive occurrence of an exposure. Since collected data rely on voluntary reporting, reported exposures may not be representative of general outcomes related to exposure type. 17 Since the “scenarios” is an optional data field during data entry, it seems likely that breast milk exposures are under-reported within NPDS. Finally, given the limitations of the NPDS database, we were unable to gather specific information about the timing of the signs and symptoms of toxicity in relation to the reported exposure to medication through breast milk, or the type of breastfeeding (intermittent/supplemental versus sole source of nutrition for the infant).
Conclusion
Substances common to both exposures through breast milk and information calls concerning medication or other drug use during breastfeeding included antibiotics, benzodiazepines, and SSRIs. Most cases of severe toxicity included potential exposures through breast milk to benzodiazepines and opioids. These data may help inform educational outreach and bedside care for breastfeeding mothers. Further study into exposures through breast milk may help inform an understanding of the potential risks of substance exposure to breastfed infants.
Footnotes
Acknowledgment
The authors thank Daniel Higgins, MLIS, for his assistance with proofreading.
Disclaimer
The American Association of Poison Control Centers (AAPCC; ![]() ) maintains the national database of information logged by the country's poison centers (PCs). Case records in this database are from self-reported calls: they reflect only information provided when the public or health care professionals report an actual or potential exposure to a substance (an ingestion, inhalation, or topical exposure, etc.), or request information/educational materials. Exposures do not necessarily represent a poisoning or overdose. The AAPCC is not able to completely verify the accuracy of every report made to member centers. Additional exposures may go unreported to PCs and data referenced from the AAPCC should not be construed to represent the complete incidence of national exposures to any substance(s).
) maintains the national database of information logged by the country's poison centers (PCs). Case records in this database are from self-reported calls: they reflect only information provided when the public or health care professionals report an actual or potential exposure to a substance (an ingestion, inhalation, or topical exposure, etc.), or request information/educational materials. Exposures do not necessarily represent a poisoning or overdose. The AAPCC is not able to completely verify the accuracy of every report made to member centers. Additional exposures may go unreported to PCs and data referenced from the AAPCC should not be construed to represent the complete incidence of national exposures to any substance(s).
Disclosure Statement
The authors have no conflicts of interest to report.