
Abstract
Background:
Exclusively breastfed infants are at risk of vitamin D deficiency.
Objective:
To find out proportion of exclusively breastfed infants having serum 25(OH)D concentration <11 ng/mL at 6 months of age with or without oral supplementation of vitamin D3 to lactating mothers.
Methods:
Randomized placebo-controlled study included 132 mothers and infants divided into two groups. Mothers received either vitamin D3 60,000 IU between 24 and 48 hours postpartum and at 6, 10, and 14 weeks amounting to 240,000 IU of vitamin D3 or placebo. Serum 25(OH)D concentration in the mothers was measured at recruitment and that of infants, at birth and 6 months. Infants were evaluated for rickets at 6 months.
Findings:
Total 114 mother–infant dyads followed. Subjects in both groups were comparable in basic characteristics. At 6 months of age, serum 25(OH)D concentration in infants was 18.93 (5.12) ng/mL in the intervention group and 6.43 (3.76) ng/mL in the control group (mean difference = 12.5; 95% CI = 10.80–14.17; p < 0.001) and vitamin D deficiency and insufficiency was corrected in 93.1% and 38% infants, respectively, in the intervention group. There was no change in the vitamin D status of infants in the control group. In 60.3% infants (RR = 0.519; 95% CI = −0.485 to 0.735) of the intervention group 25(OH)D concentration was <20 ng/mL at 6 months of age. Six infants in the control group suffered from biochemical rickets. Radiological rickets developed in one infant in the intervention group and two infants in the control group.
Conclusion:
Serum 25(OH)D concentration of exclusively breastfed infants rise significantly when mothers are orally supplemented with 240,000 IU of vitamin D3 during lactation in comparison with the infants of unsupplemented mothers with 94.6% and 48.1% reduction in the risk of vitamin D deficiency and insufficiency, respectively, at 6 months of age.
Introduction
Exclusive breastfeeding till 6 months of age followed by timely introduction of adequate and proper complementary feeding along with continued breastfeeding for at least 2 years of age reduces mortality by 20% in children <5 years of age. 1 However, it has been observed lately that exclusively breastfed infants are prone to develop nutritional rickets more often than their formula-fed peers.2,3 A large number of reports published in the past decade shows that pregnant and lactating women in both developed and developing countries, including those areas having abundant sunshine, are vitamin D deficient.4–6 There is a significant correlation between the maternal and infant's serum 25(OH)D concentration at 6 weeks, 3 months, and 6 months postpartum2,5 and with the breast milk vitamin D contents. 7 Infants are, therefore, routinely administered vitamin D to prevent its deficiency. 8 Although daily supplementation of vitamin D to newborn infants has been recommended, compliance by the parents,9,10 practices of pediatricians, 11 and the risk of incorrect dosing (both under- and overdosing) are major concerns.12,13 Vitamin D directly and indirectly regulates expression of 2–3% of the human genome 14 and caution has been sounded for the long-term supplementation of vitamin D, as it may affect immunomodulation and regulation of the expression of the genes and may cause obesity and chronic illnesses. 15 Long-term safety of vitamin D supplementation to newborn infants since birth, therefore, remains to be investigated.
Some researchers have looked at the problem of vitamin D deficiency in the exclusively breastfed infants from another angle. They supplemented lactating mothers with vitamin D in the postpartum period and found that vitamin D deficiency in infants was significantly reduced and no adverse effects were observed either on the mothers or infants.16–18 This strategy helps combating vitamin D deficiency in the mother as well. We conducted a study to find the effect of vitamin D supplementation to the breastfeeding mothers, on the days of primary immunization, on the vitamin D status of the exclusively breastfed infants at the age of 6 months.
Objectives
The objectives of the study were as follows: (1) to compare the proportion of exclusively breastfed infants having vitamin D deficiency [serum 25(OH)D concentration <11 ng/mL] at the age of 6 months with their mothers being supplemented during lactation with or without 240,000 IU vitamin D3 and (2) to find out number of infants developing radiological and biochemical rickets at 6 months of age in both the groups.
Methods
Trial design
Based on P(population) I(intervention) C(comparator) O(outcome) design it was a randomized (1:1) double-blind placebo-controlled trial carried from March 2015 to April 2016, after obtaining approval from the Institution Ethics Committee for Human Research. The trial was carried out in the Division of Neonatology, Department of Pediatrics, in a teaching hospital.
Subjects
After obtaining informed written consent 132 consecutive mothers in labor with term gestation (37–41 completed weeks), by last date of menstruation; and their infants were recruited. Information pertaining to diet, dressing habit, sunlight exposure, and other relevant data were recorded in a predesigned form. Newborn infants were thoroughly examined after birth and the gestation age was reassessed by the Modified Ballard's scoring 19 ; if there was difference of >2 weeks in the estimated gestation age by two methods then Modified Ballard scoring was taken into account. Only term appropriate for gestational age babies were included in the study.
Exclusion criteria
Neonates who were low birth weight, had congenital, chromosomal or endocrinological disorders, suffered perinatal asphyxia, hypocalcemia, hypoglycemia, respiratory distress, intracranial infection, or had undergone exchange blood transfusion were excluded from the study. Mothers known to be suffering from chronic illnesses like tuberculosis, diabetes mellitus, chronic liver disease, chronic kidney disease, severe anemia, HIV, hepatitis B, gestational diabetes mellitus, pregnancy-induced hypertension, hypothyroidism, or who had received vitamin D in the last 3 months [apart from Tab ostocalcium (elemental calcium 500 mg, vitamin D3 250 IU), given during antenatal period under national antenatal program] were also excluded.
As a hospital policy, all the mothers were counseled to initiate breastfeeding within an hour. No prelacteal feeds were given by any mother. However, 10 mothers, 4 and 6 mothers in the intervention and control groups, respectively, gave few sips of water or juice to the infants on some occasion; these predominantly breastfed infants have been included in the study. One infant was excluded from the control group on account of mixed feeding.
Randomization and blinding
Randomization was performed with the help of a computer-generated randomization table, by a third person who was not directly involved in the study, into two groups to receive either drug (vitamin D3) or placebo. The drug and placebo were coded in the randomization sequence as A or B and serially numbered in a randomization sequence from 1 to 132 and the key was kept by the same person. The allocation of the mother–infant pair to intervention or control group was carried out by serially numbered opaque sealed envelope concealment technique. The randomization key was decoded in two steps. First, the serial numbers were converted to either A or B and data were analyzed. After the statistical results were available, the second decoding was carried out; “A” stood for vitamin D3 and “B” for placebo. Thus, subjects, investigators, and data analyzer were not aware of the characteristics of the two groups until the results were revealed.
Administration of vitamin D or placebo
Each Vitanova® sachet contained 60,000 IU of cholecalciferol (vitamin D3) and placebo was an inert sugar. Vitamin D3 and placebo were similar in texture and appearance. One sachet containing either 60,000 IU vitamin D3 or placebo was given to the mother between 24 and 48 hours after delivery, and at 6, 10, and 14 weeks postpartum to swallow with water under direct supervision and the infant was immunized as per the National Immunization Schedule. Thus, all mothers consumed 4 sachets of either vitamin D3 amounting to a total of 240,000 IU vitamin D3, which was equivalent to approximate daily dose of 2,449 IU, or a placebo when their infants were being immunized with Bacillus Calmette Guerin (BCG) vaccine, live oral polio vaccine (OPV), and hepatitis B vaccine (HBV) 24–48 hours after birth and subsequently on three occasions with pentavalent vaccine, inactivated polio vaccine (IPV) and OPV at 6, 10, and 14 weeks of age.
Follow-up
The weight, length, head circumference, chest circumference, and area of the anterior fontanelle of all the infants were measured at birth as per standard methods. Each mother and baby was followed up at 6(+1), 10(+1), 14(+1) weeks and at 6 months (+2 weeks) of age. The mother was counseled to practice exclusive breastfeeding and advised not to take vitamin D supplements. Infants were immunized as per National Immunization Schedule and their weight, length, head circumference, chest circumference, and area of the anterior fontanelle were measured. Detailed physical examination was carried out and sunlight exposure was recorded. At 6 months of follow-up, the mothers were counseled to continue breastfeeding and encouraged to start complimentary feeding. Mothers and infants were evaluated for clinical evidence of hypercalcemia, as a result of vitamin D toxicity, by history and examination, in the form of poor feeding, polyuria, vomiting, constipation, seizures, and lethargy and hypotonia at each follow-up. Serum calcium, phosphorus, and alkaline phosphatase concentrations were measured in the infants at 6 months of age for evidence of biochemical rickets.
Investigations
At the time of recruitment, the maternal venous blood and cord blood samples were collected after delivery; serum separated and stored at −20°C for estimation of 25(OH)D concentration. At 6 months of age, venous blood was drawn to measure infants' serum 25(OH)D and serum calcium, phosphorus, and alkaline phosphatase concentrations. The 25(OH)D concentration was determined by the chemiluminescence immunoassay (CLIA) method (Access2 kits of Beckman Coulter Co). World Health Organization definitions were used for exclusive breastfeeding and predominant breastfeeding. 20 The insufficiency and deficiency of vitamin D was labeled at serum 25(OH)D levels <20 ng/mL and <11 ng/mL, respectively. 21 Digital X-rays of both wrist joints of the infants were taken at the age of 6 months for radiological evidence of rickets.
Outcome
Maternal serum and cord blood concentrations of 25(OH)D were measured at recruitment; in infants 25(OH)D concentration was measured again at 6 months. The number of infants with hypovitaminosis D [25(OH)D <11 ng/mL] was compared in two groups of mothers supplemented with or without vitamin D3 at 6 months of age. Similarly incidence of biochemical and radiological rickets was recorded in these infants at 6 months of age.
Sample size
The number of subjects was based on the study entitled, “Vitamin D status of term exclusively breast-fed infants and their mothers from India.” 2 In this study, 44.33% of exclusively breastfed infants were found to have 25(OH)D levels <11 ng/mL at the age of 6 months. Assuming that of them 50% exclusively breastfed infants (22%) would have serum 25(OH)D levels >11 ng/mL at 6 months of age if their mothers were supplemented with 240,000 IU of vitamin D3 in the postpartum period and considering power of study as 80% and α error of 5%, it was revealed that recruitment of 56 mother–infant pairs each in the intervention and control group would achieve the desired objective. Assuming an attrition of 15% mother–infant pairs over a follow-up period of 6 months, 66 mother–infant pairs were recruited in each group.
Statistical analysis
Paired t-test was used to compare pre- and postserum 25(OH)D concentration, and unpaired t-test was used to compare serum 25(OH)D concentrations between two groups. With the help of repeated-measures analysis of variance, the gain in the weight, length, head circumference, chest circumference, and size of the anterior fontanelle were compared. Chi-square test was used to compare mode of delivery, gestation, parity, diet and dressing habit of the mother, and gender, number of infants with rickets, and having 25(OH)D concentration <11 ng/mL, ≥11 ng/mL, <20 ng/mL, and ≥20 ng/mL in both the groups.
Analysis of covariance was used to find a relationship between vitamin D supplementation and outcome after controlling for potential confounders like birth weight, baseline maternal and infant 25(OH)D concentration, and total sun exposure. Mean difference and 95% confidence intervals were presented. For correlation between 25(OH)D concentration and various parameters the Spearman's ρ was used. Baseline 25(OH)D concentrations were divided according to two criteria, <20 ng/mL (vitamin D insufficiency) and <11 ng/mL (vitamin D deficiency). Generalized estimating equation was applied to adjust the confounders; birth weight, maternal serum 25(OH)D concentration, and total sun exposure using Poisson log link function and unstructured covariance structure. Relative risk of 25(OH)D concentration <20 ng/mL and <11 ng/mL as compared with control group were estimated from this model. Value of p < 0.05 was considered significant. Software SPSS 20 was used for statistical analysis.
Definition
Exclusive breastfeeding
“Exclusive breastfeeding” is defined as no other food or drink, not even water, except breast milk (including milk expressed or from a wet nurse) to the infant till 6 months of life, but allows the infant to receive oral rehydration solution (ORS), drops and syrups (vitamins, minerals, and medicines). 20
Predominant breastfeeding
“Predominant breastfeeding” means that the infant's predominant source of nourishment has been breast milk (including milk expressed or from a wet nurse). However, the infant may also have received water and water-based drinks, fruit juice, or ritual fluids. 20
Biochemical rickets
Serum alkaline phosphatase ≥420 IU/L*
Hypovitaminosis D 21
Vitamin D deficiency: <11 ng/mL
Vitamin D insufficiency: <20 ng/mL
Vitamin D sufficiency: ≥20 ng/mL
Results
A total of 132 mother–infant pairs were recruited at birth, comprising 66 mother–infant dyads in each group. Finally, 115 infants completed the follow-up until 6 months of age. Loss to follow-up was 8 and 9 pairs of mother and infant in the intervention and control groups, respectively. However, one infant was excluded from the control group because of mixed feeding and 114 mother–infant pairs were finally analyzed (Figure 1). The study achieved the data of desired number of subjects; 112 mother–infant pairs were needed after 15% attrition rate following recruitment.
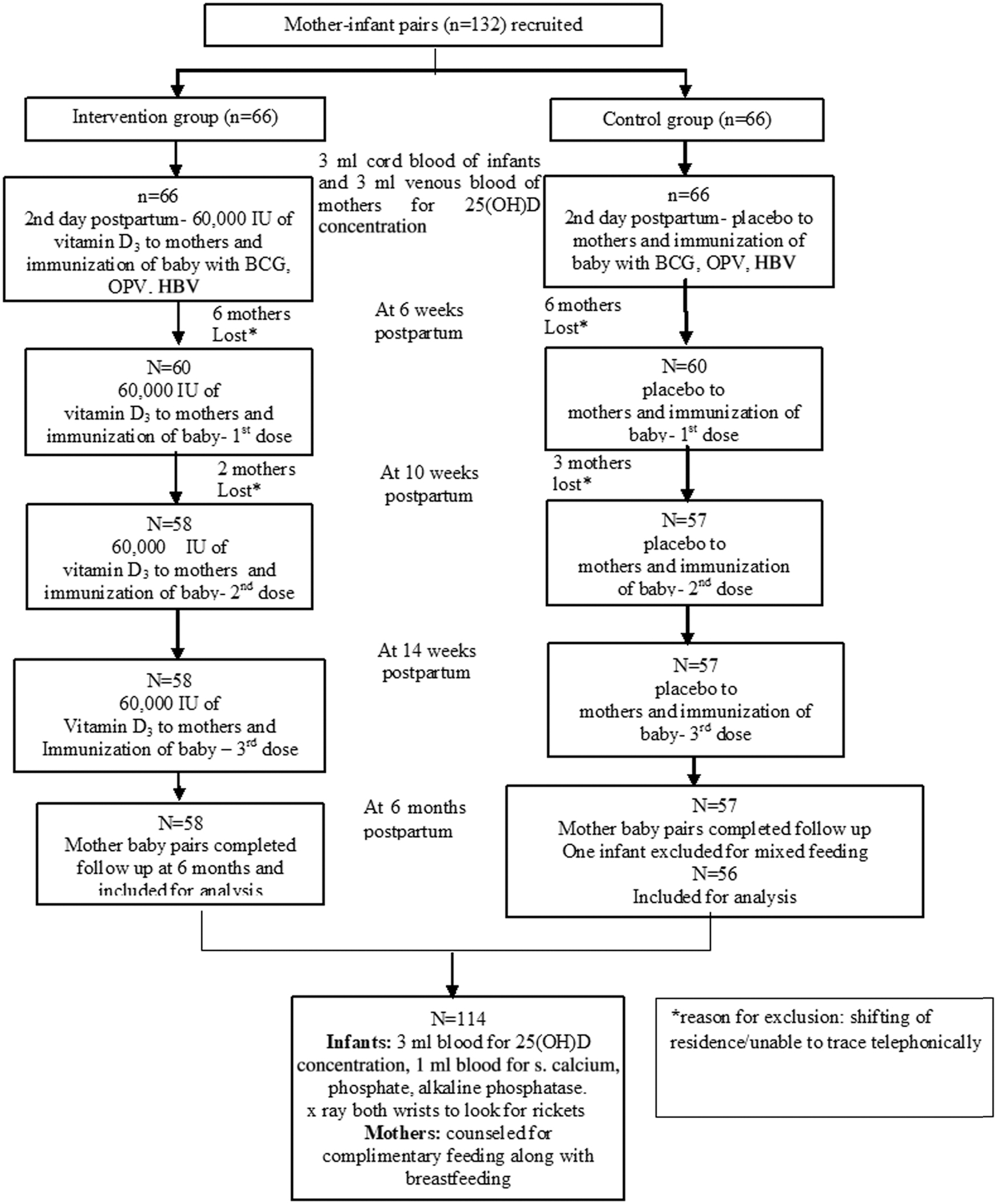
Flowchart of study.
All mothers were between 18 and 28 years of age and belonged to low- to middle-income group attending a tertiary care government teaching hospital in eastern part of Delhi. They were all Indians following different religions. The maternal characteristics, including dietary and dressing habits, and neonatal profile were similar in both groups (Table 1). Mean (SD) birth weight of the infants at birth in the intervention group [2,722 (257) g] and control group [2,765 (319) g] was similar. Mean (SD) sunlight exposure and sun index from birth to 6 months of age was 1.49 (1.32) hours and 1.88 (1.36) hours, and 0.86 (0.08) and 0.9 (0.07) in the intervention and control group, respectively, and were comparable.
Comparison of Baseline Characteristics of Mothers and Infants
Mean (SD).
BMI, body mass index.
At recruitment the serum 25(OH)D concentration was <20 ng/mL (vitamin D insufficiency) in all the mothers and 99.1% infants. A large number of mothers (90.4%) and their infants (88.6%) was indeed suffering from vitamin D deficiency [25(OH)D concentration <11 ng/mL]. The 25(OH)D concentrations in the cord blood were not normally distributed and application of the nonparametric Mann–Whitney U-test revealed a significant difference between the two groups. However, the cord blood 25(OH)D concentration in the control and intervention group was 6.0 (4.48) ng/mL and 6.89 (3.71) ng/mL, respectively, and was suggestive of gross vitamin D deficiency in the infants of two groups; hence, both the groups were similar in vitamin D status at recruitment (Table 2). The cord blood 25(OH)D concentrations were directly proportional to the serum 25(OH)D concentrations of the mothers (Spearman's rho 0.823). There was no correlation between the infants' 25(OH)D concentrations and duration of pregnancy, maternal weight, and body mass index.
Serum 25(OH)D Concentration in Mothers and Infants at Recruitment and in Infants at 6 Months of Age
p value by t-test.
p value by Mann–Whitney U-test.
IQR, interquartile range; SD, standard deviation.
At the age of 6 months a significant difference was observed between the mean (SD) serum 25(OH)D concentrations of the infants in the intervention (18.93 ± 5.12 ng/mL) and control groups (6.43 ± 3.76 ng/mL), respectively (p < 0.001) and the mean difference was 12.5 (95% CI = −10.80 to 14.17; p < 0.001) (Tables 2 and 3). In contrast to the control group, where all the infants had vitamin D insufficiency, only 60.3% infants had vitamin D insufficiency if their mother received vitamin D supplementation during lactation (p < 0.001) (Figure 2).
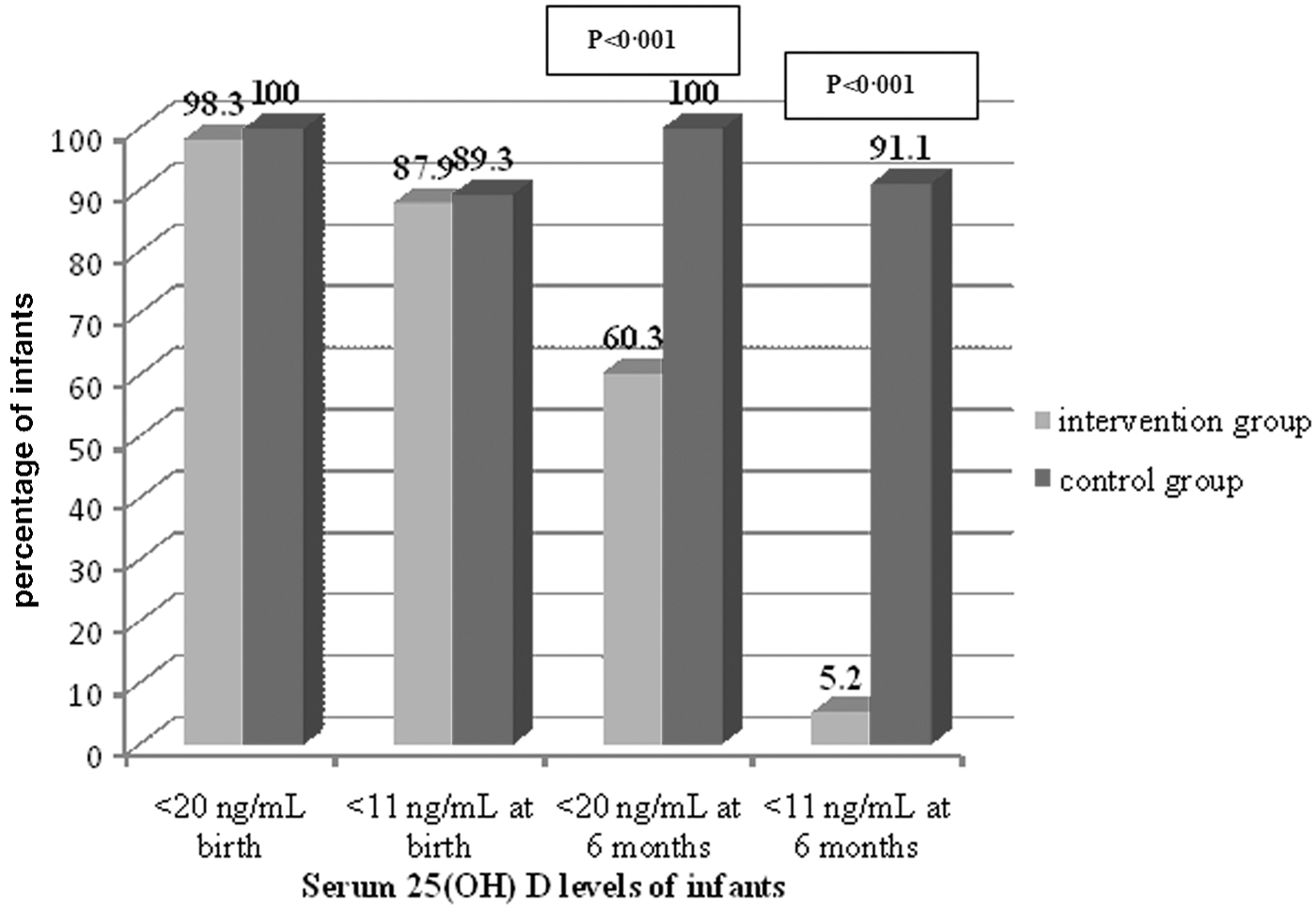
Percentage of infants with serum 25(OH)D levels <20 ng/mL and <11 ng/mL at birth and 6 months.
Serum 25(OH)D Levels in Infants at 6 Months of Age After Adjustment for Variable
Adjusted birth weight of the infant, mother's vitamin D levels at recruitment, total sun exposure (hours).
p value by Student's t-test.
Adjusted for baseline vitamin D difference at 6 months between the groups 13.12 (95% CI = 11.81–14.42) (analysis of covariance).
Significant difference in the serum 25(OH)D concentrations between the groups was maintained even after the adjustment for independent variables affecting serum 25(OH)D concentrations such as sun exposure, maternal serum 25(OH)D concentrations at recruitment, and birth weight (p < 0.001) (Table 3).
Against 5.2% infants in the intervention group, 91.1% infants in the control group had serum 25(OH)D concentration <11 ng/mL at the age of 6 months (Figure 2). A generalized estimating equation using Poisson log link function and unstructured covariance structure was applied to the confounders—birth weight, and mother's 25(OH) D concentrations and total sun exposure. It estimated that the risk of having serum 25(OH)D concentration <11 ng/mL and <20 ng/mL decreased by 94.6% (RR = 0.054; 95% CI = −0.018 to 0.161) and 48.1% (RR = 0.519; 95% CI = −0.485 to 0.735), respectively, in the exclusively breastfed infants of the mothers supplemented with vitamin D3 during lactation.
Six infants in the control group developed biochemical rickets at 6 months of age, and there was neither any relationship with the cord blood 25(OH)D nor with the maternal 25(OH)D concentrations at recruitment. No infant in the intervention group suffered from biochemical rickets. One infant in the intervention group and two infants in control group developed radiological rickets at 6 months of age.
Vitamin D supplementation to the breastfeeding mothers was safe. No infant suffered from clinical evidence of hypercalcemia like poor feeding, lethargy, polyuria, vomiting, constipation, seizures, and hypotonia as a result of vitamin D toxicity when mothers received oral bolus vitamin D3. Serum calcium and phosphorus concentrations were within normal limits at 6 months of age.
Discussion
A large numbers of pregnant and lactating women are suffering from vitamin D deficiency in the temperate and sunshine abundant countries.22–25 Several studies from India and other Asian countries in the past 10 years have also reported vitamin D deficiency in the majority of parturient women and lactating mothers and their infants.2,4,6,16,24 A German study has revealed that breastfeeding women have 4.0-fold higher risk (95% CI = 1.8–8.7) for vitamin D deficiency than nonpregnant nonbreastfeeding women and that the risk of vitamin D deficiency is higher in the winter and spring months. 25
The current randomized double-blind placebo-controlled trial reaffirmed the worst scenario that 90.4% mothers and 88.6% infants were found suffering from vitamin D deficiency at birth and that low 25(OH)D concentrations in the mothers reflected on the vitamin D store of the infants.
A newborn infant acquires vitamin D from the mother by two mechanisms. First, vitamin D stores are built-up during the intrauterine life26,27; the cord blood 25(OH)D concentrations are directly proportional to the maternal serum 25(OH)D concentrations.28–30 The cord blood 25(OH)D concentration is equal to or up to 20% lower than the maternal serum concentration. 29 It has also been seen that maternal 25(OH)D concentration has positive correlation with the infant's 25(OH)D concentrations even at 6 weeks, 3 months, and 6 months of age. 2 Subsequently an infant obtains vitamin D through breast milk. The anti-rachitic activity in the breast milk is directly proportional to the maternal vitamin D stores. 7
The third source of vitamin D supply to an infant is its synthesis under sunlight. It has been observed that newborns and infants are not adequately exposed to sunlight. A vitamin D-deficient pregnant mother will not be able to provide adequate vitamin D stores to the infant before birth. Vitamin D deficiency during lactation will further compromise the anti-rachitic activity in the breast milk. If the mother is vitamin D deficient then breast milk alone will not be able to maintain adequate vitamin D concentrations in an exclusively breastfed infant.7,31 It has been proved that breast milk vitamin D concentration increases when a mother is supplemented with vitamin D during lactation.18,32 Each 100 IU increase in the maternal vitamin D intake during lactation increases the infant's serum 25(OH)D concentration by 0.36 ng/mL. 5
Dawodu et al. found that 61% of the mothers and 82% of the infants had severe hypovitaminosis D and justified administration of vitamin D to the breastfeeding infants. 33 Many studies have reported that exclusively breastfed infants suffer from nutritional rickets if they are not supplemented with vitamin D since birth.19,27 Indian studies have reported nutritional rickets in the breastfed infants from 16.49% to almost 33% at 6 months of age.2,34 Challa et al. further stated that neonates, who were exclusively breastfed during the first 6 months of life, were in need of vitamin D supplementation irrespective of the season even in a sunny country like Greece where foods were not supplemented with vitamin D. 35
In our study mothers were supplemented with 240,000 IU of vitamin D in bolus doses over a period of 14 weeks in the intervention group, which was equivalent to approximate daily dose of 2,449 IU. It was found to be safe and resulted in almost 85% reduction in the number of children with vitamin D deficiency compared with the infants of vitamin D unsupplemented mothers. None of the children of the vitamin D supplemented mothers suffered from biochemical rickets. Radiologic rickets does not manifest until weeks of nutrient deprivation and therefore not a good assessment of what is going on at the molecular/biochemical level. Maternal supplementation of vitamin D thus prevents development of severe vitamin D deficiency and eventually rickets. However, 60.3% infants still showed vitamin D insufficiency in the study. It was possible that maternal vitamin D stores were not maintained in the absence of adequate dietary intake and/or sun exposure after the last bolus dose of vitamin D3 given to them at 14 weeks postpartum; the t½ of 25(OH)D is 15 days.
Many researchers have worked to find out the appropriate dose of vitamin D required during lactation to replenish vitamin D stores of both the mothers and infants. Ala-houhala et al. found that daily supplementation of 2,000 IU vitamin D to the lactating mothers raised serum 25(OH)D of the infants to sufficient concentration that was comparable with daily 400 IU vitamin D supplementation to the infants, whereas daily 1,000 IU vitamin D supplementation was not able to raise the infants' 25(OH)D concentrations. 36 Hollis et al. have reported in a larger cohort of mother–infant pairs that a dose of vitamin D3 as high as 6,400 IU/day to lactating mothers for 6 months was safe and raised infants' serum 25(OH)D concentrations significantly and that it was comparable with daily vitamin D supplementation of 400 IU to the late preterm and term infants. 37 Recently, Dawodu et al. reported that maternal vitamin D supplementation of 6,000 IU/day was safe and maintained adequate infants' 25(OH)D concentrations that was equivalent to maternal vitamin D supplementation of 600 IU/day along with 400 IU/day vitamin D administration to the infants. They also found that maternal serum vitamin D concentrations and breast milk vitamin D contents were significantly higher when lactating women were supplemented with higher doses of vitamin D. 32
High-dose vitamin D supplementation was found safe in various studies. Prasanna et al. supplemented lactating mothers with oral 600,000 IU of vitamin D3 or placebo over a period of 10 days and showed that it was safe. 16 They clinically monitored and measured urinary calcium and creatinine ratio in the mothers and infants at 14 weeks and 6 months. The urinary calcium:creatinine ratio was <0.5 in all the subjects, well below safe limit of <2; there were no signs and symptoms of hypercalcemia in either mothers or infants. 16
Hollis et al. and Dawodu et al. have also concluded that high-dose oral administration of vitamin D to the breastfeeding mothers is safe to them and to their infants.32,37 In a recent double-blind placebo-controlled study, Roth et al. administered vitamin D weekly to women in the prenatal period in the doses of 4,200, 16,800, and 28,000 IU with one group of pregnant women receiving 28,000 IU up to 26 weeks postpartum. 38 There was dose-dependent effect on the maternal serum, cord blood, and infant serum 25(OH)D concentrations till 1 year of age. Documented asymptomatic hypercalcemia was seen in 0.7% postpartum women and 0.7% infants at 6 months and the frequencies were not different across groups. Calciuria (uCa:Cr ratio >1 on two occasions) was seen in two women only. None of the mothers developed nephrolithiasis. Infants with documented asymptomatic hypercalcemia did not suffer from serious illness. Administration of higher doses of vitamin D to pregnant and lactating women is safe. We administered four bolus doses of vitamin D to the lactating mothers, at the time of primary immunization of the infants, amounting to 2,449 IU daily, which was safe and acceptable.
Other studies have shown that intermittent supplementation to mothers with high-dose vitamin D is equally effective as daily low-dose supplementation in raising 25(OH)D to sufficient concentrations in infants and is better in terms of compliance. Oberhelman et al. in a randomized-controlled trial concluded that a single dose of 150,000 IU vitamin D to lactational mothers was safe and equally effective to daily supplementation of 5,000 IU for 28 days in raising the 25(OH)D concentrations in the infants. 17 There can be an issue on bolus versus daily administration of vitamin D to the mothers, that similar rise in the serum 25(OH)D concentrations after two strategies is reflected at the cellular level and whether the safety profile is same. This aspect needs more research.
Although 60% and 5.2% infants in our study were still showing vitamin D insufficiency and deficiency, respectively, at 6 months of age after 240,000 IU vitamin D supplementation to their mothers, the concept, feasibility, and acceptability of the vitamin D supplementation seems to be novel and exciting. This approach of vitamin D supplementation to the mothers can be included in the health care delivery system. The mother can be given vitamin D sachet/tablet (60,000 IU) in the immunization clinic while infant is being administered vaccines; first dose of vitamin D3 at the time of BCG, OPV, and HBV0 dose administration and three subsequent doses of vitamin D3 at the time of first, second, and third dose of pentavalent vaccine and OPV/IPV administration.
The limitations of the study were that exact dose and duration of the vitamin D supplementation to the mother could not be determined and maternal serum and breast milk 25(OH)D concentrations were not measured 6 months after vitamin D supplementation. Future studies are required with higher dose and/or prolonged duration of vitamin D supplementation to lactational mothers that can completely abolish vitamin D insufficiency state in the exclusively breastfed infants. Vitamin D supplementation during pregnancy or infancy has modulatory effect on the immune functions of the infants but its evaluation is beyond the scope of the trial. The strength of the study was that adequate number of children were recruited based on the study conducted on the similar population; it was a randomized double-blind placebo-controlled trial, and the estimation of 25(OH)D was carried out by a sensitive CLIA method. The ethical dilemma of supplementing only baby and leaving mother in a vitamin D-deficient state was also not there.
Conclusion
Serum 25(OH)D concentrations of exclusively breastfed infants rose significantly at 6 months of age when their mothers were orally supplemented with 240,000 IU of vitamin D3 during lactation in comparison with the infants of vitamin D unsupplemented mothers with 94.6% and 48.1% reduction in the risk of hypovitaminosis D [25(OH)D levels <11 ng/mL] and vitamin D insufficiency [25(OH)D levels <20 ng/mL], respectively.
Only 5.2% infants had 25(OH)D concentration <11 ng/mL when their mothers received vitamin D3 during lactation compared with 91.1% infants whose mothers were not supplemented. Maternal supplementation with vitamin D3 also reduced the risk of biochemical rickets in the infants at the age of 6 months.
Footnotes
Authors' Contributions
M.T.: data collection, figures, literature search, writing; M.M.A.F.: concept, study design, monitoring, literature search, figures, data, interpretation, writing; A.A.: study design, literature search, figures, data interpretation, writing; S.V.M.: writing, lab support; R.K.M.: data analysis, writing.
Acknowledgment
Zuventus Healthcare Ltd., Mumbai, provided vitamin D sachets (Vitanova®) and placebo.
Disclosure Statement
Authors declare no conflicts of interest.
Funding Information
The Breastfeeding Promotion Network of India supported this trial by providing funds (Grant No. BPNI/2016 dt; December 4, 2016) to purchase 25(OH)D measuring kits.