
Abstract
Background:
In France, the proportion of children who are exclusively breastfed has been decreasing in recent years. The aim of the study is to assess the link between quality of life (QOL) in pregnant women from the first trimester to the end of pregnancy using the French version EQ5D-3L questionnaire and the feeding method at birth (breast or bottle).
Materials and Methods:
Five hundred pregnant adult women were monitored between 2015 and 2017 at the Toulouse University Hospital (France). The data were collected monthly. After analyzing the QOL (EQ-5D-Index) and health status (EQ-5D-Visual Analogue Scale) for 1 month, we carried out a nine-group category analysis based on their QOL in the third month (low QOL [score <0.50 out of 1], intermediate [score between 0.50 and 0.90 out of 1], or high [score ≥0.90 out of 1]) and then based on changes in their QOL between the third and eighth month [marked reduction (low >0.6 point), intermediate (low between 0.1 and 0.6 point), and slight reduction (low <0.1 points increase)].
Results:
Around1,847 questionnaires were collected and analyzed from 500 women. The monthly analysis did not highlight any link between QOL or health status reported during pregnancy and the feeding method at birth. As regard to the category analysis, following adjustment, the logistic regression model shows that breastfeeding is not linked to QOL in the third month of pregnancy (p = 0.171) or to changes in QOL during pregnancy (p = 0.426). However, there is less of a tendency to breastfeed in individuals with a high QOL in the third month of pregnancy compared to an intermediate QOL during the third month of pregnancy (p = 0.06).
Conclusion:
In this cohort of pregnant women for whom QOL was assessed throughout pregnancy, no link between QOL and feeding method was highlighted.
Introduction
Breastfeeding is defined by the Haute Autorité de Santé (French Health Authorities) and the World Health Organization (WHO) as “the feeding of a newborn infant or baby with its mother's milk. Feeding is exclusive when the newborn infant or baby receives only breast milk or partial when it is combined with another feed.”1,2
Breastfeeding has numerous long- and short-term health benefits for both mother and baby. In addition to containing all of the nutrients a baby needs during the first 6 months of life, breastfeeding reduces the risk of infections in the middle ear, respiratory tracts, and intestines, as well as the risk of allergy in infants.3–6 In the longer term, it has also been shown to reduce the risk of children and adolescents being overweight and obese.7,8 In mothers, breastfeeding accentuates the bond between mother and child, allows faster weight loss, and reduces the risk of breast cancer in the long term.9–11 The benefits of breastfeeding depend on the duration of breastfeeding. 4 In France, the proportion of children receiving exclusive bottle feeding has increased considerably over the last 10 years, rising from 41% in 1995 to 66% in 2016.12,13
Self-confidence, support from family and partner, and socioeconomic status are crucial factors involved in opting for breastfeeding (breast) or bottle feeding (bottle). 14 These elements are also themes of the quality-of-life (QOL) questionnaires.15,16 QOL is defined by the WHO as “the way in which individuals perceive their position in life in the context of culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns.” 17 It is evaluated using standardized questionnaires such as the EUROQOL EQ-5D questionnaire. 18
Thus, within the context of promoting breastfeeding, it would be interesting to establish whether there is a link between the choice of feeding method (breast or bottle) at birth and QOL during pregnancy.
Methods
Study design and population
A prospective single-center cohort study comprising 500 women monitored throughout their pregnancy was carried out between 2015 and 2017 in the Maternity Unit at the CHU Toulouse (University Hospital Centre) (level 3 maternity unit, 5,000 deliveries each year). The pregnant women were enrolled in the study before the end of the first trimester (<15th week of pregnancy) during the initial follow-up consultation or during the first ultrasound by a midwife or obstetrician. The cohort comprised female adults with civil rights and a gestational age <15th week of pregnancy. They gave their informed consent after reading the information leaflet. Pregnant women who gave birth before the 37th week of pregnancy were excluded to maintain homogeneous groups.
Electronic questionnaire and endpoints
During the first trimester of pregnancy and then on a monthly basis up to birth, the pregnant women completed an electronic questionnaire on a secure online server (Lime Survey based in Germany) from their own homes (i.e., seven measurements were recorded for pregnant women who gave birth at full term). The questionnaires were encoded specifically for each pregnant woman. Pregnant women who failed to complete the monthly questionnaire were reminded by mail and then by telephone.
Each month, the QOL was assessed with the French EQ5D-3L questionnaire. This is a European questionnaire, validated in France and nonspecific to the pregnant population. It comprised five dimensions (mobility/ability to look after oneself/routine daily activities/pain-discomfort/anxiety-depression) with three levels of responses and a visual analogue scale (VAS, between 0 and 100) used to assess health status. Based on these five dimensions, the EQ-5D-3L can describe 243 possible states of health, which are transformed into a QOL score using the algorithm developed by Chevalier and de Pouvourville in 2013. 19 This EQ-5D score varies between −0.53 and 1 (1 being the best QOL possible).
During the first trimester, the questionnaire also included a collection of sociodemographic data from medical and obstetrical history. Medical information on pregnancy was collected monthly to categorize our women into three groups: “physiological pregnancy” (no medical problem during pregnancy), “simple pathological pregnancy” (occurrence of one or more conditions that did not require home monitoring or hospitalization) and “complex pathological pregnancy” (occurrence of one or more conditions that did require home monitoring and/or hospitalization). These conditions were chosen according to French High Authority of Health guidelines published in 2016 “Suivi et orientation des femmes enceintes en fonction des situations à risque identifiées” 20 The conditions listed were viral or bacterial infections, breakthrough bleeding, gestational diabetes, cholestasis, thrombocytopenia, preterm labor risk, hypertension, premature rupture of the amniotic sac, delayed intrauterine growth, and ultrasound malformation, in addition to renal, respiratory, thromboembolic, and psychopathological maternal disorders. For each disease, a definition was given to facilitate completion. Finally, a questionnaire relating to birth methods (date and method of birth) and the method chosen to feed the newborn infant (breast/combination/bottle) at birth was completed once after birth. Thus, women who had given labor feeding their newborn infant with breast milk, either exclusive or partial, and those who adopted bottle feeding with formula milk were assigned to the relevant groups based on the WHO definition of breastfeeding. 2
Pregnant women who completed several questionnaires on the same date or who had an unknown or dubious gestational age on birth were excluded from the analysis. All of the questionnaires completed after birth or those with misleading dates or completed at the wrong time were also excluded.
Statistical analysis
The general cohort characteristics were initially presented and compared according to the groups defined by the feeding method at birth (breastfeeding, either exclusive or combined, versus bottle feeding) using χ 2 tests or Fisher's exact tests in theoretically inadequate cohorts.
The QOL pathways in each of the groups defined by the feeding method at birth were then studied. The distribution of the EQ-5D Index, EQ-5D VAS scores, and the items in the EQ-5D Index are described during each month of pregnancy. The EQ-5D Index and EQ-5D VAS scores together with their variations between the third month and the eighth month of pregnancy (calculated as the difference between the score at 3 months and at 8 months) were categorized into three groups for the remainder of the analyses: the intermediate group between the values of the first and third distribution quartile in our sample, and the ranges (between the minimum and Q1 and between Q3 and the maximum) were considered.
Finally, an adjusted analysis was performed. The maternal QOL pathway during pregnancy is summarized by two characteristics: QOL at 3 months (divided into three groups 25%—50%—25%) and its variation between the third month and the eighth month (divided into three groups 25%—50%—25%), that is, nine groups overall. The ninth month of pregnancy was excluded from the analysis due to the low number of questionnaires collected as the majority of pregnant women had given birth before completing them. To establish whether this pathway had any bearing on the choice of feeding method at birth, we assessed a logistic regression model, the dependent variable for which was feeding at birth. The independent variables introduced into the model were QOL during the third month of pregnancy, changes in the QOL between the third and eighth month of pregnancy, the level of education, smoking during the first trimester of pregnancy, the body mass index (BMI) at the start of pregnancy, the onset of disease during pregnancy (physiological/pathological pregnancy), and the delivery method (vaginal delivery/Caesarean section).
Results
Study population
Our cohort comprised 2,991 questionnaires collected from 500 out of 644 pregnant women approached, that is, an inclusion rate of 79.6%. After excluding pregnant women with an unknown or dubious gestational age at birth, or who had given birth prematurely (<37th week of pregnancy), and excluding questionnaires completed outside the fixed deadlines, our cohort comprised 1,847 questionnaires corresponding to 332 pregnant women (Fig. 1). Three hundred thirty-two patients were therefore selected for the final analysis. Among these, 235 pregnant women (70.8%) stated that they fed their child at birth (breastfeeding—exclusive or combination) and 97 bottle-fed their babies (29.2%).
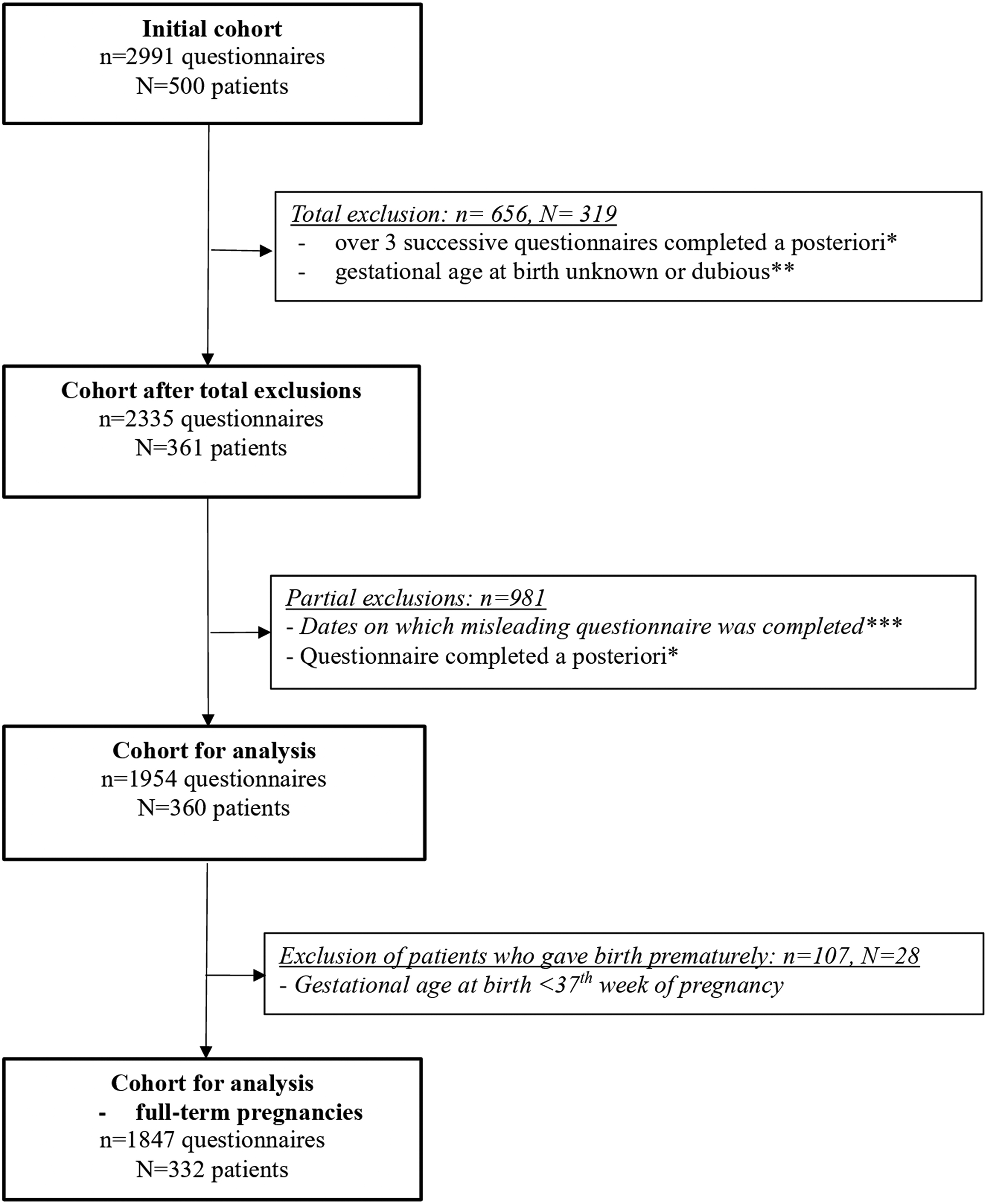
Study flowchart. * more than 15 days after the month of pregnancy; ** lost to follow-up or missing data; *** before or after pregnancy.
Table 1 describes the characteristics of pregnant women monitored during pregnancy and who gave birth at full term. Most of the women were younger than 35 years (78.9%), Caucasian (91.6%), and lived in an urban environment (66.2%). A BMI >25 (27.7% breast versus 48.4 bottle, p < 0.001), smoking (8.9% breast versus 21.7% bottle, p = 0.002), single at the start of pregnancy (2.6% breast versus 8.3% bottle, p = 0.031), no antenatal classes (83.4% breast versus 72.2% bottle, p = 0.02), and a Caesarean section (13.6% breast versus 31.3% bottle, p < 0.001) were significantly associated with a higher frequency of bottle feeding.
Description of Cohort Included According to Type of Pregnancy: Sociodemographic Characteristics, Medical and Obstetric History, and Obstetric Data Relating to the Current Pregnancy of the Patients Enrolled in the Study (n = 332)
Fisher's exact test.
“Physiological pregnancy”: no medical problem during pregnancy, “pathological pregnancy”: onset of one or more diseases (viral or bacterial infections, metrorrhagia, gestational diabetes, cholestasis, thrombopenia, threat of premature labor, hypertension, premature rupture of membranes, delayed intrauterine growth, malformation on ultrasound scan, and also maternal renal, respiratory, thromboembolic, and psychopathological disorders).
NA, nonapplicable; BMI, body mass index.
Link between feeding at birth and QOL (EQ5D-Index) during pregnancy
The study of median QOL values during each month of pregnancy in pregnant women choosing breastfeeding shows a more stable pathway from the third to the fifth month of pregnancy at 0.8 point (n = 198 observations at the third and fifth month) followed by a marked reduction up to the seventh month of pregnancy (−0.43 point) (n = 195 observations in the seventh month), and finally renewed stabilization up to the eighth month of pregnancy at 0.37 point (n = 198 observations). In the bottle-feeding group, QOL seems to decrease overall during pregnancy: the median QOL is 0.89 point (n = 77 observations during the third month), versus 0.37 point in the eighth month of pregnancy (n = 80 observations).
Regardless of the feeding method chosen, no significant difference was observed between our two groups in the third (p = 0.673) and eighth month (p = 0.788), especially due to the significant dispersion in the QOL score each time (e.g., 0.61 point in the sixth month for the bottle-fed and breastfed group) (Table 2).
Description of Quality-of-Life (EQ-5D-Index) and Health Status (EQ-5D-VAS) According to Gestational Age and Feeding Method at Birth (n = 332)
Median (IQR): first quartile and third quartile.
SD, standard deviation; IQR, interquartile range; VAS, visual analogue scale.
The deviation in QOL between the third and eighth month of pregnancy was calculated for the 229 pregnant women for whom the EQ-5D scale was completed in the third and eighth month of pregnancy (i.e., 69% of the cohort). This subcohort differed from our overall population solely in terms of level of employment at baseline (the comparison focused on all the variables used to describe the population [variables in Table 1]).
The lowest breastfeeding figure (54.6%) was recorded in the group of pregnant women with a low QOL (<0.50) during the third month combined with a slight reduction (low between 0 and 0.1) or increase in the QOL between the third and eighth month. Following adjustment, no significant correlation between breastfeeding and QOL was apparent during the third month of pregnancy (p = 0.171), and there were no changes in QOL during pregnancy (p = 0.426). However, there was less of a tendency to breastfeed by pregnant women with a high QOL during the third month of pregnancy (71%) compared to those with an intermediate QOL in the third month of pregnancy (78%) (p = 0.06) (Table 3).
Results of the Logistic Regression Models Explaining the Probability of Breastfeeding Depending on Quality-of-Life (EQ-5D-Index) and Health Status (EQ-5D-EVA) (n = 228)
Adjustment according to the following: level of education, BMI at baseline, smoking during the first trimester of pregnancy, medical problem during pregnancy, and delivery method.
VAS, visual analogue scale; OR, odds ratio; CI, confidence interval; BMI, body mass index.
On independent analysis of the five dimensions that make up the EQ-5D index, a global comparable change was apparent between the breastfeeding group and the bottle feeding group. The proportion of pregnant women who reported no problems walking gradually decreased, falling from 89.4% in the third month (n = 198 observations) to 33.3% in the eighth month (n = 198 observations) and ninth month (n = 141 observations) in the breastfeeding group versus 80.5% (n = 77) to 26.3% in the eighth month (n = 80) and then 26.1% in the ninth month (n = 46) for the bottle feeding group. In terms of independence, virtually all of the pregnant women were said to be independent in the third month, regardless of feeding method, versus 63.6% for the breastfeeding group and 62.5% for the bottle feeding group in the eighth month of pregnancy. The implementation of routine daily activities was almost identical for each group in the third month at ∼69% and low in the eighth month at 17.2% in the breastfeeding group compared to 16.2% in the bottle feeding group. The proportion of pregnant women who said they felt slightly or very concerned and depressed was stable throughout pregnancy at ∼40% in each group. The number of pregnant women reporting pain/discomfort increased at the start of pregnancy with a value of 63% being recorded in both groups. Similar findings were noted up to the ninth month with 87% being recorded in both groups. In the group of women who gave birth before completing their ninth month questionnaire, a favorable change in scores relating to mobility, independence, and implementation of daily tasks was recorded in the breastfeeding group between the eighth and ninth month, whereas these scores continued to fall in pregnant women who opted for bottle feeding (Fig. 2).
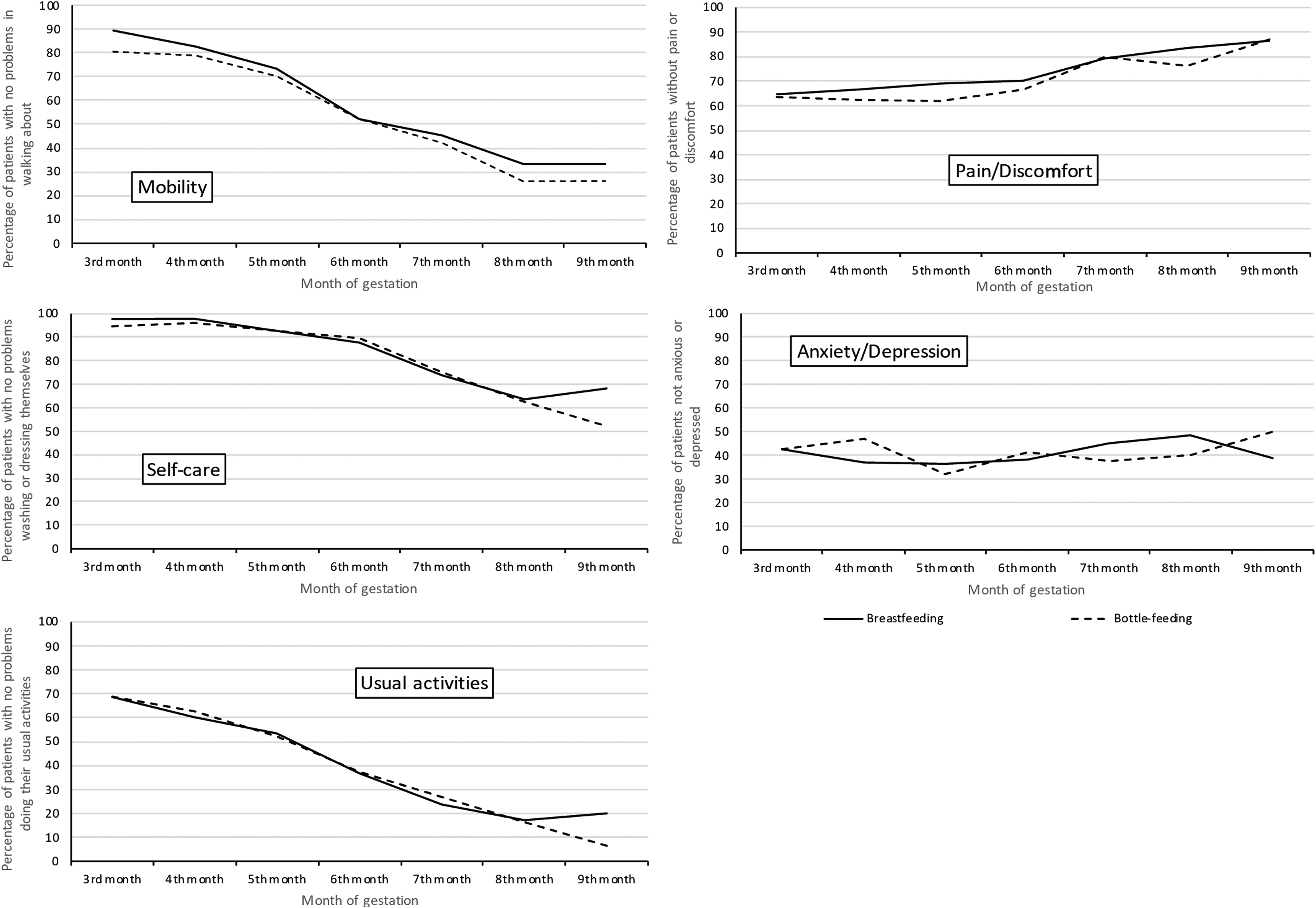
Description of five dimensions in the quality-of-life score (EQ-5D-Index) depending on feeding method at birth (n = 332). Questionnaires per month: 3rd month N = 198 (Breast) N = 77 (Bottle); 4th month N = 189 (Breast) N = 77 (Bottle); 5th month N = 209 (Breast) N = 84 (Bottle); 6th month N = 193 (Breast) N = 75 (Bottle); 7th month N = 195 (Breast) N = 85 (Bottle); 8th month N = 198 (Breast) N = 80 (Bottle); 9th month N = 141 (Breast) N = 46 (Bottle).
Link between feeding at birth and VAS during pregnancy
In the third month of pregnancy, the median VAS score was identical in both groups (median = 85 and interquartile range = 75–90), thereafter falling overall at the same time between both groups up to the seventh month of pregnancy with a slightly greater reduction being recorded in the breastfeeding group compared to the bottle feeding group (median score of 75 versus 80 in the seventh month). From the seventh to the ninth month, values stabilized in the breastfeeding group, exceeding figures recorded in the bottle feeding group (median of 75 versus 70) (Table 2).
The pregnant women were then regrouped according to their VAS score during the third month (three groups) and then according to changes in their VAS score (three groups) between the third and eighth month (i.e., nine groups). Thus, in the third month, the pregnant women were categorized as follows: low VAS (<76), intermediate between 76 and 90), and high (≥91), and then between the third and eighth month as follows: marked reduction (low >17 points), intermediate (low between 0 and 17 points), and slight (low between 0 and 1 or increase). Following adjustment, the VAS in the third month, regardless of changes between the third and eighth month, did not significantly affect the choice of feeding method at birth (Table 3).
Discussion
Our study did not highlight any link between QOL or health status reported during pregnancy and the feeding method at birth. After adjustment, breastfeeding was not associated with QOL in the third month of pregnancy (p = 0.171) or with changes in QOL during pregnancy (p = 0.426).
To our knowledge, this is the first study to focus on the impact of QOL on feeding method at birth in pregnant women in France. In a review of the bibliography published in 2017, no QOL for the French population publication addressed the issue of breastfeeding. The main subjects studied were pathological pregnancies and, in particular, depression problems. 21
As in the 2014 Etude Longitudinale Française depuis l'Enfance study, the proportion of women who fed their babies was significantly lower in the case of obesity (p < 0.001), single status of the mother (p = 0.03), medical history before pregnancy (p = 0.01), no antenatal classes (p = 0.02), smoking (p = 0.002), and Caesarean section (p < 0.001).22,23
In both groups, a decrease in QOL during pregnancy was observed only between the fifth and seventh month in the breastfeeding group compared to a progressive decrease throughout pregnancy in the bottle feeding group.
However, the main factors acknowledged as influencing the method of feeding are all featured in the dimensions investigated in the QOL questionnaires, that is, the physical dimension, psychological dimension, social/relational dimension, and the financial dimension. These factors include obesity, self-confidence, support from family and partner, and socioeconomic status.15,16 Beyond a lack of power, we have not perhaps succeeded in highlighting a significant link due to the choice of the EQ5D questionnaire, which is potentially too general and does not broach some dimensions of QOL such as social support. Furthermore, it focuses only on one item of psychological wellbeing, combining anxiety and depression. 24 Indeed, each QOL questionnaire targets different subjects for each dimension. The EQ-5D-3L questionnaire is based on the following dimensions: mobility (problem in moving around), independence (problems taking care of oneself), routine daily activities (problem with work, studies, domestic chores, leisure activities, etc.), pain (pain or discomfort), and anxiety (being anxious or depressed). Thus, the choice of another questionnaire, such as the WHOQOL or SF36 questionnaire, for instance, may be an interesting alternative.15,25
In the literature, several studies have highlighted a link between antenatal QOL and breastfeeding. In 2014, Mortazavi et al. 26 confirmed that the QOL scores evaluated during the third trimester of pregnancy using the WHOQOL-BREF questionnaire in a cohort of 358 women in north-eastern Iran were significantly linked to breastfeeding difficulty scores at 4 weeks postpartum. The mothers with poor QOL were more likely to experience difficulties feeding shortly after giving birth. Conversely, women who perceived their QOL to be “good” or “very good” recorded lower scores for feeding problems. 26 This study adopted the same approach that was carried out in 2011 in Brazil, highlighting a link between successful breastfeeding and QOL following childbirth. 27
In addition to a monthly global QOL analysis, the category analysis based on QOL during the third month and any change throughout pregnancy seems of clinical interest. In fact, since the pregnant women’ QOL varied considerably from the third month and changes during pregnancy differ significantly between pregnant women, a subgroup analysis would provide a more precise analysis. Even if there is less of a tendency to breastfeed in pregnant women with a strong QOL in the third month, (p = 0.06), changes in their QOL during pregnancy may reflect changes (loss of independence, anxiety, etc.) likely to affect their choice. An analysis of a larger pregnant woman cohort might reveal a link.
Our study has several limitations. First, we only had a small cohort, especially since the subgroup analyses generated a lack of power. The number of pregnant women choosing to breastfeed in our study (70.8%) is slightly higher than that observed in the last Enquête National Périnatale française (French National Perinatal Survey) conducted in 2016 (66%).13,28 Nevertheless, this figure is close to that published in 2017 on the health status of the French population, with a figure of 69.5% being recorded in the department of la Haute-Garonne. 29 Moreover, this was a single-center study with a potential selection bias because recruitment was carried out by midwives for patients who were committed to good study compliance. However, the use of the French version of the EQ5D-3L questionnaire generated a single validated QOL score adapted specifically for the French population.18,19,30 These are the first data that will have to be rechecked with other specific questionnaires, particularly for obese and depressed patients, which are known factors in reducing QOL and are also associated with the probability of breastfeeding. The use of an electronic questionnaire completed online by pregnant women in their own homes, limits the information bias as the pregnant women were not exposed to any third-party influence on completing their questionnaires.31–33 For future studies, it would be interesting to ask pregnant women about their feeding choices on a monthly basis, in conjunction with the QOL questionnaire, to investigate changes in the method chosen and any correlation with QOL.
Conclusion
In conclusion, neither QOL (EQ5D-index) nor VAS (EQ5D-VAS) during pregnancy appears to affect the feeding method selected at birth. A more powerful study would be required to confirm or refute these data.
Ethical Approval
This study received a favorable opinion from the Ethics Committee for Research in Obstetrics and Gynaecology in France on March 3, 2015 (opinion number CEROG OBS 2015-01-02).
Footnotes
Acknowledgments
We would like to thank the French-speaking Mother-child Network of (Réseau Mère-Enfant de la Francophonie) for its support in carrying out this study.
Disclosure Statement
M.M., O.C., C.D., L.M., Y.M., V.E., and C.V. contributed in the design of the study. M.M., A.F., and A.D.P. contributed the data collection, and M.M., V.E., and C.V. analyzed and interpreted the data. M.M. and C.V. drafted the article. O.C., C.D., L.M., Y.M., and C.V. made a critical revision of the manuscript.
No competing financial interests exist.
Funding Information
This study received funding from the Réseau Mère-Enfant de la Francophonie as part of a research grant.