
Abstract
Objective:
The aim of this study was to evaluate the association between possible covariates, with emphasis on maternal body mass index (BMI), on exclusive breastfeeding and on total breastfeeding during the first postnatal year.
Design:
A longitudinal study encompassing 723 women who were followed during the first postnatal year
Methods:
Data concerning pregnancy, delivery, neonatal period, and breastfeeding were extracted from respective medical records. Sociodemographic data on the participants were self-reported. The Cox Proportional Hazard Model was used for investigating the effects of different covariates.
Results:
Compared with women with BMI <25.0, obese women ran a higher risk of ceasing exclusive breastfeeding prematurely (Hazard ratio [HR] = 1.38, p = 0.009). Multiparous women had a lower risk of ceasing the exclusive breastfeeding prematurely, than primiparous women (HR = 0.78, p = 0.009). Concerning exclusive breastfeeding as well as total breastfeeding, the risk of prematurely ceasing the breastfeeding decreased with increasing age (p = 0.028 and p ≤ 0.001, respectively).
Median duration of exclusive breastfeeding was shorter among obese women compared with women with BMI <30.0 (3.0 months versus 6.0 months). Corresponding figures for total breastfeeding were 4.0 months versus 8.0 months. Concerning parity and exclusive breastfeeding, there was no difference in median duration between primiparous women and multiparous women (4.0 months), whereas multiparous women had a longer median duration of total breastfeeding, than primiparous women (8.0 months versus 7.0 months).
Conclusion:
The risk of ceasing exclusive breastfeeding prematurely is high among obese women. This result indicates the need for targeted supportive interventions, individualized according to BMI. With increasing age, the risk of ceasing breastfeeding prematurely decreases, and compared with primiparous women, multiparous women run a lower risk of ceasing exclusive breastfeeding prematurely.
Introduction
Breastfeeding is considered as a natural choice for most women. It provides the child with adequate nutrients for growth and development and several studies have reported short- and long-term health benefits for the child as well as for the woman.1–3 Moreover, breastfeeding provides economic and environmental advantages to society. 4 According to the recommendation of the World Health Organization (WHO), which has been accepted by many countries, including Sweden, the child should be exclusively breastfed during the first 6 months of life. Continued breastfeeding, along with appropriate complementary food is proposed during the first 2 years of life, or for as long as the parents and child wish. 5 Despite the recommendation from the WHO and the knowledge about the benefits of breastfeeding, the goal of continued breastfeeding is not often reached by many countries and also by Sweden.6,7 Among children 6 months of age, only 14% were exclusively breastfed, whereas just over 50% were partially breastfed in Sweden in the year 2016. 7
Maternal obesity has been reported to have a negative impact on breastfeeding. In comparison with normal weight women, obese women have a lower intention to breastfeed,8,9 decreased odds of initiating breastfeeding,10–12 shorter breastfeeding duration, 13 and increased risk of premature cessation of breastfeeding.10,14 In a limited number of studies, the association between body mass index (BMI), gestational weight gain, and breastfeeding outcome has been the focus.12,15,16 The results diverge as two of the studies showed no difference in duration of breastfeeding in relationship to BMI and gestational weight gain,12,15 whereas a systematic review and meta-analysis, 16 found that excessive gestational weight gain was a risk factor for premature cessation of any breastfeeding, among overweight women as well as among obese women. In a few studies, social factors and breastfeeding have been investigated and the results show that the duration of breastfeeding varies depending on socioeconomic status, social factors, and healthy habits.13,17
The aim of this cohort study was to evaluate the association between possible covariates, with emphasis on maternal BMI, on exclusive breastfeeding and on total breastfeeding during the first postnatal year.
Materials and Methods
The study context and recruitment of participants
All data concerning women and children are registered in standardized antenatal, delivery, neonatal, and child health service records. Women with uncomplicated pregnancies are recommended to have eight to nine visits to a midwife and, if necessary, additional appointments with an obstetrician. The regular program during the child's first year of life consists of visits at 1–2 weeks of age, once a month from 1 to 6 months of age, and then at 8, 10, and 12 months of age. All data in connection to the controls are registered in standardized Swedish antenatal, delivery, neonatal, and child health service records.
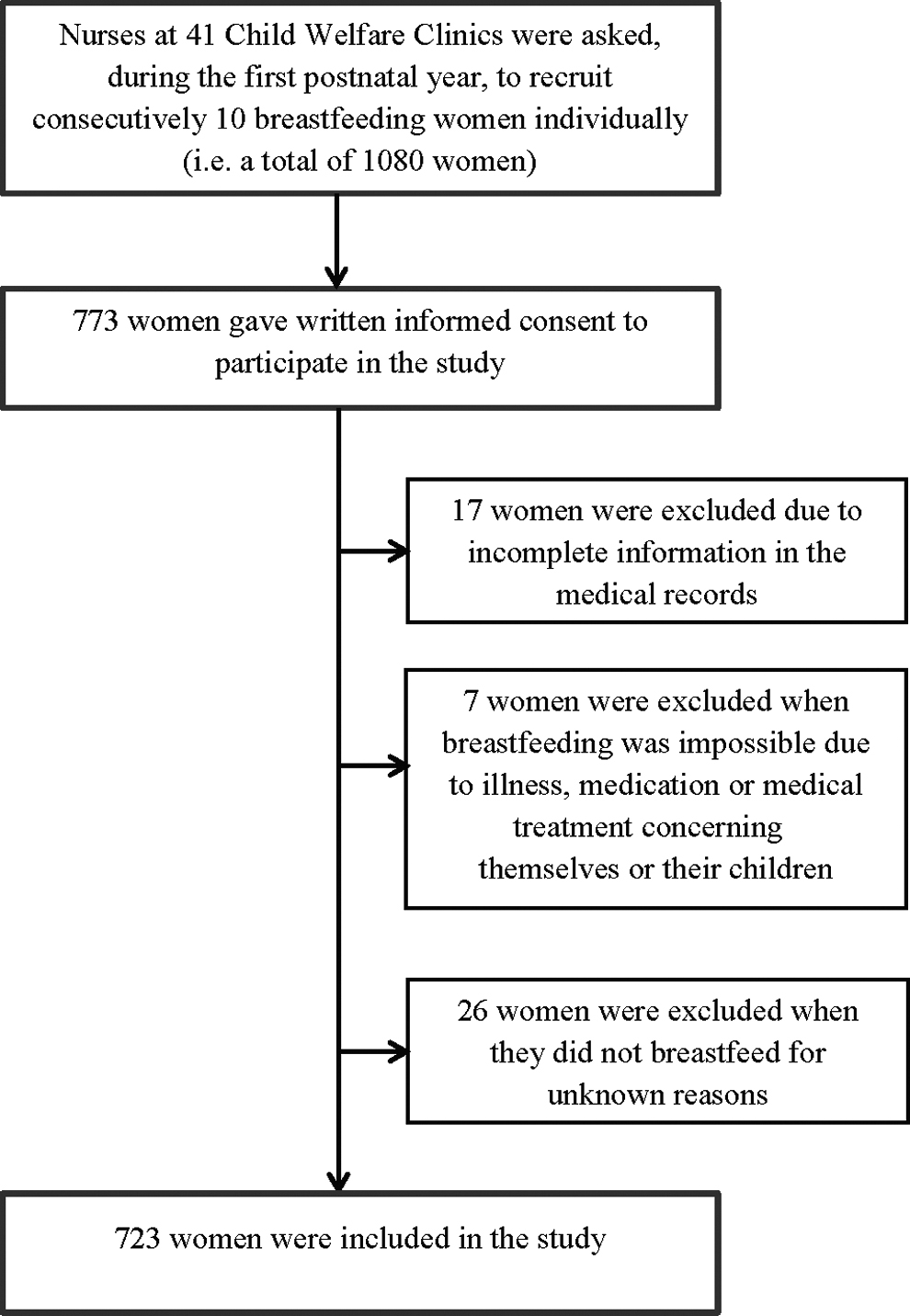
Nurses at 41 Child Welfare Centers (CWCs) in southeast Sweden were asked to individually recruit consecutively 10 breastfeeding women during the first postnatal year (i.e., a total of 1,080 women). Recruitment was performed between October 2015 and December 2016, and a total of 723 (66.9%) women were included in the study (Fig. 1). Women who did not understand Swedish or who were breastfeeding twins were excluded. Most of the participants were recruited during their first 6 months of breastfeeding. Written informed consent was obtained from all the women, who also gave permission to the main author (I.M.C.) to obtain relevant information from the pregnancy record (weight in early pregnancy (<15 weeks) and in pregnancy at week 37 or later, height, possible pregnancy complications), from the delivery record (possible delivery complications), from the neonatal record (gestational length, birth weight, the health status of the infant at birth, possible care at a neonatal intensive care unit), and from the child health service record (extent of breastfeeding from 2 to 12 months of age, possible care at pediatric hospitals). The data on marital status, occupation, educational level, tobacco habits, and health status were self-reported by the women on inclusion in the study.
Description of the population in the study.
Outcome measures
The extent of breastfeeding (exclusively breastfed since birth, fully breastfed in the last 7 days, predominantly breastfed in the last 7 days, partially breastfed in the last 7 days or not breastfed in the last 7 days) was documented in the record at the CWCs at each visit and further extracted for the purpose of this study. In this study, exclusive breastfeeding is defined to mean that the infant has solely been given breast milk since birth, whereas total breastfeeding means that the infant has had periods of exclusive breastfeeding as well as periods of partial breastfeeding. The duration of exclusive breastfeeding and total breastfeeding was analyzed in the present study.
Study variables
Based on measured weight and height data in early pregnancy (<15 weeks), BMI was calculated, and the WHO classifications of underweight (<18.5 kg/m2), normal weight (18.5 to <25.0 kg/m2), overweight (25.0 to 29.9 kg/m2), and obesity (≥30.0 kg/m2) were adopted. 18 In the group of underweight women, there were few participants; therefore, they were combined with the group of normal weight women.
Besides BMI, the following covariates were used in the analyses: age (the mean age at the inclusion in the study), parity (primiparous women or multiparous women), marital status (married/cohabiting with a partner or other family situation), education level (≤/>12 years of education), occupation (gainfully employed/parental leave/student or not gainfully employed), tobacco use (absent or present), incidences of complications during pregnancy and delivery (absent or present), gestational weight gain (defined as the difference between the first registered weight information in early pregnancy and registered weight information in pregnancy week 37 or later). The gestational weight gain in relationship to BMI in early pregnancy was classified according to recommended weight gain ranges provided by the Institute of Medicine 19 and in this study was categorized as inadequate, adequate or excessive.
The study was approved by the regional Ethical Review Board in Linköping, Sweden (Dnr.2015/45–31).
Statistical analyses
All analyses were performed using SPSS 26.0 (IBM, Armonk, NY). Statistical significance was defined as (two-sided) p ≤ 0.05. The Cox Proportional Hazard Model was used for investigating the effects of above-mentioned covariates on exclusive and total breastfeeding. Women who dropped out during the study period or who were still breastfeeding at the end of the study were defined as censored. Univariable analyses with exclusive or total breastfeeding as dependent variables, and covariates as independent variables were performed to assess the hazard ratio (HR) for cession of breastfeeding prematurely. In the multivariable analyses with exclusive or total breastfeeding as dependent variables and covariates with significant values in the univariable analyses as independent variables were performed to assess the HR for cession of breastfeeding prematurely.
The relationship between different BMI classes as well as the parity and the duration of exclusive breastfeeding were shown by using the Cox adjusted survival function.
Results
Initially, we performed interaction tests to assess whether the analysis should be stratified based on parity or based on gestational weight gain. The model with BMI and parity as the main factors together with their interaction effect and the model with BMI and gestational weight gain as the main factors together with their interaction effect showed no statistically significant interactions. Therefore, we refrained from stratifications.
A total of 773 women gave written informed consent to participate in the study. A total of 17 women were excluded because there was incomplete information on them in the medical records. Furthermore, seven women were excluded as breastfeeding was not recommended due to illness, medication, or medical treatment concerning themselves or their children. In addition, a total of 26 women were excluded as they did not breastfeed for unknown reasons. Finally, a total of 723 women participated in the study (Fig. 1). Characteristics of the participants are displayed in Table 1. To assess possible selection bias, we investigated sociodemographic differences between women who participated in the study and women who for unknown reasons did not breastfeed and did not participate in the study for that reason (Supplementary Table S1). Women who did participate in the study were younger, had a lower education level, and more often not gainfully employed, compared with the study women.
Characteristics of the Participants
The difference between registered weight at pregnancy week ≥37 and registered weight at the recruitment (<15 gestational weeks).
BMI, body mass index; SD, standard deviation.
The effects of covariates on the exclusive and total breastfeeding duration were investigated in univariable and multivariable regression analyses (Table 2). After adjusting for parity and age, obese women ran a higher risk of ceasing exclusive breastfeeding prematurely, compared with women with BMI <25.0 (HR = 1.38, p = 0.009). Furthermore, after controlling for BMI classes and age, multiparous women had a lower risk of ceasing exclusive breastfeeding prematurely than primiparous women (HR = 0.78, p = 0.009) (Table 2). Based on the results of the multivariable analysis in Table 2, Figures 2 and 3 show the adjusted survival analyses of the effects of BMI and parity on the duration of exclusive breastfeeding.
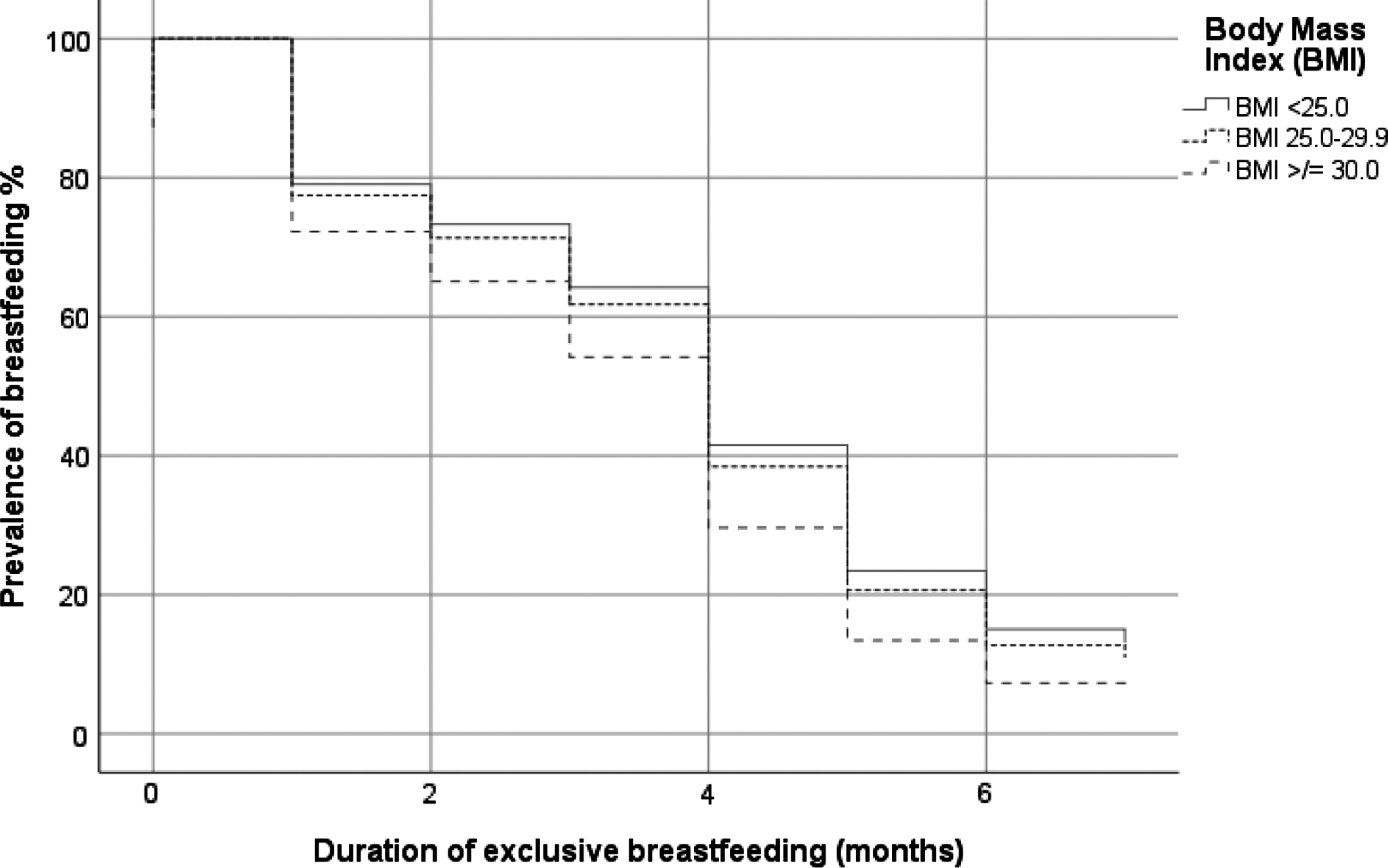
Cox survival function for adjusted analysis of the effects of BMI on the duration of exclusive breastfeeding. Assessed 12 months postpartum and adjusted for parity and maternal age. BMI, body mass index.

Cox survival function for adjusted analysis of the effects of parity on the duration of exclusive breastfeeding. Assessed 12 months postpartum and adjusted for BMI and maternal age.
Cox Proportional Hazard Model for the Effects of Covariates on the Exclusive and Total Breastfeeding Duration
Exclusive and partial breastfeeding.
Univariable analysis.
Multivariable analysis (including significant values in the univariable analysis).
HR.
CI (95%).
Overall p-value for all BMI classes (i.e., BMI <25.0, 25.0–29.9, ≥30.0).
Information on education level is missing in 10 women. Therefore, they are not included in the analysis.
Gestational weight gain according to recommendations of Institute of Medicine.
Overall p-value for all gestational weight gain levels (i.e., inadequate, adequate, excessive).
CI, confidence interval; HR, Hazard ratio.
Concerning the duration of exclusive as well as total breastfeeding, the multivariate analyses show that the risk of prematurely ceasing the breastfeeding decreased with increasing age (p = 0.028 and p ≤ 0.001, respectively) (Table 2).
Duration of exclusive and total breastfeeding according to BMI classes and parity are shown in Table 3. Women with BMI <30 had a longer median duration of exclusive and total breastfeeding than obese women. Concerning parity and exclusive breastfeeding, the median duration was the same in the groups of primiparous women and multiparous women, whereas primiparous women had a shorter duration of total breastfeeding, compared with multiparous women.
Duration of Exclusive and Total Breastfeeding According to Body Mass Index and Parity
Discussion
In this longitudinal cohort study, we evaluated the association between possible covariates on the duration of exclusive and total breastfeeding during the first postnatal year. This period was chosen since a slightly increased prevalence of breastfeeding at 9 and 12 months postnatally has been reported in Sweden during the last decade. 7 We found that in comparison with women with BMI <25, that obese women breastfed exclusively for a shorter period and had an almost 40% higher risk of ceasing breastfeeding prematurely, whereas multiparous women had just over a 20% lower risk of ceasing exclusive breastfeeding prematurely than primiparous women. Furthermore, our results indicate that the age of the women affects both the duration of exclusive and total breastfeeding. The risk of ceasing the breastfeeding prematurely decreased with increasing age.
Our results are both in line and in contrast with previous published studies. In an earlier study, we found that 5 months postnatally, there were more obese women who had ceased to breastfeed than underweight and normal weight women. 20 A Brazilian study 21 found that obese women exclusively or totally breastfed for a shorter period than normal weight women, whereas another Brazilian study 15 reported no differences in duration of breastfeeding according to prepregnancy BMI. Furthermore, an American study 22 suggested that women with BMI ≥25.0 were less likely to breastfeed exclusively at 6 weeks and at 6 months, compared with normal weight women. Neither the study by Tao et al. 12 nor the study by Bartok et al. 23 showed an association between maternal BMI in different classes and breastfeeding outcomes after adjustment for relevant covariates. A Spanish study found that the rate of cessation of predominant breastfeeding among obese women was higher than for other women in the cohort. 17 Similar results are reported in a Swedish study. 24 Primiparous women had a higher risk of terminating exclusive breastfeeding within 2 months postpartum, compared with multiparous women, and the univariable analysis indicated that women with BMI ≥25.0 had an increased risk of ceasing breastfeeding less than 2 months postnatally. 24 In our study, the median period of exclusive breastfeeding was 3 months or more, irrespective of BMI class, and concerning parity, the median period of exclusive breastfeeding was equal among primiparous women and multiparous women. In a systematic review and meta-analysis encompassing 17 studies, preferentially from western countries, the authors observed a positive association between prepregnancy excess maternal weight and cessation of exclusive breastfeeding. 25
We found that with increasing age, the risk of prematurely ceasing the breastfeeding decreased. This was in line with the results in the Spanish study, which showed that cessation of predominant breastfeeding was higher in young women, compared with women in older age groups. 17 On the contrary, our results differ from the Norwegian study, which reported that higher maternal age was negatively associated with exclusive breastfeeding 4 months postpartum. 13 Furthermore, Bjørset et al. 13 found that higher parity led to a higher likelihood of exclusive breastfeeding 4 and 5 months postpartum. This result agrees with our findings. Multiparous women had a lower risk of ceasing exclusive breastfeeding prematurely, compared with primiparous women.
The somewhat disappointing results concerning obese women in the present study are confirmed by findings in quantitative and qualitative studies. In a previous prospective study, we investigated the estimated extent and duration of the forthcoming breastfeeding and found that more multiparous women with overweight and obesity judged that the forthcoming breastfeeding would be partial, compared to multiparous women with BMI <25. 20 A meta-synthesis 26 showed that the obese breastfeeding women experienced ordinary difficulties to a greater degree. Medical interventions during childbirth might lead to complications and therefore possible separation from their infants, which negatively impacted breastfeeding. Furthermore, the difficulties might lead to doubt about their ability to breastfeed. 26 The obese women's breastfeeding challenges are described in another study. 27 They had to handle the technique of breastfeeding in a different way to normal weight women. For example, they had to adopt a particular body position so that the infant could take an optimal grip on the nipple. Another challenge was the exposure of the body when breastfeeding in public. In these situations, it was tempting to use formula instead of breastfeeding. 27 Both studies concluded that obese women requested breastfeeding support throughout the breastfeeding period. Staff at antenatal care clinics, maternity wards, and at the CWC should therefore strive to design and develop optimal breastfeeding information and breastfeeding care, in particular, for obese women.
Breastfeeding plays an important role concerning future health aspects of both the women and infants. It is well documented that breastfeeding benefits the health of the women as it can prevent breast cancer, improve birth spacing, and might reduce the risk of diabetes and ovarian cancer. 1 Infants who are breastfed for a longer period have been reported to have lower risk of infectious deceases, and a growing body of evidence suggests that breastfeeding might protect against overweight and obesity later in life.1,28–31 Therefore, the need to encourage breastfeeding cannot be emphasized enough.
The decision on whether or not to breastfeed and the outcome of breastfeeding can be crucial for future breastfeeding choice. Da Vanzo et al. 32 suggest in their study that women often repeat the feeding method they used with their first infant with later children. Women who breastfed their first infant are likely to breastfeed a later infant, and those who did not breastfeed the firstborn, are unlikely to breastfeed a child born later. However, if the breastfeeding experience was of short duration or was perceived to be unsuccessful or unsatisfactory, the women are less likely to breastfeed a child born later. 32 These results indicate the importance of providing careful support for obese primiparous women during pregnancy as well as postnatally. Rollins et al. 4 discuss the need for interventions to increase the global breastfeeding prevalence and conclude that when relevant interventions within different areas are achieved adequately, breastfeeding practices are responsive and can improve rapidly. Concerning the area of health care services, several interventions are included in the concept of the Baby Friendly Hospital Initiative. 33 Individual counseling, group education, support from specially trained health staff, immediate breastfeeding support at delivery, and breastfeeding management have been shown to increase the prevalence of exclusive or any breastfeeding up to 6 months postnatally. 4 It is possible that supportive interventions designed for obese pregnant and postnatal women may increase the prevalence of exclusive or total breastfeeding. The antenatal breastfeeding information and education should be tailored to prepare the obese woman and her partner for the forthcoming task, and furthermore, the continuum of care, from antenatal care to the child health service, should offer a supportive atmosphere to protect and promote breastfeeding.
This study has both strengths and limitations. All data concerning primary outcome were extracted from medical records. Only sociodemographic data were self-reported. This is, as far as we know, one of the few studies to evaluate the association between several possible covariates on breastfeeding duration during the first postnatal year. However, there are certain limitations. We had no information concerning the health status of the women and the infant at the time of data collection. It is therefore possible that there were reasons for ceasing breastfeeding associated with diseases of the mother or the infant. When interpreting the results, one ought to keep in mind the differences between the study women and women who for unknown reasons did not breastfeed and did not participate in the study for that reason. In addition, we had no information about race or ethnicity. It is possible that breastfeeding traditions might differ between ethnic groups. All data in the medical records were registered by the staff at the antenatal care clinics, hospitals, and CWC. Despite the existence of guidelines on how to document optimally, it is possible that differences within the staff group concerning medical registration occurred (information bias). However, these putative errors are unlikely related to exposure covariates or outcomes.
Conclusion
Compared with women with BMI <25.0, the duration of exclusive breastfeeding was shortened among obese women, and they had a higher risk of ceasing the exclusive breastfeeding period prematurely. Multiparous women ran a lower risk of ceasing the exclusive breastfeeding period prematurely than primiparous women. Regarding both exclusive and total breastfeeding, the risk of prematurely ceasing the breastfeeding decreased with increasing age.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.