
Abstract
Purpose:
This study aims to achieve a better understanding of the trend of maternal milk macronutrient levels by analyzing protein, lipid, carbohydrate, and energy content of the breast milk and investigate the possible confounders of macronutrient content during the first 4 weeks of lactation to meet the specific needs of babies, guide optimum fortification of maternal milk.
Patients and Methods:
Breast milk from 39 mothers who had delivered preterm infants and 21 mothers of term infants were collected longitudinally for the first 4 weeks of lactation. Fresh milk samples were obtained on day 3, 7, 14, and 28 of lactation. The samples are analyzed using mid-infrared milk analyzer (MIRIS Human Milk Analyzer, HMA; Miris AB, Uppsala, Sweden).
Results:
Colostral milk protein concentrations of mothers of both preterm and term infants were significantly higher and the protein content of the samples decreased in time, according to the week of lactation during the study period. In contrast, fat, carbohydrate, and energy content were lowest in the colostral milk in both groups. When preterm and term milks were compared, fat and carbohydrate levels on 28th day and energy levels on 14th and 28th days were significantly higher in term milks, whereas no difference in protein contents were observed between the two groups on each time period. Mode of delivery was found to have statistically significant correlation with protein content of the milk.
Conclusion:
This longitudinal study revealed significant changes in analyzed macronutrient contents of mother's milk over the first 4 week period.
Introduction
Human breast milk is the ideal nutrient for survival, growth, and development of human infants, due to its unique combination of essential nutrients and a variety of bioactive factors.1,2 Exclusive breastfeeding for the first 6 months of life and continuing breastfeeding till 2 years of life or beyond is recommended by many different associations, groups, or organisations and this approach is adopted by many countries and nations. 3
There are many studies conducted in different ethnic groups and populations.1,3–11 According to the data of some of these studies, milk macronutrient composition appears to be independent of maternal diet and maternal anthropometric measures.6,11,12 Milk composition has been shown to change over the course of lactation that is reflecting developmental maturation of the lactating breast or differences in nursing frequency. 13 Colostrum is the milk that is secreted right after birth during the first 5–7 days, transitional milk is the one secreted between day 5 and 15 and mature milk is the milk secreted between days 15–20. 14
Human milk analysis for a more precise and individual information about human milk composition, which is possible to perform by bedside devices, has the potential to improve the nutrition care of high-risk newborns. Equipment to analyze human milk in a rapid and precise manner is available, and the technology is rapidly evolving.15–17 A baby's own mother's milk is the most unique and ideal nutrition for a baby. With the help of these devices, it has become possible to investigate the possible changes in composition of human milk according to the level of prematurity, day and stage of lactation.3,5,14 Rassin et al. showed that preterm human milk contained higher protein and lower carbohydrate levels. 18 In another study, nitrogen content of preterm human milk was higher during the first 3 weeks after delivery. 19 On the other hand, there are several studies that demonstrated no difference in protein, energy, carbohydrate, and lipid levels between preterm and term infants. 20 There are many conflicting results in the literature on this subject.5,21
In clinical practice, most of the clinicians, institutions, and guidelines recommend routine fortification of human milk to meet the increased nutritional demands of the preterm infants.22,23 However, because of the gastrointestinal immaturity of these babies, it is important to investigate whether the content is appropriate especially before fortification.4,24
Thus, the primary aim of this study was to investigate the differences between the term and preterm human milks during the first 4 weeks of lactation and their possible confounders.
Materials and Methods
A total of 60 lactating mothers in babies were recruited to the study. Thirty-nine of them had preterm and 21 had term infants. Their babies were followed up in Neonatal Intensive Care Unit of Adnan Menderes University Hospital between January 2015 and September 2016. Milks of mothers who did not supply appropriate milk sample during the planned time interval, who had history of smoking, alcohol usage, or substance abuse, or the babies with severe feeding intolerance and stayed on total parenteral nutrition for a prolonged duration, or without an exact gestational age or deceased during the study period were excluded. Milk samples were collected by hand expression or manual milk pump, from either right or left breast, before infant feeding, between 8 and 10 AM on days 3, 7, 14, and 28 of lactation. These specific days are chosen as they are known to reflect colostral, transitional, and mature milk properties. Considering the foremilk and hindmilk difference, each time, the milking process is continued until no more milk is coming from that breast. Fresh milk samples were analyzed in 2 hours after collection. To minimize measurement errors due to heterogeneity of the fluid, milk samples were processed with homogenizers before analysis. The samples were analyzed for macronutrient contents, using mid-infrared milk analyzer (MIRIS Human Milk Analyzer, HMA; Miris AB, Uppsala, Sweden).
Statistical analysis was performed with SPSS software version 18.0 (SPSS, Inc., Chicago, IL). For hypothesis testing involving quantitative variables, parametric and nonparametric methods (t-test or Mann–Whitney test, respectively) were used as appropriate after ascertaining normality of distribution via the Kolmogorov–Smirnov or Shapiro–Wilk tests. The chi-square test, Fisher's exact test, odds ratios, and 95% confidence intervals were used to assess the relationship between categorical variables. In all tests, p-values <0.05 were considered statistically significant. Between-group comparisons were performed with Kruskal–Wallis tests with the Mann–Whitney U test adjusted by Bonferroni correction. Within-group comparisons of pre- and postintervention measurements were performed with the Wilcoxon signed-rank test. Differences between groups were assessed by using the Friedman test and analysis of variance.
This study was performed after being approved by the Adnan Menderes University Hospital Ethical Committee and conducted concurrent with Declaration of Helsinki Principles. All donors provided written inform consent before participating in the study.
Results
A total of 60 lactating women were recruited to the study. Twenty-five of the babies were girls and thirty-five of them were boys. Thirty-nine of the women had given birth prematurely with mean gestational age 29.7 ± 3.0 weeks and birth weight 1451 ± 479 g. There was no difference between the groups regarding gender distribution (p = 0.553) (Table 1). Totally 21 mothers with term babies with mean gestational age of 38.0 ± 1.1 weeks and birth weights 3041 ± 470 g were recruited to the study. Demographical characteristics of the babies were given in Table 1. No correlation between maternal age and milk protein, lipid, carbohydrate, and energy content was observed (p = 0.115, r = −0.102; p = 0.035, r = 0.035; p = 0.021, r = −0.149, p = 0.719, r = 0.023; respectively). Sixteen of the babies were born via normal vaginal delivery whereas 44 of them were born via Caesarean section (C/s). Regarding delivery route, protein content of the milk of mothers who delivered their babies via C/s was significantly higher compared to mothers who gave birth via vaginal delivery (1.794 ± 0.848; 1.543 ± 0.514 g/dL respectively; p = 0.021). Thirty-three percent of the mothers were primary school, 19% of them were high school, and 8% of them were university graduates. No correlation between maternal educational status and milk macronutrient content (protein, lipid, carbohydrate, energy) was observed (p = 0.413, p = 0.588, p = 0.570, p = 0.799; respectively). Similarly, no correlation between and milk macronutrient and energy content and maternal area of residence (urban/rural) was seen (p = 0.110, p = 0.379, p = 0.101, p = 0.400; respectively).
Demographic Characteristics of the Groups
NVD, normal vaginal delivery.
When macronutrient contents of maternal milks of preterm and term babies were compared regarding day of lactation, protein content was seen to decrease in time in both groups (p < 0.001, p < 0.001; respectively) but when the two groups were compared on each different time period, no statistically significant differences were found on 3th, 7th, 14th, and 28th days (Table 2 and Fig. 1). On the other hand, lipid and carbohydrate contents of both preterm and term milks were seen to increase in time, however, the increase in lipid content in preterms was not statistically significant (for lipids; p = 0.056, p < 0.001; respectively and for carbohydrates; p < 0.001, p < 0.001; respectively). While no differences between the two groups were observed on 3th, 7th, and 14th days regarding lipid and carbohydrate contents, on the 28th day lipid and carbohydrate contents of term milks were significantly higher than the preterm milks (p = 0.001, p = 0.005; respectively) (Tables 3, 4 and Figs. 2, 3). When preterm and term maternal milk energy contents were compared regarding day of lactation, statistically significant increase in this content is seen in time, in term milks but not in preterm milks (p < 0.001, p = 0.026; respectively). No significant differences were observed in between the two groups on 3th and 7th days but on 14th and 28th days, term milks had significantly higher energy levels (p = 0.029, p < 0.001; respectively) (Table 5 and Fig. 4).
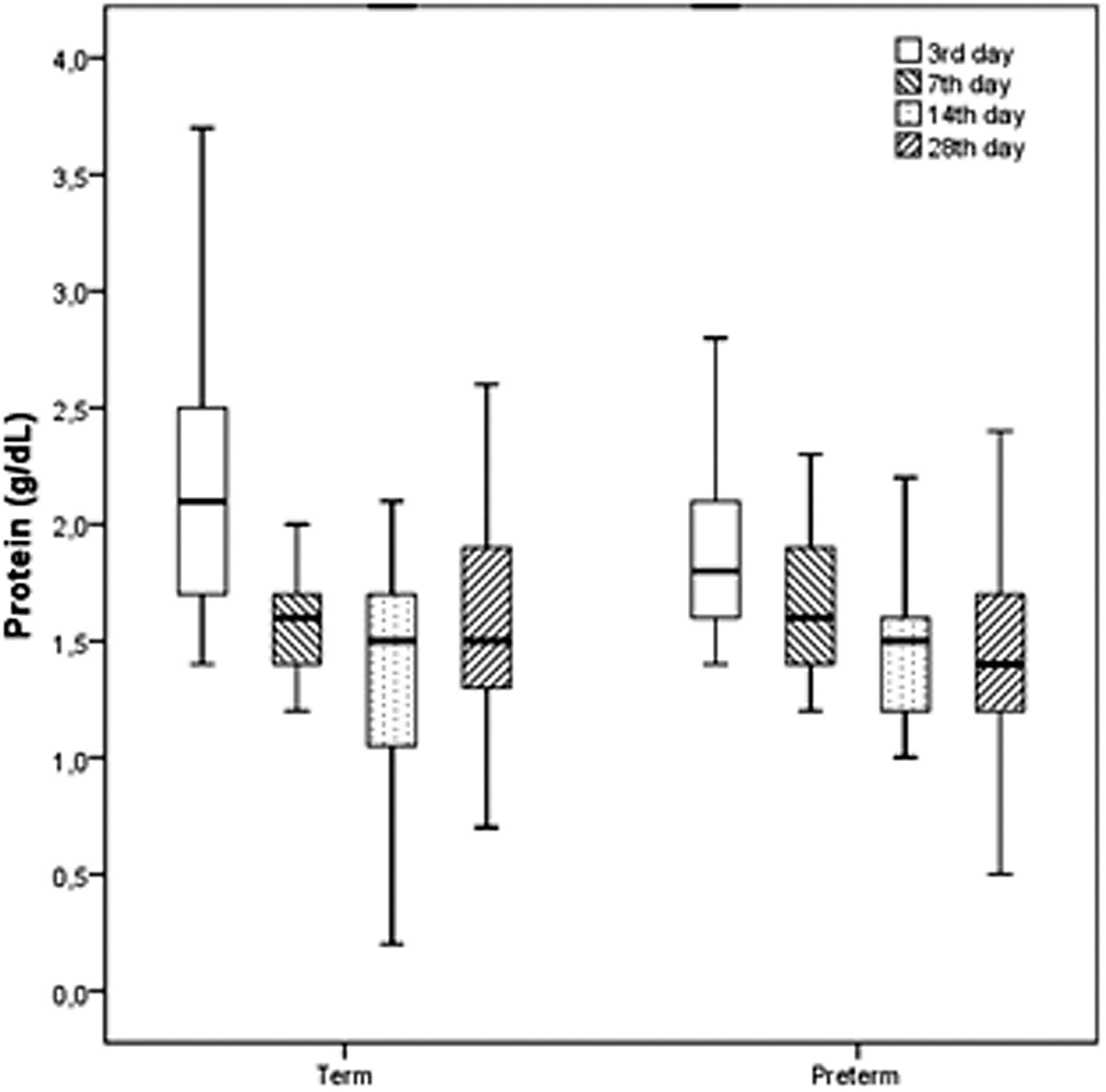
Protein trend of human milk over the first month.
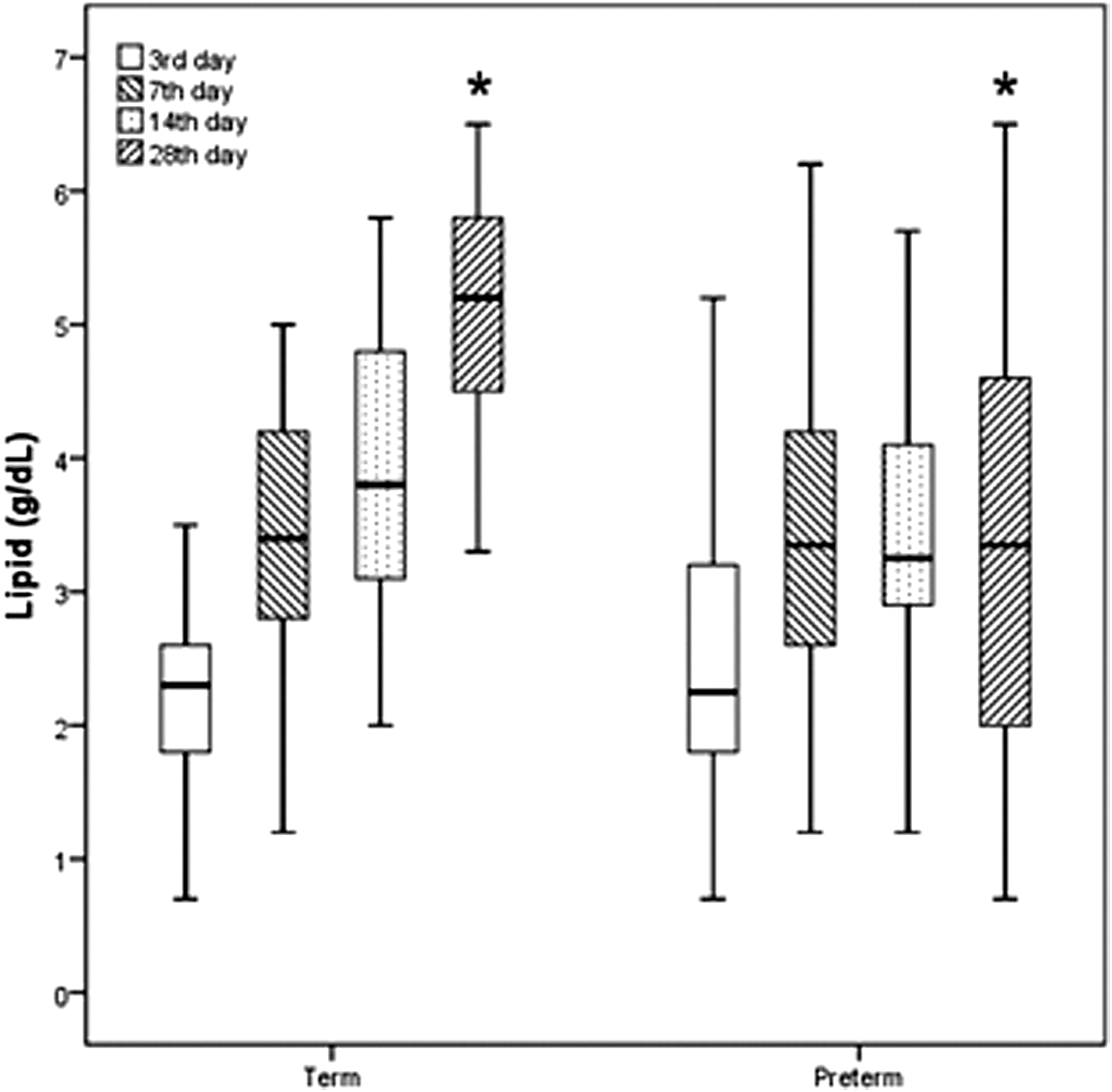
Lipid trend of human milk over the first month. *p < 0.05.
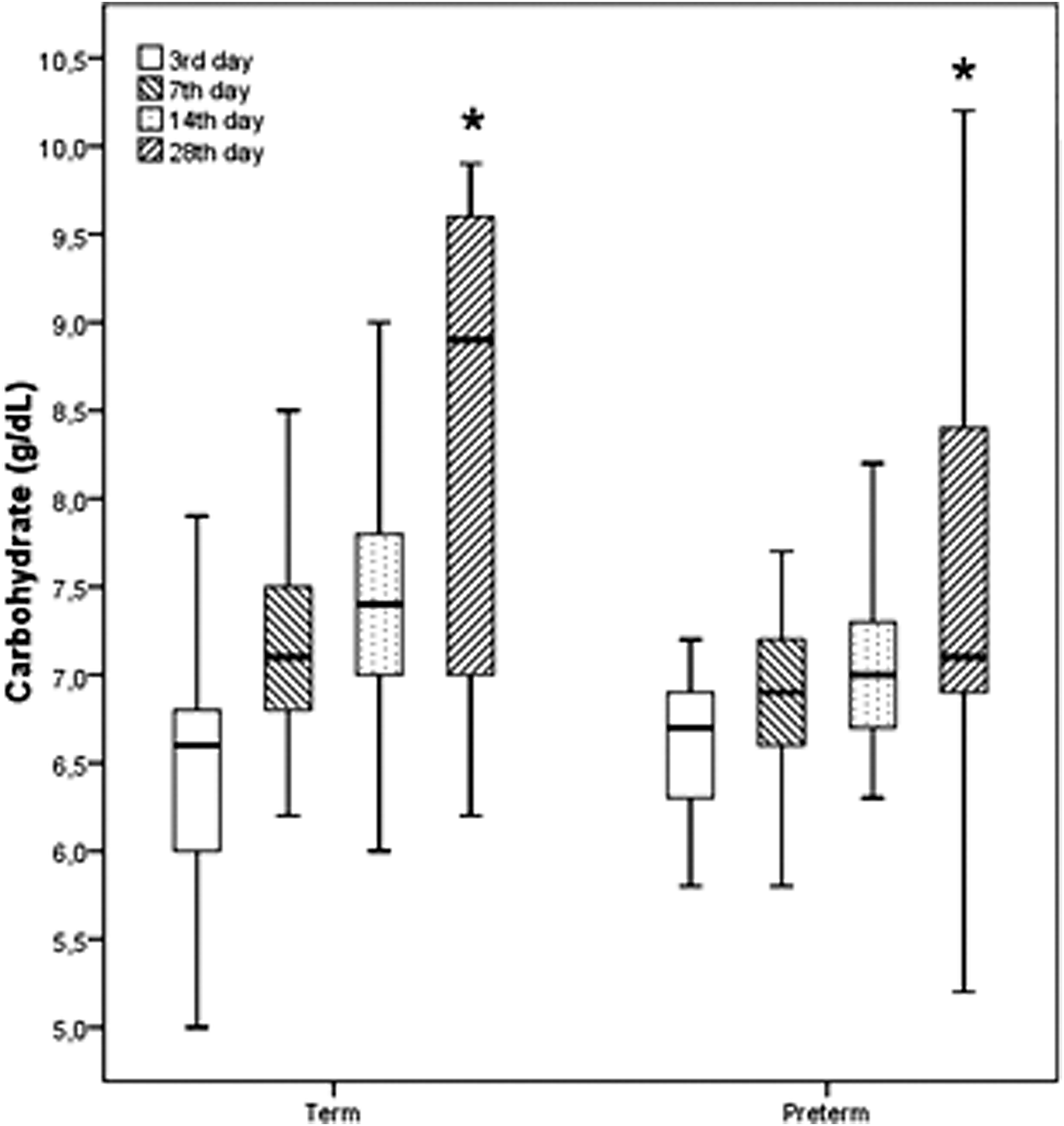
Carbohydrate trend of human milk over the first month. *p < 0.05.
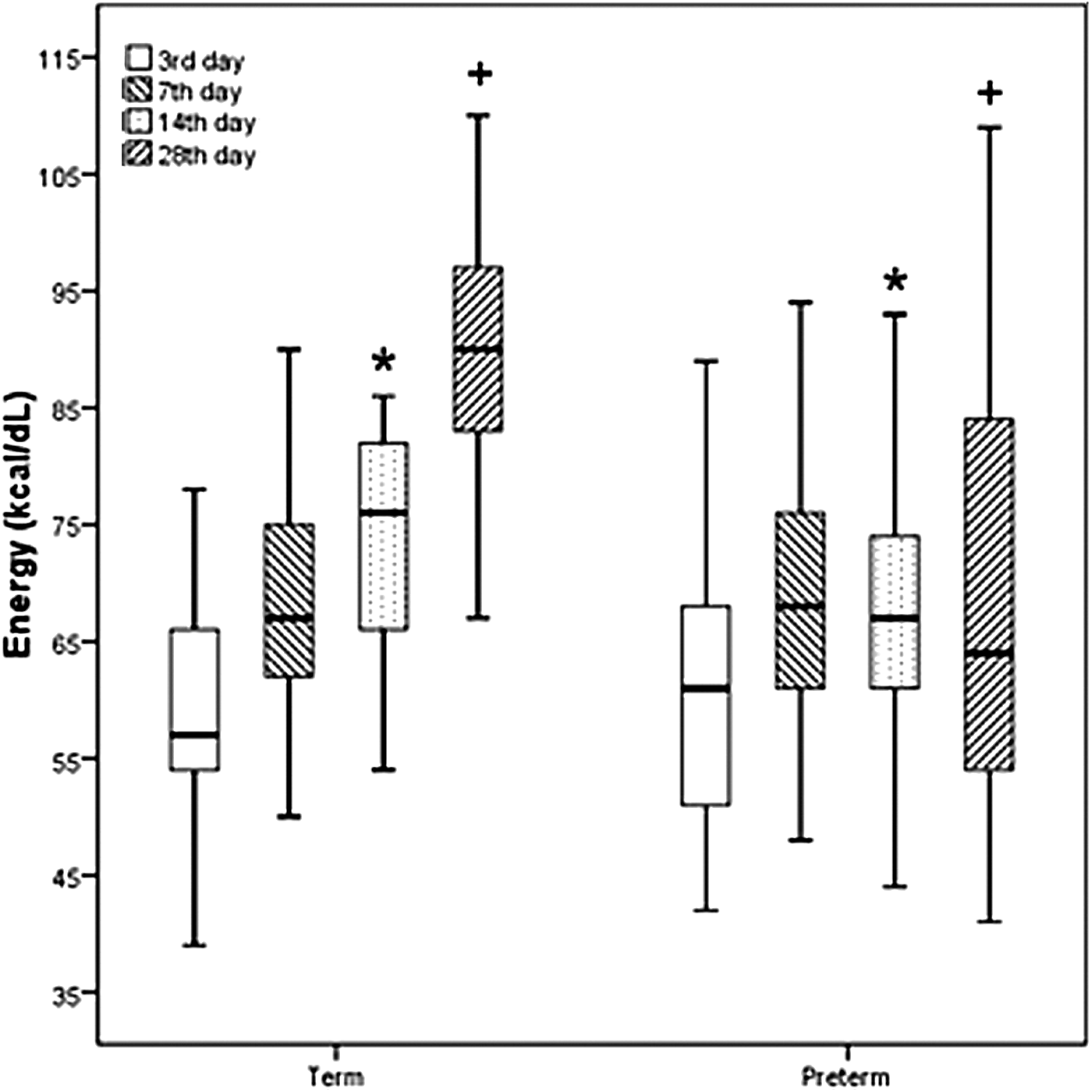
Energy trend of human milk over the first month. *, + p < 0.05.
Protein Content with Respect to Postnatal Age
Data are given as median (25–75 percentile).
Lipid Content with Respect to Postnatal Age
Data are given as median (25–75 percentile).
Carbohydrate Content with Respect to Postnatal Age
Data are given as mean ± standard deviation.
Energy Content with Respect to Postnatal Age
Data are given as mean ± standard deviation.
Discussion
As human milk composition varies and easy access to bedside human milk analysis process that serves as a rapid, easy, and safe way of determining the milk content has become reality, interest in an individualized and targeted approach to human milk fortification is increasing. 15 It is shown in many studies that protein content of maternal milk is decreasing and lipid and energy contents are undergoing several changes in time especially during the first 4 weeks of lactation.5,25,26
In accordance with the results of previous studies, we confirmed that protein content of human milk decreased gradually in time.3,4,26–28 On the other hand, when preterm and term milks were compared at different time points during the first 4 weeks of lactation, no significant difference was seen in between the two groups regarding protein content. While these results were compatible with Paul et al. 20 and Hsu et al.'s findings, they were in contradiction with the results of the studies that found higher protein contents in preterm milks compared with the term milks.4,5,14,29,30 Protein levels in our study varied between 1.2–2.1 g/dL in preterms and 1.0–2.6 g/dL in terms while both higher and lower levels are reported in the literature. 28 With the results of our study, considering the high turnover rate and increased protein demands of preterm babies, the importance of fortification of mother milks of these babies is once more emphasized.
When mother milks were analyzed for carbohydrate levels, compatible with the previous studies, concentration of this macronutrient was found to increase in time, in both groups.4,25,27 But besides, in our study, 28th day term maternal milks were found to have significantly higher carbohydrate levels compared to the preterms. The mean carbohydrate content in our study varied from 6.3 to 8.4 g/dL and these results are consistent with previous studies in the literature. 28 In previous studies, both higher carbohydrate concentrations at all time points in term milks 5 or similar carbohydrate levels in term and preterm milks had been reported.4,31 The discrepancy between previous findings and those of the present study regarding protein and carbohydrate content might be due to ethnic differences, nutritional status of the mother, sample size differences or variations in sample collection methods.
In our study, lipid levels were found to increase in time in both groups and no differences in lipid levels were found between the two groups on day 3, 7, and 14. Similar to carbohydrate levels, 28th day term maternal milks were found to have significantly higher lipid levels compared with the preterms. The measured lipid content in our study varied between 1.7 and 5.9 g/dL. Kreissl et al. 28 measured lipid content ranging between 1.1 and 6.1 g/dL, and the other studies in the literature showed similar results. Results of previous studies are quite variable regarding lipid trends. There are articles reporting increase in lipid levels in time but finding always higher levels in term milks,5,32,33 increase in lipid levels but finding no difference between term and preterm milks,4,5,20,31 or finding neither change in lipid levels in time nor difference between the two groups. 29 Lipid content of human milk is known to be the most variable macronutrient. 3 It is shown to be affected by the diet of the mother, hind- or fore-milk, daytime/nighttime feeding, and storage conditions.34–37 Due to all these prior knowledge, in our study, for standardization purposes, maternal milks were obtained from all the participants in the morning, at the same hour of the day, from the same breast, until that breast is completely empty and the samples were homogenized due to heterogenic nature of the milk. Differences in results of many studies were attributed partially to sampling differences in different studies.
In the present study, energy content of maternal milk is shown to increase in time without a difference between the two groups on day 3 and 7. But higher levels of energy content are observed in term milks on day 14 and 28 (75.7 and 87.9 kcal/dL respectively). On the other hand, preterm milks contained 67.5 and 69.7 kcal/dL of energy on these days, which is concordant with several studies in the literature but slightly lower than the reported value in a meta-analysis.28,38,39 This result is attributed to previously detected more significant increase in both lipid and carbohydrate levels in term milks by time. In another previous study, mature milk was found to have higher energy content compared to colostrum and later periods of lactation like 4–5 or 5–6 months. 3
In contradiction to the study conducted by Dizdar et al., our analysis revealed higher protein content in milks of mothers who delivered their babies by C/s. 6 But different from our study in which we studied both preterm and term milks at four different time periods of lactation, they analyzed only colostral milk samples of term babies. This difference in results may be attributed to difference in sampling periods between the two studies, relatively small sample size of our study, high C/s rate of our hospital, which is a referral hospital for high-risk pregnancies, and having both preterm and term milk samples analyzed together in our study. In another study, the investigators found that C/s delivery was a quite strong risk factor for increased fat content and decreased carbohydrate content in human milk and this difference persisted at least 3 months. This was attributed to hormonal activity induced by labor and uterine contractions. 7 In our study no correlation between type of delivery and milk lipid and carbohydrate contents were observed.
One of the limitations of our study is that body mass indexes of mothers were not calculated and taken into consideration. Besides, the mothers were not on a standard diet throughout the study period. Another limitation is that total milk volume of each mother, which might pose a potential influence on the results is not analyzed. Besides, possible relationship between milk macronutrient content and growth patterns of babies or clinical impact of variations in macronutrient content is also not investigated in our study.
It is crucial to investigate the differences in macronutrient contents of maternal milk and its possible confounders due to the unique composition of this miraculous nutrient with its many essential aminoacids, fatty acids, and lactose that are important for healthy growth of a baby. With the results of all these studies, a better understanding of the needs of babies in special circumstances, development of infant formulas that will be used in case of maternal milk insufficiency, and optimum fortification of maternal milk may be possible. For this reason, with the help of current standardized methods, further investigations in different ethnic groups with larger sample sizes may help to reveal more precise trends in maternal milk macronutrient contents of both preterm and term babies and guide health care providers to meet specific needs of babies for a healthy growth and development.
Conclusion
This longitudinal study revealed significant changes in analyzed macronutrient contents of mother's milk over the first 4-week period. Macronutrient contents other than protein component were found to vary regarding the time of delivery. By using bedside, rapid, and reliable milk analyzing devices, it has become possible to investigate the differences in macronutrient contents of maternal milk and its possible confounders due to the unique composition of this miraculous nutrient. Further investigations in different ethnic groups with larger sample sizes may help to reveal more precise trends in maternal milk macronutrient contents of both preterm and term babies and meet specific needs of babies for a healthy growth and development.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.