
Abstract
Background:
Postpartum mothers express and store breast milk using a hospital-grade pump and manufacturer-specific kit (flanges, bottles, tubing, valves, and membranes). After hospital discharge, mothers may attempt to interchange kits from different manufacturers. The objective of this study is to determine whether pump performance is affected by the use of a different manufacturer's kit.
Materials and Methods:
Suction pressure was tested using kits and six pumps from three manufacturers (Ameda, Medela, and Spectra). Pump settings (speed and vacuum strength) simulated maximum, minimum, and commonly used median settings. Suction pressure (mmHg) was measured using an analog gauge and repeated six times for each pump-kit combination. Measurements were compared using repeated measures analysis of covariance (ANCOVA) to determine whether kit was an independent predictor of suction pressure.
Results:
The kit type was a significant independent predictor (p < 0.05) of suction pressure for all at medium vacuum strength and many at maximum and minimum vacuum strengths. Upon further analysis interchanging kits resulted in both significantly increased and decreased suction pressures compared to the manufacturer-specific kit.
Conclusion:
Breast pump kits generate variable suction pressures when interchanged between pumps from different manufacturers. Interchanging combinations of kits and breast pumps could potentially lead to low milk expression due to ineffective suction pressure or increased discomfort from excessive pressure. The results of this study emphasize the importance of maternal education regarding the use of manufacturer-specific kits and breast pumps.
Introduction
Lactating mothers commonly use breast pumps to allow for regular human milk expression and collection despite separation from their breastfeeding infant.1,2 Most women use an electric breast pump and are provided with a compatible equipment kit from the same manufacturer. 3 Kits contain breast pump tubing, breast shields (also referred to as flanges), valves with diaphragms, and collection bottles. They are designed by the manufacturer to be used with their matching breast pump model to provide optimal milk expression and comfort. 4 The tubing, valve, and diaphragm create the vacuum suction pressure that is required to drain the breast. The volume of milk expressed by the breast pump is determined by the vacuum suction pressure and the cycle frequency generated by the pump and the amount of breast fullness. 4 Poor suction pressure can limit milk expression leading to early termination of breastfeeding.4–7 Extreme suction pressure can cause discomfort and breast injury and affect long-term breastfeeding success.8–11 Despite manufacturer recommendations, breastfeeding expert advice and differences in pump design, we observed that some women interchange kits between different manufacturers of breast pumps. Currently, there are no studies that evaluate whether interchanging the brand of kit impacts breast pump performance. To investigate this, we determined whether electric breast pump suction pressure is affected by the kit brand.
Materials and Methods
Six common double electric breast pumps encompassing three manufacturers were assessed. Three pumps were multi-use or “hospital-grade” from Ameda: Platinum®, Sister Maja Breast (SMB)® and Elite®. The other three pumps were personal use or “home-grade”: Medela Pump In Style®, Ameda Purely Yours®, and Spectra S2®. Three kits for each brand (Ameda, Medela, and Spectra) were used to test each pump at various cycles per minute (CPM) and vacuum strengths. Each brand of kit was compatible with its brand of pump regardless of model. For example, the Ameda kit is compatible with all Ameda pumps. The kits were exclusively used for testing; a lactating mother had never used them. The manufacturer kit was considered the control kit with the null hypothesis being that there is no difference between control and alternate kits.
Breast pump settings were determined based on published infant breastfeeding oral suction pressures and recommendations from International Board of Lactation Consultant Examiners certified lactation consultants. Breastfeeding infants generate an average oral suction pressure of 100 and 150 mmHg within 24 hours after a cesarean delivery or vaginal delivery respectively. 12 Lactation consultants recommend an initial vacuum strength setting of “medium” on all breast pumps that is then individually adjusted for comfort (C.M. Pawlowski, pers. comm.).4,13 Medium vacuum strength was defined as the setting on the breast pump vacuum pressure dial that is equidistant from the highest and lowest settings available. When measured in our experiments using the compatible breast pump and kit, the “medium” vacuum strength for each pump created a suction pressure between 100 and 150 mmHg, which is consistent with published values. Suction pressure was also measured at minimum and maximum vacuum strength for each pump to evaluate the variation in pressures across the breadth of available settings for each pump.
Breast pump speed was measured in CPM. With the exception of the Ameda SMB, which only had one speed setting, CPM varied for any given pump. We therefore analyzed each pump at its lowest, median, and highest CPM to mimic the multiple sucking rates an infant uses when breastfeeding. Infants latch and suck at a higher rate during nonnutritive sucking, or before milk let down. This was mimicked with a higher CPM. Infants then decrease their sucking rate to sustain a “maintenance phase” during nutritive feeding, which was mimicked with lower CPM.14,15
Each kit was assembled and connected to a breast pump according to the manufacturer instructions. The adapter contained in the Ameda kit was used to attach all three brands of kits to the hospital-grade pumps. When testing the home-grade pumps, the same adapter was only used to connect the Ameda kit to the Ameda Purely Yours Pump. An analog vacuum pressure gauge (product no. 617659; Ameda, Inc., Buffalo Grove, IL) connected to a rubber stopper was inserted into each flange to simulate normal occlusion of the shield by the maternal breast (Fig. 1). This is the same method in which our biomedical engineering department measures vacuum strength and ensures quality control for each pump within the hospital. It is the manufacturer's recommended method to assess vacuum strength for each pump (personal communication). The resultant suction pressure produced in mmHg was measured for each pump-kit combination. Six total measurements per combination of pump kit were recorded in a repeated measures format.
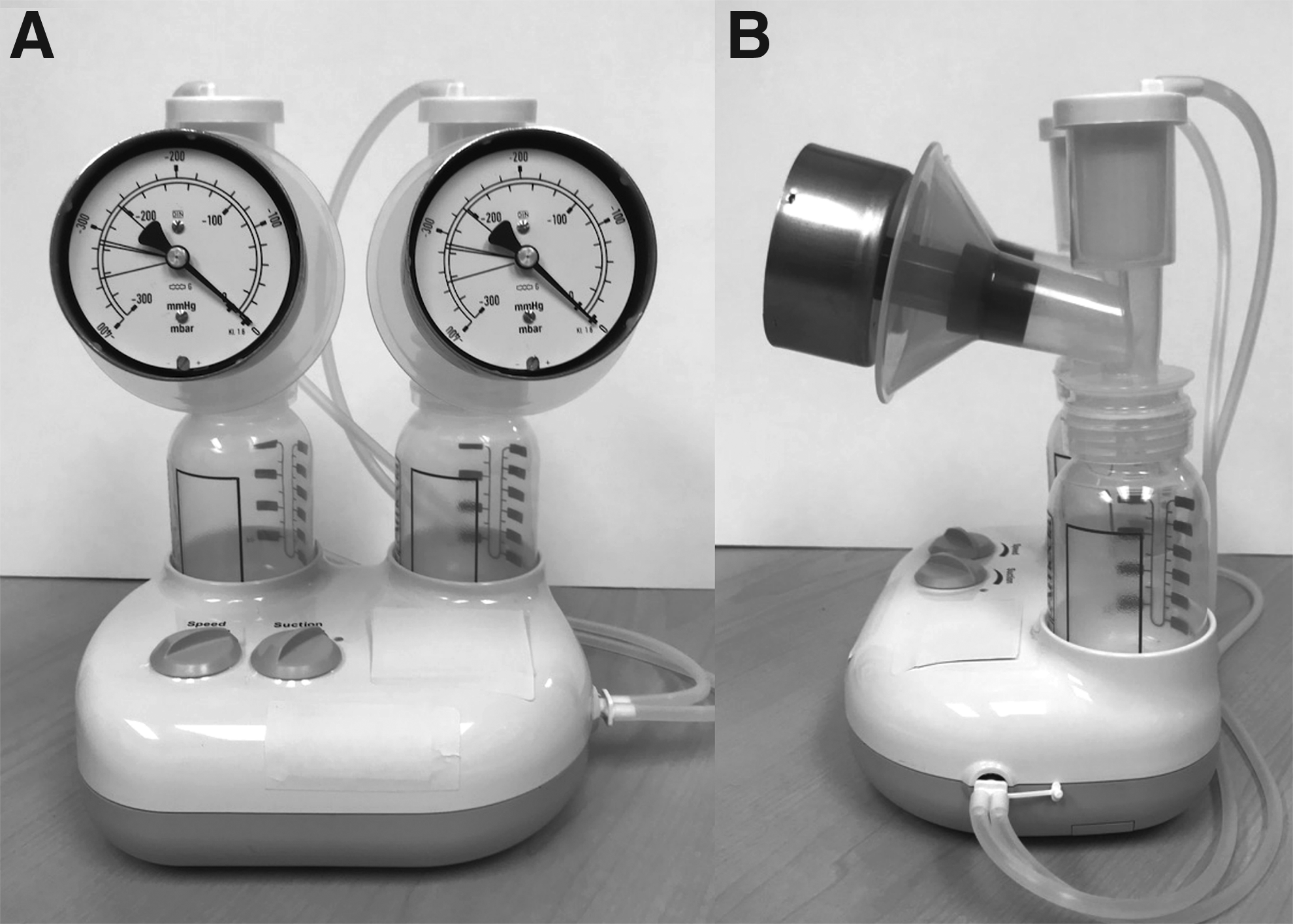
Front
Results were analyzed for differences by using a repeated measure analysis of covariance (ANCOVA) model to predict whether the kit was a significant predictor of suction pressure (software: SAS 9.4). The manufacturer designated kit for each brand was used as the control and compared to the two alternate kit brands. Post hoc analyses determined the significance of each pairwise comparison.
Results
In a repeated measures ANCOVA model where pressure is predicted by speed setting and the kit being used, kit type was a significant independent predictor (p < 0.05) of suction pressure for all pumps tested at medium vacuum strength as described in the methods. This was also true for many of the pumps at maximum and minimum vacuum strengths. Specifically, at maximum vacuum strength, kit type was a significant independent predictor of suction pressure in all pumps except the Spectra pump. In contrast, at minimum vacuum strength, kit type was an independent predictor of suction pressure with only the Ameda SMB and Spectra pumps. The mean fractional uncertainty for a set of six repeated measures was 4.0%, with a range of 0.8–12.7%.
Upon further analysis, using the medium vacuum settings with varying CPM, interchanging kits resulted in both significantly (p < 0.05) increased and decreased suction pressures compared to the manufacturer-specific kit in all the pumps except the Ameda Elite (Table 1). The changes in suction pressure were consistent despite variation in CPM settings for all pump-kit combinations tested.
Mean (Standard Error) Suction Pressure (mmHg) Using Medium Vacuum Strength with Variable Cycles per Minutes for Each Kit Type
The control kit as defined by the manufacturer recommended kit.
p < 0.05 compared to the control kit.
SMB, Sister Maja Breast.
Further analysis of maximum vacuum settings among hospital and home pumps also showed variability in suction pressures when used with an incompatible kit (Table 2). The authors note that some individual nonrecommended pump-kit combinations produced exceedingly high suction pressures that were >300 mmHg and unmeasurable by our methods when used with the maximum vacuum setting. This was observed when the Ameda SMB pump was used with both the Medela and Spectra kits and when the Spectra S2 pump was used with the Medela kit. For statistical analysis, the value 300 mmHg was used when the pressure exceeded the maximum pressure measured by the analog gauge.
Mean (Standard Error) Suction Pressure (mmHg) Using Maximum Vacuum Strength with Variable Cycles per Minutes for Each Kit Type
The control kit as defined by the manufacturer recommended kit.
The maximum measurable pressure by the tool used in this study was 300 mmHg. The value of 300 mmHg was used for statistical analysis for individual measurements in excess of the maximum pressure measured by the analog gauge.
p < 0.05 compared to the control kit.
Less variability in suction pressures was observed when kits were interchanged between hospital and home pumps at minimum vacuum settings. Only the Ameda kit-Spectra S2 pump combination produced a significant difference in pressure compared to the control (Table 3).
Mean (Standard Error) Suction Pressure (mmHg) Using Minimum Vacuum Strength with Variable Cycles per Minutes for Each Kit Type
The control kit as defined by the manufacturer recommended kit.
p < 0.05 compared to the control kit.
Discussion
In this study, we investigated whether the suction pressure, which is a determining factor in milk expression, was affected by interchanging different manufacturer kits with common electric breast pumps. Among most hospital and home electric breast pumps at settings most commonly used for maintenance of lactation, our results show that suction pressure is independently and significantly affected by the brand of kit. Moreover, interchanging kits provides variable differences in suction pressure—both higher and lower—rather than a consistent difference. Specifically, Spectra brand kits produced lower pressures when used with a different manufacturer's pump. In contrast, both Medela and Ameda kits produced higher suction pressures when used with a pump not recommended by the manufacturer. Kit type did not affect suction pressure with the hospital-grade Ameda Elite at medium vacuum settings. Similar variability in pressure was also observed at maximum vacuum strength among all the incompatible kit-pump combinations except the Spectra S2 pump. In contrast, there was minimal variability in suction pressure when pumps were tested using a minimum vacuum strength. Thus, interchanging kits may have unintended consequences on milk expression due to the variability in generated pump suction pressure.
Lactation is dependent on repetitive milk expression that empties the breast and results in release of prolactin and an increase in milk production. Breast pumps are designed to mimic infant oral suction pressure and suckling rate to empty the breast. 16 By frequently pumping, a mother who is separated from her infant can successfully maintain lactation and provide breast milk to her infant.16–18 However, low vacuum pump pressure can be ineffective at fully emptying the breast that can lead to lower total milk expression or delay the onset of lactation.5,7,13 Kent et al. showed that using less than the maximum comfortable vacuum pressure on an electric pump leads to decreased milk volumes. 13 Another report demonstrated that 39% of women were not able to express enough milk despite a working pump. 10 Decreased milk expression over time leads to termination of lactation. In our study, Spectra brand kits consistently produced significantly lower suction pressures when used with all but two nonmanufacturer recommended pumps at appropriate milk expression settings. If women interchange kits without adjusting pressures to fully express their milk, their total milk volume may decline and potentially affect their ability to maintain lactation long term.
In contrast to low suction pressures, we also found that Medela and Ameda kits consistently produced significantly higher suction pressures compared to the control kit at commonly used vacuum strength settings. McClellan et al. showed that mothers of infants who had stronger baseline intra oral vacuum strengths were more likely to experience persistent nipple pain with breastfeeding and was associated with lower milk intake by the nursing infants. 19 Similar to the mother-infant dyad, elevated breast pump pressures can also lead to nipple pain or breast injury resulting in decreased milk expression and early termination of breastfeeding.5,6,8,11,20 Specifically, Qi et al. found that 62% and 15% of lactating mothers report problems and injuries related to the breast pump and elevated suction pressures may contribute to this. 10 One of the most common reported problems was discomfort and/or pain; the three most common reported injuries were sore nipples, pressure bruise, and nipple injury. 10 In another report by Brown et al. that evaluated Medical Device Reports submitted to the United States Food and Drug Administration between 1992 and 2003, the most common patient problems associated with electric breast pumps were pain, soreness or discomfort, the need for medical intervention, and tissue damage. 8 The most common device problems were high suction and inadequate suction. 8 Our study highlights the importance of following manufacturer's recommendations regarding pump-kit combinations, thus potentially decreasing the risk of injury related to elevated pump suction pressures.
Full-term infants have sucking pressures that range between −50 to 197 mmHg. 4 However, electric breast pumps can produce suction pressures as high as −270 mm Hg. 4 Kent et al. showed that among 21 mothers who used an electric pump, maximum comfortable vacuum pressure varied and only half of the women could tolerate a pressure greater then −200 mmHg. 13 Although suction pressures measured in our study did not exceed −220 mmHg at a medium vacuum settings, we did observe that some nonrecommended manufacturer pump-kit combinations produced exceedingly high pressures that were unmeasurable (>−300 mmHg) when at maximum vacuum strength settings during some, but not all, of our individual recordings. This was observed with the Ameda SMB pump when used with both Medela and Spectra kits and with the Spectra S2 pump when used with the Medela kit. Because the maximum pressures generated by these pump-kit combinations were outside the range measured by the analog gauge used in this study, the pressures were capped at 300 mmHg for analysis and thus may underestimate the true differences in pressures. Future studies using a pressure gauge with a larger range would provide a more accurate measurement of the pressures generated at maximum vacuum strength.
Many lactating mothers rely on breast pumps to maintain milk expression when separated from their breastfeeding infant. The 2005–2007 Infant Feeding Practices Study II found that ∼85% of women will express milk during their infant's first year of life and 60% of them will use an electric breast pump. 3 With the passage of the Patient Protection and Affordable Care Act in 2010 and the increased emphasis on supporting breastfeeding during maternal-infant separation due to illness and employment, the number of women who have access to different models of breast pumps in diverse environments including home, work, and medical facilities will likely increase.3,18,21 Qi et al. found that most women learn to use a breast pump by either reading the manual or the Internet, watching a video, or learning on their own as opposed to in-person training. 10 Although manufacturers design the breast pump kits to be used exclusively with their product, it is unknown how many women may interchange the kits between different models of breast pumps. Our study showed that incompatible kits can both increase and decrease vacuum suction pressure when using equivalent pump settings, which could potentially result in either decreased milk expression or injury, respectively. Thus, educating women to use a kit with the recommended breast pump for optimal milk expression is important.
There were several limitations to our study. Our study was not performed in a clinical setting and milk expression was not measured among the different pump-kit combinations. Therefore, the results of this study cannot be fully extrapolated to clinical care. The effects of different pump-kit combinations on milk expression remain unknown and is an area in need of future study. In addition, the electric pump vacuum settings used in this study were based on infant oral sucking pressures and lactation consultant recommendations. During actual use, each woman determines the appropriate suction pressure based on individual comfort.4,16
Conclusion
In summary, electric breast pump suction pressure is independently and significantly affected by the brand of kit. Interchanging kits has the potential to negatively impact milk expression or increase the risk of pump-related injury. Women may interchange kits out of convenience and make assumptions that this will not affect the quality of the pump. Based on our findings, we suggest using the manufacturer's recommended kit with each pump. Breastfeeding women should be aware that if they choose to interchange the brand of kit between different pumps, the appropriate settings for the initial kit may no longer produce the same pressure, and this difference is variable depending on the electric pump and kit. Therefore, health providers should emphasize the importance of following manufacturer instructions and using compatible equipment with electric breast pumps to assist lactating mothers with breastfeeding success.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.